
Abstract
Objective
There have been only a few studies of ischemic stroke in patients with pulmonary tuberculosis (pTB). This study aimed to explore the clinical features and the underlying pathogenesis of pulmonary tuberculosis-related ischemic stroke (TBRIS).
Methods
Active pulmonary tuberculosis patients with acute ischemic stroke (without conventional vascular risk factors) were recruited as the TBRIS group. Patients who solely had active pulmonary tuberculosis were recruited as the control group (pTB group). Clinical data were collected, and multiple logistic regression analysis was applied to analyze the independent risk factors for TBRIS.
Results
A total of 179 TBRIS patients and 179 pTB patients were enrolled. Most (56.42%) of the TBRIS patients experienced the ischemic stroke events within 3 months after the diagnosis of tuberculosis. The multiple logistic regression analysis revealed that an increased mean platelet volume; elevated plasma D-dimer, C-reactive protein, and serum ferritin levels; and an increased monocyte percentage were independent risk factors for TBRIS. The AUC of the identification model was 0.778, with a sensitivity of 70.30% and a specificity of 78.90%.
Conclusion
The findings in the present study suggested that most of the TBRIS patients experienced ischemic stroke within 3 months after the diagnosis of tuberculosis. And the more intensive immune response to the tuberculosis infection in the TBRIS group contributed to the initiation of platelet activation and to the development of a hypercoagulable state, which were attributed to the pathogenesis of TBRIS. Index of TBRIS equaling to 0.3234 facilitates clinicians to identify the pTB patients who were at higher risk for TBRIS, and allow physicians to take further effective measures to prevent ischemic stroke in patients with pTB. However, our findings will need to be confirmed by further studies.
Introduction
Tuberculosis is a poorly controlled infectious disease worldwide, and extrapulmonary tuberculosis within the central nervous system is the most devastating and deadly form of tuberculosis.Citation1,Citation2 Ischemic stroke is a noninfectious disease that occurs worldwide. Previous study showed that patients with tuberculous meningitis were at high risk of ischemic stroke, and the interval of development of ischemic stroke after the diagnosis of tuberculous meningitis in some patients was shortly only one month, and the ischemic stroke tended to worsen the prognosis.Citation3–5 Pulmonary tuberculosis is more common than tuberculous meningitis. However, the relationship between pulmonary tuberculosis and ischemic stroke is not fully understood. In 1997, Schoeman et al reported a child with miliary pulmonary tuberculosis that was complicated by acute ischemic stroke. A follow-up autopsy found that the cerebral artery embolus that caused the ischemic stroke was composed of inflammatory granulomas, suggesting that pulmonary tuberculosis might directly cause ischemic stroke, namely pulmonary tuberculosis-related ischemic stroke (TBRIS).Citation6 Since then, acute ischemic stroke has been reported in patients with active pulmonary tuberculosis, which seems to further suggest a relationship between pulmonary tuberculosis and ischemic stroke.Citation7–9 In 2010, in order to explore the relationship between pulmonary tuberculosis and ischemic stroke, Sheu et al performed a population-based three-year follow-up study using an insurance database, in which 2283 tuberculosis patients were included as the experimental group and 6849 patients without tuberculosis were included as the comparison group, and the study found that the risk of ischemic stroke in patients with pulmonary tuberculosis was 1.52 times higher than that of the patients without tuberculosis, suggesting that pulmonary tuberculosis might directly or indirectly lead to ischemic stroke and that TBRIS clinically exists.Citation10 However, in 2014, Wu and his teams carried out another 3-year follow-up study, by using a similar insurance database, and the study found that pulmonary tuberculosis did not increase the risk of ischemic stroke.Citation11 However, it is well known that pulmonary tuberculosis is a chronic infectious disease and a curable disease. When pulmonary tuberculosis is active, elevated plasma inflammatory factors, such as C-reactive protein, increased platelet activation and the development of a hypercoagulable state, may be continued.Citation12–14 More importantly, elevated plasma inflammatory factors, such as C-reactive protein, platelet activation and the hypercoagulable state, have been found to contribute not only to an increased risk of ischemic stroke but also to a poor prognosis.Citation15–18 As a result, it was hypothesized that active pulmonary tuberculosis may lead to ischemic stroke through elevated plasma inflammatory factors, such as C-reactive protein, platelet activation and/or hypercoagulability, namely TBRIS. However, the clinical features and underlying pathogenesis of TBRIS have not been fully elucidated.
To investigate the clinical features and underlying pathogenesis of TBRIS, in the present retrospective case–control study, active pulmonary tuberculosis patients with acute ischemic stroke but without conventional vascular risk factors were included as the experimental group, and pure active pulmonary tuberculosis patients without stroke also without conventional vascular risk factors were included in the control group. Then, the plasma inflammatory markers, indicators of platelet activation, and D dimer levels in both the experimental and control groups were collected. Finally, the risk factors for TBRIS and the possible pathogenesis of ischemic stroke were evaluated through a univariate analysis, multivariate logistic regression and ROC analysis. This study should facilitate clinicians identify the patients with pulmonary tuberculosis who are at high risk for ischemic stroke and will allow physicians to take further effective measures to prevent ischemic stroke in patients with pulmonary tuberculosis.
Materials and Methods
This study was conducted in accordance with the Declaration of Helsinki and approved by the First Affiliated Hospital of Guangxi Medical University Ethical Review Committee. Approval Number: 2022 (KY-E-010). The written informed consent was waived because of the retrospective nature of our study. During the data collection, personally identifiable information such as names, addresses and phone numbers of the study participants were never recorded. The collected data were kept confidentially and used only for the purpose of the study.
Patient Selection
Patients with TBRIS who were hospitalized between January 2011 and December 2020 in 5 centers (The First and the Second Affiliated Hospital of Guangxi Medical University, The Wuming Hospital of Guangxi Medical University, People’s Hospital of Guangxi Zhuang Autonomous Region and The Fourth People’s Hospital of Nanning City) were included in the present study as the TBRIS group. Considering the difficulty in accurately diagnosing TBRIS in clinical practice, and after referring to the conception of cancer-related ischemic stroke,Citation19,Citation20 TBRIS in the present study was defined as patients with active pulmonary tuberculosis and acute ischemic stroke without conventional stroke risk factors. According to the American Heart Association diagnostic criteria for stroke,Citation21 acute ischemic stroke was diagnosed as follows: patients who suffered from a new and sudden onset of focal neurological deficits, such as limb weakness or numbness in one or both limbs, fatigue or aphasia. The patients’ brain MRIs and/or CTs could identify the ischemic lesions that were consistent with the neurological symptoms.
The conventional stroke risk factors were defined as follows: (i) hypertension (taking antihypertensive drugs, diastolic blood pressure ≥90 mmHg, or systolic blood pressure ≥140 mm Hg); (ii) diabetes (taking anti-diabetic drugs or random blood glucose level ≥11.1 mmol/L);Citation22 (iii) hyperlipidemia (taking lipid-lowering drugs, low-density lipoprotein >3.64 mmol/L, serum total cholesterol >5.72 mmol/L or triglycerides >1.70 mmol/L);Citation23 and (iv) smoking and drinking, coronary artery disease, rheumatic heart valve disease, and atrial fibrillation (history of disease or assessed by a cardiologist according to the electrocardiogram and transthoracic echocardiography at admission).
Active pulmonary tuberculosis was diagnosed based on the “Guideline” for pulmonary tuberculosis.Citation24 The patients had symptoms, such as cough, expectoration, hemoptysis, night sweats, fever, weight loss and loss of appetite. Furthermore, one of the following four laboratory conditions were required for confirmed cases of pulmonary tuberculosis: (i) 2 sputum smears positive for acid-fast bacilli or 1 sputum smear positive for acid-fast bacilli with chest imaging that had changes consistent with active pulmonary tuberculosis or 1 sputum smear that was positive for acid-fast bacilli with 1 sputum mycobacterium culture that was positive; (ii) positive culture of Mycobacterium tuberculosis and the chest imaging showed changes consistent with active pulmonary tuberculosis; (iii) positive detection of Mycobacterium tuberculosis nucleic acid and chest imaging had evidence for active pulmonary tuberculosis; and (iv) The pathological examination of lung tissue was consistent with the pathological changes of tuberculosis.
The exclusion criteria for the TBRIS group included (i) patients with tuberculosis in lung tissue and other organs outside the pleura; (ii) patients with malignant tumors, HIV or Treponema pallidum infection, or autoimmune disease; (iii) patients with heart, kidney or liver failure; (iv) patients with bacterial, fungal pneumonia or sepsis; and (v) patients with various types of encephalitis, such as tuberculous meningitis and cryptococcal meningitis; (vi) patients with incomplete clinical or imaging data.
Age-, sex- and living condition-matched patients with only active pulmonary tuberculosis were recruited as the control group (pTB group). The pTB group was hospitalized at the same center during the same period, and the pTB group shared the same exclusion criteria as the TBRIS group.
Collection of Clinical Data
The general data were collected, and the data included demographic data (age, sex and living conditions) and conventional stroke risk factors, such as smoking, hypertension, diabetes, coronary artery disease, rheumatic heart valve disease and atrial fibrillation. The symptoms and signs of focal neurological deficits, the lesions of ischemic stroke and the precise timing for the diagnosis of stroke were also collected. Data on pulmonary tuberculosis, such as the patient’s signs and symptoms, the clinical types of pulmonary tuberculosis (including primary pulmonary tuberculosis, hematogenous pulmonary tuberculosis, secondary pulmonary tuberculosis, tuberculous pleurisy, tuberculous tracheitis, tuberculous bronchitis), and the actual timing of the diagnosis were collected at the same time. The etiologies of the tuberculosis cases were also collected.
Routine laboratory data were also collected, such as routine blood tests, erythrocyte sedimentation rate (ESR), C-reactive protein, serum ferritin (SF), and D-dimer. For TBRIS patients, the laboratory data was collected according to the following conditions: (I) data was collected within 24 hours after admission, and the data were from patients who were admitted for acute ischemic stroke while being diagnosed with pulmonary tuberculosis during the treatment of ischemic stroke. (II) The data was collected within 24 hours of the acute ischemic stroke attack, and the data were from patients who were diagnosed with acute ischemic stroke during the treatment of pulmonary tuberculosis.
Furthermore, the imaging finding results (such as cranial CT, CT angiography, MRI, magnetic resonance angiography, diffusion-weighted MRI, chest CT or X-ray, trans-cranial Doppler ultrasound, echocardiography and ambulatory blood pressure monitoring) were collected.
Treatment
In the present study, all patients in both the TBRIS group and the pTB group received standard anti-tuberculosis treatment according to the guidelines for tuberculosis.Citation21 Patients in the TBRIS group were treated with anti-acute ischemic stroke medications according to the guidelines for acute ischemic stroke, 12 patients first received venous thrombolysis therapy, and all patients received antiplatelet therapy.Citation20
Statistical Analysis
Statistical analyses were performed using SPSS version 26.0 software (IBM). p < 0.05 was considered statistically significant. Continuous variables were compared between the 2 groups using Student’s t-test and the Mann–Whitney U-test, while categorical variables were compared using the χ2 test. To explore the independent risk factors for TBRIS, variables with p < 0.05 in the univariate analyses were analyzed in the multiple logistic regression analysis. In order to create a reliable model to identify TBRIS, we combined the independent risk factors for TBRIS to develop the index of TBRIS. Moreover, an ROC analysis was used to compare the area under the ROC curve (AUC) of the index of TBRIS with every independent risk factor using MedCalc version 15.8 software packages.
Results
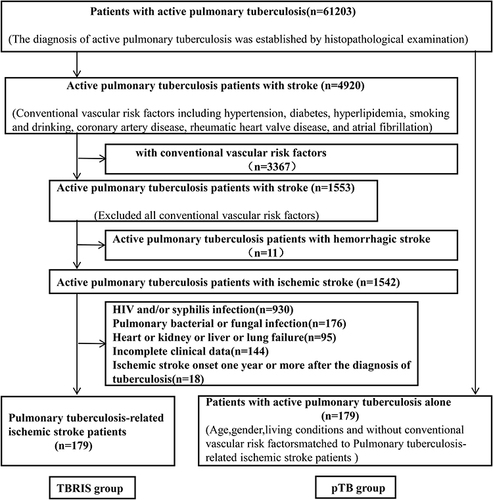
In the present study, there were 61,203 active pulmonary tuberculosis patients and 4920 active pulmonary tuberculosis patients with acute ischemic stroke were firstly screened out. Then, 179 patients who met the TBRIS criteria were enrolled as TBRIS group. And the other 4741 patients were excluded, including 3367 patients with traditional stroke risk factors, 11 patients with cerebral hemorrhage, 930 patients with HIV and/or a syphilis infection, 176 patients with pulmonary bacterial or fungal infections, 95 patients with heart, kidney, liver or lung failure, 144 patients with incomplete clinical data and 18 patients with an onset of ischemic stroke one year or more after the diagnosis of tuberculosis. Finally, 179 patients aged 32–84 years (median 66.00 [IQR 12], 124 males, 55 females) were enrolled in TBRIS group. In the pTB group, 179 patients were included, and they were aged 48–85 years (median 64.00 [IQR 10], 109 males, 70 females). No significant differences were found in the living conditions, sex or age between the two groups (p > 0.05) ( and ). The two groups of patients shared similar pulmonary tuberculosis manifestations: cough, expectoration, night sweats, weight loss, fever and appetite loss. Pulmonary CT and/or X-ray showed that secondary pulmonary tuberculosis was the most common clinical type of tuberculosis in the two groups (97.2% vs 98.3%), followed by hematogenous pulmonary tuberculosis (2.8% vs 1.7%). There was no significant difference in the clinical types of pulmonary tuberculosis between the two groups (p > 0.05) ().
Table 1 General Data
Figure 1 Flowchart for the screening of patients with pulmonary tuberculosis-related ischemic stroke. TBRIS: pulmonary tuberculosis-related ischemic stroke pTB: pulmonary tuberculosis.
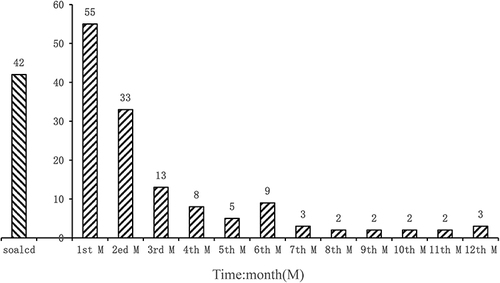
In the TBRIS group, 42 (21.46%) patients were hospitalized for first-ever ischemic stroke and were found to have active pulmonary tuberculosis during hospitalization, and these patients were given anti-tuberculosis treatment. A total of 137 (76.54) active pulmonary tuberculosis patients were first diagnosed with acute ischemic stroke while receiving antituberculosis treatment. Among these patients, 101 (56.42%), 22 (12.29%) and 14 (7.82%) patients experienced ischemic stroke within the first 3 months, 4–6 months and 7–12 months, respectively ().
Figure 2 Temporal map between the course of pulmonary tuberculosis and the onset of ischemic stroke. ![]()
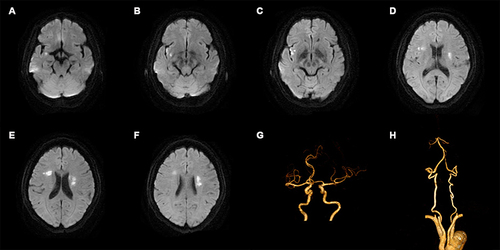
In addition, in the TBRIS group, there were 138 (138/179, 77.09%) patients who had 2 or more scattered, patchy and variable-sized ischemic lesions according to the neuroimaging studies. These lesions were distributed to 2 or more cerebral arterial territories in most of the patients (118/179, 65.92%) but were confined to only one cerebral arterial territory in the other patients (20/179, 11.17%). Moreover, 41 (41/179, 22.91%) patients had a single ischemic lesion (). Regarding the locations of the lesions, most of the ischemic lesions were scattered in the basal ganglia, the next mostly likely locations were the semioval center and thalamus regions, followed by the frontal lobe, parietal lobe, temporal lobe, cerebellum and brain stem, and the occipital lobe was the least likely to be involved (). The vascular examinations revealed that the cerebrovascular vessels were normal in the patients in the present study ().
Table 2 Comparison of the Laboratory Data Between the Patients with TBRIS and pTB
Figure 3 Typical neuroimage of a patient with acute ischemic stroke and active pulmonary tuberculosis. Images are from a male in his 50s who had acute ischemic stroke without conventional stroke risk factors and who was initially diagnosed with active pulmonary tuberculosis during the treatment of ischemic stroke. Six MRI diffusion-weighted images (picture A–F) show multiple high-signal lesions in multiple arterial regions of the brain. Two pictures of computed tomography angiography (picture G and H) show normal cerebral vessels.
Compared to the pTB group, the TBRIS group had higher WBC counts, Hb levels, neutrophil counts, neutrophil percentages, lymphocyte counts, lymphocyte percentages, neutrophil-to-lymphocyte ratios (NLR), monocyte counts, monocyte percentages, mean platelet volumes (MPV), D-dimer, C-reactive protein (CRP), serum ferritin (SF) and serum albumin (ALB) (p < 0.05) (). The TBRIS group also had higher mortality rates (7.45%, 15.96%) at 30 days and 90 days after the stroke (). Furthermore, the multiple logistic regression analysis revealed that elevated D-dimer levels (odds ratio [OR]:1.432, 95%confidence interval [CI]:1.072–1.911, p < 0.05), MPV (OR:1.833, 95% CI:1.371–2.450, p < 0.05), CRP levels (OR:1.014, 95% CI:1.001–1.02, p < 0.05), SF (OR:1.001, 95% CI:1.000–1.002, p < 0.05), and monocyte percentages (OR:1.253, 95% CI:1.036–1.515, p < 0.05) were independent risk factors for TBRIS ().
Table 3 Multivariate Logistic Regression Analysis
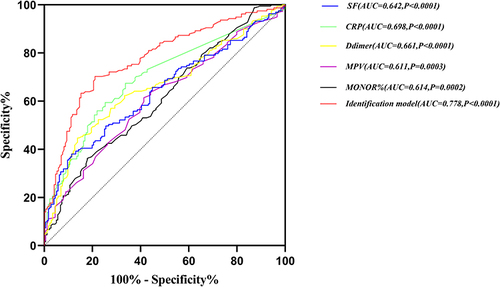
Compared to the AUCs of the D-dimer, mean platelet volume, C-reactive protein, serum ferritin, and monocyte percentage, the AUC of the index of TBRIS was the largest (AUC = 0.778, sensitivity 70.30%, specificity 78.90%), with the cutoff value equaling to 0.3234 ( and ).
Table 4 ROC Analysis of the Independent Risk Factors and the Identification Model of TBRIS
Figure 4 Analysis of the ROC curve and the area under the curve.
Discussion
In the present study, most TBRIS patients (56.42%) developed an ischemic stroke within 3 months after the diagnosis of pulmonary tuberculosis, suggesting that TBRIS were likely to develop during the intensive inflammatory response period that occurred in active pulmonary patients. Some TBRIS patients presented with ischemic stroke as the initial event, and these patients were diagnosed with active pulmonary tuberculosis during the anti-ischemic stroke treatment. Although acute ischemic stroke has often been found in patients with active pulmonary tuberculosis,Citation7–9and active pulmonary tuberculosis was found to increase the risk for ischemic stroke,Citation10 the relationship between active pulmonary tuberculosis and ischemic stroke has not been established.Citation10,Citation11 However, the findings in the present study still indicated that pulmonary tuberculosis should be considered while determining the etiology of an ischemic stroke because pulmonary tuberculosis is one of the possible causes of cryptogenic ischemic stroke.
In the present study, the neuroimaging showed that TBRIS was associated with particularly striking features. First, brain MRI and/or CT showed that most patients with TBRIS had 2 or more ischemic lesions that were distributed in 2 or more cerebral arterial territories and that the ischemic lesions commonly appeared in the basal ganglia, semioval center and thalamus regions. Second, the vascular examinations showed that the TBRIS patients in the present study had normal cerebral vessels. The patients with tuberculous meningitis were also found to be at high risk for ischemic stroke. The neuroimaging features of the ischemic strokes in patients with tuberculous meningitis include multiple lacunar lesions, and these lesions are mostly involved in the “TB zone”, which are supplied by the medial lenticulostriate and thalamoperforating arteries.Citation5,Citation25,Citation26 However, the neuroimaging features of TBRIS have not been reported.
In the present study, the TBRIS group also had a higher mortality rate, both at the 30th day and at the 90th day after the ischemic stroke, compared to the pTB group, indicating that ischemic stroke not only lead to physical disability but also might lead to more severe outcomes in patients with pTB. Therefore, to prevent the development of TBRIS and to improve the prognosis of patients with TBRIS, it is not only useful but necessary to elucidate the pathogenesis of TBRIS.
In the present study, the multivariate analysis showed that elevated plasma levels of D-dimer, MPV, CRP, and SF and an increase in the monocyte percentage were independent risk factors for TBRIS, implying that these independent risk factors alone or in combination promoted the development of TBRIS through different kinds of pathways.
Generally, previous studies have demonstrated that tuberculosis may lead to elevated inflammatory factors in the plasma, such as CRP and SF, and may also lead to platelet activation and the development of a systemic hypercoagulable state.Citation12–14,Citation27,Citation28 First, in the present study, the TBRIS group had elevated plasma inflammatory factors, such as CRP and SF, and an increased monocyte percentage compared to the pTB group, which implies that the immune response to tuberculosis infection may be more intensive in TBRIS patients compared to pTB patients.Citation29 Moreover, a higher MPV was also found in the TBRIS group. As it has been reported that a higher MPV is a common biomarker for platelet activation and that a higher MPV is correlated with the CRP concentration,Citation30 the more intensive immune response to the tuberculosis infection in the TBRIS group may have induced the increase in the platelet activation in the TBRIS group. As platelet activation has a close relationship with the development of a hypercoagulable state,Citation31–33 the more intensive immune response to a tuberculosis infection may induce a stronger hypercoagulable state in the TBRIS group.
In addition, in the present study, the TBRIS group had elevated plasma D-dimer levels. As previous studies have found that elevated plasma D-dimer levels were common in patients with ischemic strokeCitation18,Citation34,Citation35 and in patients with pTB,Citation36 that elevated plasma D-dimer levels have been used as a biomarker of a hypercoagulable state, and that pulmonary tuberculosis could cause a hypercoagulable state,Citation37 the TBRIS group may have developed a stronger hypercoagulable state. Furthermore, Seok et alCitation38 found that elevated plasma D-dimer levels were linearly correlated with the frequency of the microembolic signals in the internal carotid on transcranial Doppler ultrasound and were correlated with the development of thrombotic stroke, indicating that a hypercoagulable state may lead to ischemic stroke. In summary, in the present study, the more intensive immune response to tuberculosis infection in the TBRIS group may initially induce more active platelet activation, then a stronger hypercoagulable state and ultimately the development of TBRIS.
In the present study, the ROC curve analysis showed that the index of TBRIS had the largest AUC, which suggests that the independent risk factors that were included in the index of TBRIS altogether promoted the development of TBRIS, and this also illustrates that the index of TBRIS had the most power to predict the pTB patients who were at higher risk for TBRIS. Clinicians should identify TBRIS from other subtypes of ischemic stroke in terms of the etiology with the index of TBRIS equaling to 0.3234 (such as an ischemic stroke resulting from an atherosclerotic thrombosis of the large artery in pTB patients). In addition, the concept of TBRIS and its clinical characteristics and possible pathogenesis have raised more people’s attention to enhance the quality of life of patients with pTB through effectively preventive and therapeutic measures for TBRIS.Citation39
Our study has limitations. First of all, due to our strict inclusion criteria for TBRIS, the number of TBRIS patients included in our study was still small despite the retrieval of 10-year data from 5 centers. Second, due to the retrospective nature of the study, the findings need to be confirmed by future studies.
Conclusion
The findings in the present study suggested that most of the TBRIS patients experienced ischemic stroke within 3 months after the diagnosis of tuberculosis. And the more intensive immune response to the tuberculosis infection in the TBRIS group contributed to the initiation of platelet activation and to the development of a hypercoagulable state, which were attributed to the pathogenesis of TBRIS. Index of TBRIS equaling to 0.3234 facilitates clinicians to identify the pTB patients who were at higher risk for TBRIS and allow physicians to take further effective measures to prevent ischemic stroke in patients with pTB. However, our findings will need to be confirmed by further studies.
Data Sharing Statement
The datasets generated and analyzed in this study will be available by the corresponding author upon reasonable request.
Ethical Approval
This project fully considered and protected the rights and interests of the study objects. It meets the criteria of Ethical Review Committee. The Medical Ethics Committee of The First Affiliated Hospital of Guangxi Medical University has approved the protocol.
Informed Consent
The written informed consent was waivered because of the retrospective nature of our study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
We would like to thank Prof. Li for her guidance on statistical methods. We are grateful for the advice and discussions with our colleagues Junli Liang and Jinyu Liang as well as the anonymous reviewers.
Additional information
Funding
References
- Berger CA, Alipanah N, Kheir F, et al. Summary for clinicians: 2019 clinical practice guideline summary for the treatment of drug-resistant tuberculosis. Ann Am Thorac Soc. 2020;17(8):911–917. doi:10.1513/AnnalsATS.202004-318CME
- Eisinger RW, Embry AC, Read SW, Fauci AS. 2019: a banner year for tuberculosis research. J Infect Dis. 2020;222(11):1768–1771. doi:10.1093/infdis/jiaa051
- Solomons RS, Nieuwoudt ST, Seddon JA, van Toorn R. Risk factors for ischemic stroke in children with tuberculous meningitis. Childs Nerv Syst. 2021;37(8):2625–2634. doi:10.1007/s00381-021-05163-2
- Zhang L, Zhang X, Li H, Chen G, Zhu M. Acute ischemic stroke in young adults with tuberculous meningitis. BMC Infect Dis. 2019;19(1):362. doi:10.1186/s12879-019-4004-5
- Misra UK, Kalita J, Maurya PK. Stroke in tuberculous meningitis. J Neurol Sci. 2011;303(1–2):22–30. doi:10.1016/j.jns.2010.12.015
- Schoeman JF, Rutherfoord GS, Hewlett RH. Acute stroke in a child with miliary tuberculosis. Clin Neuropathol. 1997;16(6):303–308.
- Arulprakash N, Narayanan L, Narayanan S, Young A. Patient with stroke and primary tuberculosis. J Neurosci Rural Pract. 2018;9(4):613–615. doi:10.4103/jnrp.jnrp_59_18
- Briones-Claudett K, Briones-Claudett M, Briones Zamora K, et al. Ischemic stroke and disseminated tuberculosis in intensive care: a case report. Am J Case Rep. 2020;21:e920410. doi:10.12659/AJCR.920410
- Radmanesh F, Nejat F, El Khashab M. Cerebral infarction as the first presentation of tuberculosis in an infant: a case report. J Microbiol Immunol Infect. 2010;43(3):249–252. doi:10.1016/S1684-1182(10)60039-4
- Sheu J, Chiou H, Kang J, Chen Y, Lin H. Tuberculosis and the risk of ischemic stroke: a 3-year follow-up study. Stroke. 2010;41(2):244–249. doi:10.1161/STROKEAHA.109.567735
- Wu C, Chen L, Yen M, et al. Does non-central nervous system tuberculosis increase the risk of ischemic stroke? A population-based propensity score-matched follow-up study. PLoS One. 2014;9(7):e98158. doi:10.1371/journal.pone.0098158
- Wilson D, Moosa MS, Cohen T, et al. Evaluation of tuberculosis treatment response with serial C-reactive protein measurements. Open Forum Infect Dis. 2018;5(11):ofy253. doi:10.1093/ofid/ofy253
- Kirwan DE, Chong DLW, Friedland JS. Platelet activation and the immune response to tuberculosis. Front Immunol. 2021;12:631–696. doi:10.3389/fimmu.2021.631696
- Cudahy PGT, Warren JL, Cohen T, Wilson D. Trends in C-reactive protein, D-Dimer, and fibrinogen during therapy for HIV-associated multidrug-resistant tuberculosis. Am J Trop Med Hyg. 2018;99(5):1336–1341. doi:10.4269/ajtmh.18-0322
- Shantikumar S, Grant PJ, Catto AJ, Bamford JM, Carter AM. Elevated C-reactive protein and long-term mortality after ischaemic stroke: relationship with markers of endothelial cell and platelet activation. Stroke. 2009;40(3):977–979. doi:10.1161/STROKEAHA.108.525105
- Kollikowski AM, Pham M, März AG, et al. Platelet activation and chemokine release are related to local neutrophil-dominant inflammation during hyperacute human stroke. Transl Stroke Res. 2021;13(3):364–369. doi:10.1007/s12975-021-00938-w
- Ferreira JP, Lam CSP, Anker SD, et al. Plasma D-dimer concentrations predicting stroke risk and rivaroxaban benefit in patients with heart failure and sinus rhythm: an analysis from the COMMANDER-HF trial. Eur J Heart Fail. 2021;23(4):648–656. doi:10.1002/ejhf.2003
- Alvarez-Perez FJ, Castelo-Branco M, Alvarez-Sabin J. Usefulness of measurement of fibrinogen, D-dimer, D-dimer/fibrinogen ratio, C reactive protein and erythrocyte sedimentation rate to assess the pathophysiology and mechanism of ischaemic stroke. J Neurol Neurosurg Psychiatry. 2011;82(9):986–992. doi:10.1136/jnnp.2010.230870
- Kono T, Ohtsuki T, Hosomi N, et al. Cancer-associated ischemic stroke is associated with elevated D-dimer and fibrin degradation product levels in acute ischemic stroke with advanced cancer. Geriatr Gerontol Int. 2012;12(3):468–474. doi:10.1111/j.1447-0594.2011.00796.x
- Bang OY, Seok JM, Kim SG, et al. Ischemic stroke and cancer: stroke severely impacts cancer patients, while cancer increases the number of strokes. J Clin Neurol. 2011;7(2):53–59. doi:10.3988/jcn.2011.7.2.53
- Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 Guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50(12):e344–e418. doi:10.1161/STR.0000000000000211
- Draznin B, Aroda VR, Bakris G, et al. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes-2022. Diabetes Care. 2022;45(Suppl 1):S17–s38.
- Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. J Am Coll Cardiol. 2019;73(24). e285–e350.
- Nahid P, Mase SR, Migliori GB, et al. Treatment of drug-resistant tuberculosis. an official ATS/CDC/ERS/IDSA clinical practice guideline. Am J Respir Crit Care Med. 2019;200(10):e93–e142. doi:10.1164/rccm.201909-1874ST
- Garg RK, Sharma R, Kar AM, et al. Neurological complications of miliary tuberculosis. Clin Neurol Neurosurg. 2010;112(3):188–192. doi:10.1016/j.clineuro.2009.11.013
- Hsieh FY, Chia LG, Shen WC. Locations of cerebral infarctions in tuberculous meningitis. Neuroradiology. 1992;34(3):197–199. doi:10.1007/BF00596334
- Kager LM, Blok DC, Lede IO, et al. Pulmonary tuberculosis induces a systemic hypercoagulable state. J Infect. 2015;70(4):324–334. doi:10.1016/j.jinf.2014.10.006
- Robson SC, White NW, Aronson I, et al. Acute-phase response and the hypercoagulable state in pulmonary tuberculosis. Br J Haematol. 1996;93(4):943–949. doi:10.1046/j.1365-2141.1996.d01-1722.x
- Ntolios P, Papanas N, Nena E, et al. Mean platelet volume as a surrogate marker for platelet activation in patients with idiopathic pulmonary fibrosis. Clin Appl Thromb Hemost. 2016;22(4):346–350. doi:10.1177/1076029615618023
- Lee MY, Kim YJ, Lee HJ, Cho SY, Park TS. Mean platelet volume in Mycobacterium tuberculosis infection. Biomed Res Int. 2016;2016:7508763. doi:10.1155/2016/7508763
- Cumpelik A, Gerossier E, Jin J, et al. Mechanism of platelet activation and hypercoagulability by Antithymocyte Globulins (ATG). Am J Transplant. 2015;15(10):2588–2601. doi:10.1111/ajt.13316
- Membre A, Wahl D, Latger-Cannard V, et al. The effect of platelet activation on the hypercoagulability induced by murine monoclonal antiphospholipid antibodies. Haematologica. 2008;93(4):566–573. doi:10.3324/haematol.12364
- Freedman J, Mody M, Lazarus AH, et al. Platelet activation and hypercoagulability following treatment with porcine factor VIII (HYATE:C). Am J Hematol. 2002;69(3):192–199. doi:10.1002/ajh.10057
- Ramos-Pachón A, López-Cancio E, Bustamante A, et al. D-dimer as predictor of large vessel occlusion in acute ischemic stroke. Stroke. 2021;52(3):852–858. doi:10.1161/STROKEAHA.120.031657
- Hou H, Xiang X, Pan Y, et al. Association of level and increase in D-dimer with all-cause death and poor functional outcome after ischemic stroke or transient ischemic attack. J Am Heart Assoc. 2021;10(3):e018600. doi:10.1161/JAHA.120.018600
- Min W, Zi-Feng J, Jian-Lin X, Hao-Hui F. Role of the fibrinogen degradation products and D-dimer in the differential diagnosis of pulmonary tuberculosis and community-acquired pneumonia. Clin Lab. 2018;64(1):135–140. doi:10.7754/Clin.Lab.2017.170720
- Gon Y, Sakaguchi M, Takasugi J, et al. Plasma D-dimer levels and ischaemic lesions in multiple vascular regions can predict occult cancer in patients with cryptogenic stroke. Eur J Neurol. 2017;24(3):503–508. doi:10.1111/ene.13234
- Seok JM, Kim SG, Kim JW, et al. Coagulopathy and embolic signal in cancer patients with ischemic stroke. Ann Neurol. 2010;68(2):213–219. doi:10.1002/ana.22050
- Chao BH, Yan F, Hua Y, et al. Stroke prevention and control system in China: CSPPC-stroke program. Int J Stroke. 2021;16(3):265–272. doi:10.1177/1747493020913557