
Abstract
A novel intranasal formulation of azelastine HCl (AZE, an antihistamine) and fluticasone propionate (FP, a corticosteroid) in a single spray (MP-AzeFlu [Dymista®]) was studied in four randomized, double-blind, placebo-controlled trials of patients with seasonal allergic rhinitis conducted in the US. Study sites were distributed so that all major US geographic regions and the prevalent pollens within these regions were represented. Spring and summer studies included patients aged 12 years and older with allergy to grass and tree pollens. Fall studies enrolled patients with allergy to weeds, in particular ragweed. In addition, a study was conducted during the winter months in patients with allergy to mountain cedar pollen in TX, USA. Regardless of allergy season or prevalent pollen, MP-AzeFlu improved nasal symptoms of allergic rhinitis (AR) to a significantly greater degree than AZE or FP, two treatments that currently are recommended as the first-line AR therapy. MP-AzeFlu improved all individual AR symptoms and was significantly better than FP and AZE for nasal congestion relief, which is generally accepted as the most bothersome symptom for AR patients. The onset of action was within 30 minutes. MP-AzeFlu also provided clinically important improvement in the overall Rhinoconjunctivitis Quality of Life Questionnaire score and significantly improved ocular symptoms of rhinitis compared to placebo. Favorable characteristics of the MP-AzeFlu formulation as well as superior clinical efficacy make it an ideal intranasal therapy for AR.
Introduction
Seasonal allergic rhinitis (SAR) symptoms may be experienced by patients during spring, summer, fall, and winter depending upon sensitivity to the different prevalent pollens. It is important for an allergic rhinitis (AR) therapy to show consistent effect regardless of the prevalent pollens. This is particularly evident for large countries like the US.
AR is a major cause of morbidity, medical costs, and deficits in work, school, and leisure activities.Citation1 In the US, the prevalence of AR is now estimated at 60–90 million individuals or ~30% of the population, and the prevalence continues to increase at a steady rate.Citation2,Citation3 Global climate changes resulting in elevated levels of carbon dioxide, increased plant productivity, and increases in airborne pollen may account in part for the increased prevalence.Citation4 Under experimental conditions, it was shown that doubling the concentration of carbon dioxide in a controlled atmosphere resulted in a 61% increase in ragweed pollen production.Citation5
Shifts in the timing of allergy seasons due to climate change have resulted in increased peak pollen concentrations and annual pollen levels in Europe and the US, with the most widely documented expansion seen with the Juniperus species across the Central Plains and the southwest and western US.Citation4 Across the continental US from 2001 to 2010, the average peak pollen counts and the average daily pollen counts increased by 42% and 46%, respectively.Citation6 Regardless of the cause, the potential impact of climate change should be included in future assessments of the overall health burden of AR.Citation7
There has been a well-recognized need for new therapies to effectively treat seasonal allergies, especially for patients with more severe disease.Citation8 Despite the available therapies, prior to the introduction of MP-AzeFlu, large-scale longitudinal surveys of allergy sufferers have identified a continuing unmet need for treatments that provide rapid and sustained relief of AR symptoms and interventions that improve the overall quality of life of these patients.Citation8,Citation9
The clinical trial program for approval of a novel intranasal formulation of azelastine HCl (AZE, an antihistamine) 137 µg and fluticasone propionate (FP, a corticosteroid) 50 µg in a single spray (MP-AzeFlu, Dymista®; Meda Pharmaceuticals Inc., Somerset, NJ, USA) is summarized in this review. Clinical efficacy studies of MP-AzeFlu involving >4,000 patients were performed during a 20-month period in the US during the spring,Citation10 summer, fall,Citation11 and Texas mountain cedar allergy seasons in different geographical regions across the US.Citation12,Citation13
Clinical studies
An overview of the MP-AzeFlu clinical studies is presented in . Patients in the four efficacy studies (MP 4001 [Texas mountain cedar, Winter], MP 4002 [Spring], MP 4004 [Fall], and MP 4006 [Spring to Fall]) included males and females aged 12 years and older with a 2-year history of seasonal allergies and a positive skin prick test to a local seasonal allergen within the past year. Based on the study entry criteria, the qualified patients had moderate-to-severe SAR. The studies were randomized, double-blind, parallel-group, placebo-controlled, 2-week, multicenter trials conducted in the US, with study sites distributed so that all major US geographic regions and the prevalent pollens within those regions would be represented.
Table 1 MP-AzeFlu clinical studies
In study MP 4001, MP-AzeFlu was compared to com-mercially available AZE (Astelin; Meda Pharmaceuticals Inc.) and FP (Roxane Laboratories, Columbus, OH, USA), whereas in all other studies, MP-AzeFlu was compared to a noncommercially available AZE and FP. In these studies, the monotherapy comparators were reformulated in the same vehicle and delivery device as MP-AzeFlu.
The MP-AzeFlu clinical studies were conducted according to the guidelines and recommendations of both the US Food and Drug Administration and European Medicines Agency, and all efforts were made to ensure the safety of the patients in the studies.Citation14,Citation15 All the patients (or guardians) signed written informed consent before entering the study.
In all these SAR studies, efficacy was determined by the US Food and Drug Administration- and European Medicines Agency-specified primary efficacy end point: the change from baseline in patient-reported symptom severity based on the 12-hour reflective total nasal symptom score (rTNSS). Patients recorded their symptom scores in diaries twice daily, in the morning and again in the evening, each day of the 2-week study. Symptoms were scored on a 4-point scale, with 0 being symptom free, 1 being mild symptoms, 2 being moderate symptoms, and 3 being severe symptoms, so that 24 was the maximum daily score. A summary of the primary efficacy outcome in each of the SAR studies is shown in . A placebo-subtracted comparison of the differences between active treatment groups in each study is shown in .
Figure 1 A summary of primary efficacy results in the MP-AzeFlu clinical studies in patients with moderate-to-severe SAR (values shown are placebo subtracted).
Abbreviations: SAR, seasonal allergic rhinitis; LS, least-squares; FP, fluticasone propionate; AZE, azelastine HCl; TNSS, total nasal symptom score.
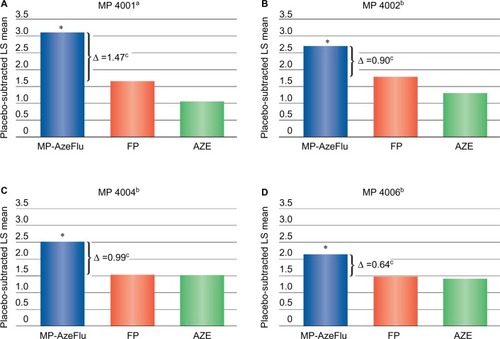
Table 2 Change from baseline in total nasal symptom scores in 2-week studies with MP-AzeFlu in patients with SAR
Other evaluations of efficacy included the change from baseline in: 1) total ocular symptom score (TOSS) with symptoms of watery eyes, itchy eyes, and red eyes; 2) time to onset of action; 3) individual nasal and ocular symptom scores; and 4) health-related quality of life using the Rhinoconjunctivitis Quality of Life Questionnaire (RQLQ).Citation16
Texas mountain cedar study (MP 4001)
Study MP 4001 was designed using commercially available AZE and FP as the active-control monotherapies.Citation12,Citation13 This design is in contrast to studies MP 4002, MP 4004, and MP 4006 in which MP-AzeFlu was reformulated and therefore not compared to commercially available monotherapy comparators.
During the 14-day study period, MP-AzeFlu reduced the rTNSS by 5.3 points from a baseline symptom score of 18.6. This reduction in symptom severity was statistically significant (P<0.001) compared to both active monotherapies (). As shown in , MP-AzeFlu significantly (P<0.05) improved the individual symptoms of nasal congestion, itchy nose, and sneezing compared to AZE, FP, and placebo. Runny nose was significantly (P<0.01) improved compared to AZE and placebo. MP-AzeFlu significantly improved the overall TOSS compared with FP and placebo.
Table 3 Change from baseline individual nasal symptom scores in 2-week studies with MP-AzeFlu in patients with SAR
MP-AzeFlu improved all individual ocular symptoms compared to AZE, FP, and placebo with the exception of watery eyes when compared to AZE. All active treatments resulted in significant (P<0.001) improvements from baseline in the RQLQ score. A clinically important change (defined as >0.5 units) relative to placebo was only achieved in the MP-AzeFlu group.
Spring study (MP 4002)
In study MP 4002,Citation10 MP-AzeFlu was compared with the reformulated AZE and FP and placebo. As shown in , for the primary efficacy variable, the improvement in the rTNSS of 5.5 points from a baseline of 18.3 with MP-AzeFlu was statistically significant compared to both reformulated FP (P=0.034) and AZE (P=0.002).
MP-AzeFlu significantly (P≤0.015) improved all individual symptoms of the rTNSS compared to placebo and reformulated AZE and significantly (P≤0.043) improved runny nose compared to reformulated FP (). MP-AzeFlu significantly (P<0.0001) improved the TOSS compared to placebo. Patients treated with MP-AzeFlu had statistical (P<0.001) and clinical improvement in the RQLQ score compared to placebo (P<0.001) and AZE (P=0.029).
Fall study (MP 4004)
In the fall study,Citation10,Citation11 the improvement in the rTNSS from baseline in the MP-AzeFlu group (5.6 points) was statistically significant () compared to reformulated FP (P=0.038) and AZE (P=0.032). MP-AzeFlu significantly (P≤0.05) improved all the individual symptoms of the rTNSS compared to placebo with significantly (P≤0.05) greater improvement in nasal congestion and sneezing compared to reformulated FP and significantly (P≤0.029) greater improvement in nasal congestion than reformulated AZE ().
In a 4-hour in-office onset of action assessment following the first dose of study medication, MP-AzeFlu had a rapid onset of action within 30 minutes compared to placebo.Citation11 All active treatments significantly (P<0.05) improved the TOSS compared to placebo, with patients treated with MP-AzeFlu experiencing significantly (P≤0.029) better overall ocular symptom relief than patients treated with reformulated FP. Patients treated with MP-AzeFlu also reported statistical (P<0.001) and clinical improvements in the RQLQ score compared to placebo.
Spring to fall study (MP 4006)
Study MP 4006 was a large multicenter study initiated during the spring allergy season and conducted through the summer to the beginning of the fall season.Citation10 The results for all primary and secondary efficacy assessments in this study were similar to the results of studies MP 4002 and MP 4004. MP-AzeFlu significantly (P<0.001) improved the rTNSS compared to FP (P=0.029), AZE (P=0.016), and placebo (). MP-AzeFlu improved all individual rTNSS symptoms compared to placebo (P<0.05), and demonstrated significant improvement compared to FP in sneezing (P≤0.026) and to AZE in congestion, rhinorrhea, and sneezing (P≤0.026). RQLQ scores and TOSS were also significantly (P≤0.002) improved with MP-AzeFlu compared to placebo ().
Safety
Safety from studies MP 4001, MP 4002, MP 4004, and MP 4006
A total of 4,022 patients were evaluated for safety and tolerability in the 2-week studies MP 4001, MP 4002, MP 4004, and MP 4006, and >94% of the patients in each treatment group completed the full duration of the study period. In all the studies, the incidence and types of adverse events were similar across the active treatment groups (). The majority of all adverse events were considered mild in severity and unrelated to treatment. The most frequently reported adverse events with MP-Flu were dysgeusia (bitter taste) and epistaxis. These events, in particular dysgeusia, were mostly mild and transient in nature. The incidence of epistaxis with MP-AzeFlu was similar to that with placebo. The reasons that patients dropped out of the studies varied widely among the participants; however, there were no dropouts due to serious or unexpected adverse events.
Table 4 Overview of most frequent treatment-emergent adverse events (2-week studies)Table Footnotea
Post hoc efficacy analyses
To better characterize the efficacy of MP-AzeFlu, post hoc analyses of time to response for pre-determined clinically relevant endpoints included: 1) the percentage of patients achieving a 50% reduction in symptom scores and the time to reach this degree of improvement; 2) the percentage of patients with complete or near-complete symptom relief (no more than a single point remaining in any symptom); 3) response by disease severity; and 4) an analysis of a combined nasal and ocular symptom score.
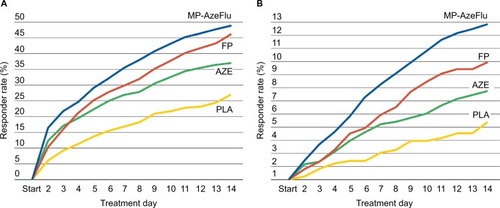
Post hoc analyses of studies MP 4002, MP 4004, and MP 4006 were included in the work by Carr et alCitation10 that showed that more patients treated with MP-AzeFlu had a 50% improvement in nasal symptoms compared to reformulated AZE and FP and achieved this improvement up to 3 days sooner compared to FP and up to 5 days sooner compared to AZE (). More patients treated with MP-AzeFlu (12.4%) had complete or near-complete relief of symptoms and experienced this relief 5–7 days sooner than patients treated with reformulated AZE (7.1%) or FP (9.3%; ).
Figure 2 Time-to-response curves showing the percentage of patients with a 50% improvement in rTNSS (A) or with a score of ≤1 point for each nasal symptom (B) after 2 weeks of treatment in studies MP 4002, MP 4004, and MP 4006.
Abbreviations: rTNSS, reflective total nasal symptom score; FP, fluticasone propionate; AZE, azelastine HCl; PLA, placebo.
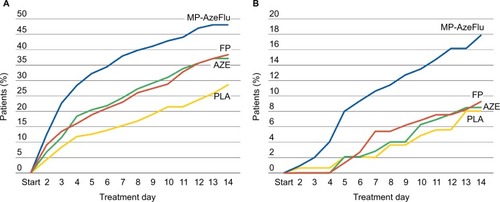
A similar analysis of the data from the Texas mountain cedar studyCitation13 also showed that more patients treated with MP-AzeFlu had a 50% improvement and achieved this improvement up to 6 days faster than with the commercially available AZE and FP alone (). More patients treated with MP-AzeFlu (17.8%, one in six) had complete or near-complete symptom relief compared to FP (9.2%) and AZE (8.3%). MP-AzeFlu patients achieved this level of improvement up to 8 days faster than FP (P=0.026) and 7 days faster than AZE (P=0.015). Overall, MP-AzeFlu was superior to placebo in improving the rTNSS for all patient types regardless of which individual symptom was the most prominent in their particular complex of symptoms. In a subset of patients with moderate-to-severe ocular symptoms, MP-AzeFlu was significantly better than FP (P=0.0012) and AZE (P=0.0456) alone. In addition, when nasal and ocular symptoms were combined into a composite total score, there was more than a two-fold improvement with MP-AzeFlu compared to commercially available AZE (P=0.0004) or FP (P=0.0013) ().
Figure 3 Time-to-response curves showing the percentage of patients with a 50% improvement in rTNSS (A) or with a score of ≤1 point for each nasal symptom (B) after 2 weeks of treatment in study MP 4001.
Abbreviations: rTNSS, reflective total nasal symptom score; FP, fluticasone propionate; AZE, azelastine HCl; PLA, placebo.
Discussion
Prevailing pollens and allergen sensitivity patterns differ across the US from season to season and year to year. With such wide regional and geographical variances, a new or existing AR treatment should show consistent effect regardless of the season or prevailing pollen. MP-AzeFlu’s clinical development program represented the largest head-to-head direct comparison of active treatments carried out in AR to date.Citation10 Furthermore, these studies were carried out during different times of year, during different pollen seasons, and in many centers, with a broad geographical spread across the US.
Seasonal allergies are caused by a variety of plant pollens, with the most common sources being grasses, trees, and weeds. Tree and grass pollens predominate in the spring and summer in most areas of the US, whereas weeds, in particular ragweed, are the most prevalent fall pollens.Citation17 In addition, areas of south central Texas and parts of Oklahoma, Missouri, and Arkansas have an abundance of pollen from cedar plants (Juniperus ashei) during the winter months.Citation18 In many parts of the US, in particular southern tier states, seasonal allergens can be prevalent year-round, compounding the problems that seasonal allergy sufferers experience.Citation1
Grass pollens are a major aeroallergen source world-wide. Global grass pollination patterns suggest that, in the future, subtropical grasses will increasingly contribute to the global burden of AR and asthma, in particular affecting heavily populated parts of Africa, India, Asia, Australia, and the Americas.Citation19 In addition, the duration of the grass allergy seasons in the US appears to be increasing. Across multiple geographical regions, the US grass pollen season varied from 34 days to 179 days, with evidence that over the past 10 years, the average duration of the pollen season is trending to be longer.Citation17
Ragweed pollen is the most prevalent fall pollen in the US and has one of the longest pollination seasons among the aeroallergens.Citation7 During a 14-year period from 1980 to 1994, two studies by the National Health and Nutrition Examination Survey conducted for the US National Center for Health Statistics identified prevalence rates of allergy to ragweed pollen more than doubling from 12.5% to 26.2% during that period.Citation20 In these studies, the prevalence rates for ragweed pollen allergy were highest in the Northeast (32.2%) and >22% in all US geographic regions.
Texas mountain cedar (J. ashei) is a drought-resistant shrub or small tree that is native to South Central Texas and parts of Oklahoma, Missouri, and Arkansas. Cedar pollen is unique in that pollination occurs in winter months in the US with peak pollen counts seen from mid-December to early February.Citation21 The highest pollen counts on record in the US have been attributed to Texas mountain cedar.Citation22 A study completed at the University of Texas Medical Branch at Galveston has identified the molecular structure of the cedar pollen, and the findings suggest that the unique structure of the cedar allergen may be responsible in part for the potent allergenicity.Citation23
The response to MP-AzeFlu was consistent across seasons for overall nasal symptom score, overall ocular symptom score, as well as for each of the individual nasal and ocular symptoms. In addition, MP-AzeFlu provided the same degree of relief regardless of season or prevailing pollen, providing confidence in response. The consistent effect on ocular symptom relief is particularly noteworthy because these ocular symptoms may have the greatest negative impact on patients’ quality of life, exceeding that of nasal congestion.Citation24 The consistent relief provided by MP-AzeFlu for each individual nasal and ocular symptom shows that no single symptom is driving the effect but that MP-AzeFlu provides a uniform reduction in each of the most common symptoms associated with SAR.Citation10 In addition, many patients with SAR are also sensitive to nonallergic triggers.Citation25 In patients with chronic rhinitis including nonallergic rhinitis and perennial allergic rhinitis, MP-AzeFlu was shown to be effective over a 1-year period with sustained efficacy greater than that seen with FP.Citation26
Regardless of allergy season or prevalent pollen, MP-AzeFlu improved overall nasal symptoms of AR to a significantly greater degree than FP or AZE, the two active treatments currently recommended as the first-line AR therapy.Citation1 MP-AzeFlu was effective during spring allergy seasons where trees and grasses are the predominant allergens and during ragweed season in the fall. In the MP 4006 study, MP-AzeFlu effectively relieved patients’ symptoms induced by allergens prevalent during summer months. In the Texas mountain cedar study, the patients showed greater improvement with MP-AzeFlu compared to the first-line active controls and placebo.
The superiority of MP-AzeFlu over AZE and FP was seen for each individual symptom of the rTNSS, and the onset of action of MP-AzeFlu was rapid, within 30 minutes. MP-AzeFlu also provided clinically important improvement in health-related quality of life. Post hoc efficacy analyses of the extent of response and time to response showed that more patients treated with MP-AzeFlu achieved greater improvements compared to patients treated with AZE or FP, and perhaps more importantly, achieved these responses significantly faster. To that extent, in an open-label, multi-center study in Germany that included 1,781 patients with AR, treatment with MP-AzeFlu resulted in higher response rates than seen in the double-blind trials.Citation27
The clinical benefits of MP-AzeFlu are facilitated not only by the incorporation of two active agents from different and complementary medication classes into a single spray but also by characteristics of the MP-AzeFlu nasal spray formulation (eg, drug concentration, spray volume, vehicle pH, isotonicity, and osmolality). MP-AzeFlu is a thixotropic suspension. Thixotropic suspensions flow freely as liquids when stirred or shaken and return to a more viscous suspension upon standing; the suspended particles do not settle rapidly, and any sediment produced is easily and uniformly redispersed by shaking. The suspension vehicle used for MP-AzeFlu allows for the reversible conversion between a viscous liquid and a more fluid liquid. The MP-AzeFlu formulation is isotonic and therefore has no effect on the movement of fluids into or out of cells. The isotonicity is adjusted using glycerin, which may act as a transporter of the active ingredients across the nasal mucosa. In addition, glycerin is a known humectant and can provide moisture-retention capacity to the formulation. The effect of formulation on clinical efficacy has been investigated with other treatments for AR.Citation28 The MP-AzeFlu formulation may have contributed to the larger treatment effect observed compared with commercially available active comparators, and these overall differences in formulation may contribute to the clinical efficacy of MP-AzeFlu.Citation29
The studies presented in this review included SAR patients 12 years and older with moderate/severe disease treated for 14 days. Within this time frame, MP-AzeFlu was well tolerated. The number of adverse events reported by patients was low in all active groups, with dysgeusia (bitter taste) most often reported in the MP-AzeFlu and AZE groups and headache and epistaxis more commonly reported in the FP group. These events were usually mild in intensity and transitory in nature. Bitter taste is a common side effect with AZE nasal spray; however, proper administration of the nasal spray will enable retention of the medication in the nasal mucosa and reduce the potential for taste problems.Citation30 A longer term study was also conduced outside of the US and showed that MP-AzeFlu was well tolerated after 1 year of continuous use, with no safety signal; this would preclude its long-term use.Citation31 The safety of MP-AzeFlu in adults and adolescents has been comprehensively reviewed.Citation32
Conclusion
MP-AzeFlu was statistically superior to both an intranasal antihistamine and an intranasal corticosteroid in four consecutive randomized, double-blind SAR studies conducted in different US allergy seasons. MP-AzeFlu provided clinical benefits beyond what is achieved with two currently available first-line intranasal therapies, making it the ideal treatment consideration for SAR.
Acknowledgments
Funding for clinical studies and writing support for the manuscript were provided by Meda Pharmaceuticals Inc., Somerset, NJ, USA.
Disclosure
The author has received research support and consultancy and speaker fees from Meda Pharmaceuticals, and reports no other conflicts of interest in this work.
References
- WallaceDVDykewiczMSBernsteinDIThe diagnosis and management of rhinitis: an updated practice parameterJ Allergy Clin Immunol20081222 SupplS1S8418662584
- NathanRAMeltzerEODereberyJThe prevalence of nasal symptoms attributed to allergies in the United States: findings from the burden of rhinitis in an America surveyAllergy Asthma Proc200829660060819173786
- DalalAAStanfordRHenryHBorahBEconomic burden of rhinitis in managed care: a retrospective claims data analysisAnn Allergy Asthma Immunol20081011232918681080
- LevetinEVan de WaterPChanging pollen types/concentrations/distribution in the United States: fact or fiction?Curr Allergy Asthma Rep20088541842418682110
- WaynePFosterSConnollyJBazzazFEpsteinPProduction of allergenic pollen by ragweed (Ambrosia artemisiifolia L.) is increased in CO2-enriched atmospheresAnn Allergy Asthma Immunol200288327928211926621
- ZhangYBieloryLZhongyuanMTingCRobockAGeorgopoulosPAllergenic pollen season variations in the past two decades under changing climate conditions in the United StatesGlob Chang Biol20142141581158925266307
- BieloryLLyonsKGoldbergRClimate change and allergic diseaseCurr Allergy Asthma Rep201212648549423065327
- MeltzerEOGrossGNKatialRStormsWWAllergic rhinitis substantially impacts patient quality of life: findings from the Nasal Allergy Survey Assessing LimitationsJ Fam Pract2012612 SupplS5S1022312622
- GrossGKatialRHadleyJMarpleBRyanSStoloffSNasal Allergy Survey Assessing Limitations (NASL) 2010 Survey: allergic rhinitis continues to impact patient quality of lifeJ Allergy Clin Immunol2011127Issue 2AB217
- CarrWBernsteinJLiebermanPA novel intranasal therapy of azelastine with fluticasone for the treatment of allergic rhinitisJ Allergy Clin Immunol201212951282128922418065
- MeltzerEOLaForceCRatnerPPriceDGinsbergDCarrWMP29-02 (a novel intranasal formulation of azelastine hydrochloride and fluticasone propionate) in the treatment of seasonal allergic rhinitis: a randomized, double-blind, placebo-controlled trial of efficacy and safetyAllergy Asthma Proc201233432433222856633
- HampelFCRatnerPVan BavelJDouble-blind, placebo-controlled study of azelastine and fluticasone in a single nasal spray delivery deviceAnn Allergy Asthma Immunol2010105216817320674829
- MeltzerERatnerPBachertCClinically relevant effect of a new intranasal therapy (MP29-02) in allergic rhinitis assessed by responder analysisInt Arch Allergy Immunol2013161436937723652808
- FDA Guideline [webpage on the Internet]Guidance for Industry Allergic Rhinitis: Clinical Development Programs for Drug ProgramsUS Department of Health and Human Services, FDA Center for Drug Evaluation and Research2000 Available from: http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/ucm071293.pdfAccessed May 9, 2016
- EMA GuidelineGuideline on the Clinical Development of Medicinal Products for the Treatment of Allergic Rhinoconjunctivitis CHMP/EWP/2455/022004 Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2009/09/WC500003554.pdfAccessed May 9, 2016
- JuniperEFGuyattGHDevelopment and testing of a new measure of health status for clinical trials in rhinoconjunctivitisClin Exp Allergy199121177832021881
- ZiskaLKnowltonKRogersCRecent warming by latitude associated with increased length of ragweed season in central North AmericaPNAS2011108104248425121368130
- Van de WaterPKKeeverTMainCELevetinEAn assessment of predictive forecasting of Juniperus Ashei pollen movement in the southern great plains, USAInt J Biometerol20034827482
- DaviesJMGrass pollen allergens globally: the contribution of subtropical grasses to burden of allergic respiratory diseasesClin Exp Allergy201444679080124684550
- ArbesSJGergenPJEliotLZeldinDCPrevalences of positive skin test responses to 10 common allergens in the US population: results from the Third National Health and Nutrition Examination SurveyJ Allergy Clin Immunol2005116237738316083793
- Allergy and Asthma Center of Austin [homepage] Available at: http://www.nosneezes.comAccessed May 9, 2016
- San Antonio Express-News [webpage on the Internet]Cedar and Allergy Symptoms Hit Highest Levels of the Season2014 http://www.mysanantonio.com/business/health-care/article/Cedar-and-allergy-symptoms-hit-highest-levels-of-5150578.phpAccessed September 25, 2014
- CzerwinskiEWMidoro-HoriutiTWhiteMABrooksEGGoldblumRMCrystal structure of Jun a 1, the major cedar pollen allergen from Juniperus ashei, reveals a parallel B-helical coreJ Biological Chem2005280537403746
- BousquetPJDemolyPDevillierPMesbahKBousquetJImpact of allergic rhinitis on quality of life in primary careInt Arch Allergy Immunol2013160439340023183377
- RidoloEMontagniMMelliVBonzanoLIncorvaiaCCanonicaGWA role for the intranasal formulation of azelastine hydrochloride/fluticasone propionate in the treatment of allergic rhinitisTher Deliv20156665365925913181
- PriceDShahSBhatiaSA new therapy (MP29-02) is effective for the long-term treatment of chronic rhinitisJ Investig Allergol Clin Immunol2013237495503
- KlimekLBachertCMosgesREffectiveness of MP29-02 for the treatment of allergic rhinitis in real-life: results from a noninterventional studyAllergy Asthma Proc2015361404725562555
- SalapatekAMLeeJPatelDSolubilized nasal steroid (CDX-947) when combined in the same solution nasal spray with an antihistamine (CDX-313) provides improved, fast-acting symptom relief in patients with allergic rhinitisAllergy Asthma Proc201132322122921477425
- BousquetJBachertCBernsteinJAdvances in pharmacotherapy for the treatment of allergic rhinitis; MP29-02 (a novel formulation of azelastine hydrochloride and fluticasone propionate in an advanced delivery system) fills the gapsExpert Opin Pharmacother201516611625387541
- Dymista [package insert]Somerset, NJMeda Pharmaceuticals2012
- BergerWEShahSLiebermanPLong-term, randomized safety study of MP29-02 (a novel formulation of azelastine hydrochloride and fluticasone propionate in an advanced delivery system) in subjects with chronic rhinitisJ Allergy Clin Immunol Pract20142217918524607046
- KlimekLBousquetJPriceDSafety evaluation of MP29-02 (a novel formulation of azelastine hydrochloride and fluticasone propionate) for allergic rhinitisExp Opin Drug Safety2016151117129