

Abstract
Purpose
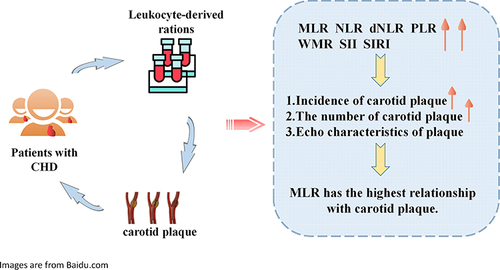
This study explored the relationship between monocyte-to-lymphocyte ratio (MLR) as well as other leukocyte-derived ratios and carotid plaques in patients with coronary heart disease (CHD).
Patients and Methods
A total of 12,093 patients with CHD were selected as research participants. Leukocyte-derived ratios assessed in this study included neutrophil-to-lymphocyte ratio (NLR), derived NLR (dNLR), MLR, platelet-to-lymphocyte ratio (PLR), white blood cell-to-mean platelet volume ratio (WMR), lymphocyte×neutrophil/104 ratio (MNM), systemic immune inflammation index (SII), and systemic inflammation response index (SIRI). Leukocyte-derived ratios were divided into four groups according to quarters. Logistic regression analysis was performed to evaluate the relationship between leukocyte-derived ratios and the incidence, number, and echo characteristics of carotid plaques in patients with CHD. Further analysis was performed after adjusting for confounding factors.
Results
Among the 12,093 participants, 71.7% had carotid plaques. After adjusting for confounding factors, MLR, NLR, dNLR, PLR, SII, SIRI, and WMR were found to be associated with carotid plaque formation. Among them, MLR had the strongest association with the incidence of carotid plaques (odd ratio[OR]:1.889; 95% confidence interval[CI]:1.406–2.539) and hyperechoic plaques (OR:2.024; 95% CI:1.481–2.767). When MLR was viewed as a categorical variable, the risk of carotid plaque formation in Q4 was 1.4 times higher than that in Q1. The relationship between MLR and carotid plaques in females (OR:2.250; 95% CI:1.458–3.473) was stronger than that in males (OR: 1.638; 95% CI:1.102–-2.436). The relationship between MLR and carotid plaques in patients younger than 65 years (OR:3.597; 95% CI:2.379–5.439) was stronger than that in those older than 65 years (OR:1.577; 95% CI:1.046–2.378).
Conclusion
Leukocyte-derived ratios were related to the incidence, number, and echo characteristics of carotid plaques. In particular, MLR, an inflammatory biomarker that encompasses innate and adaptive immunity, may be of great value in revealing the incidence and echo characteristics of plaques.
Graphical Abstract
Abbreviations
RCSCD-TCM, Retrospective Cohort Study on Adjuvant Treatment of Coronary Heart Disease Angina Pectoris With Chinese Patent Medicine; CHD, coronary heart disease; AS, atherosclerosis; CVD, cardiovascular diseases; OPCAB, Off-Pump Coronary Artery Bypass Grafting; IMT, intima-media thickness; NLR, Neutrophil-to-Lymphocyte ratio; dNLR, derived Neutrophil-to-Lymphocyte ratio; MLR, Monocyte-to-Lymphocyte ratio; PLR, Platelet-to-Lymphocyte ratio; WMR, White blood cell-to-Mean platelet volume ratio; MNM, Lymphocyte×Neutrophil/104 ratio; SII, systemic immune inflammation index; SIRI, system inflammation response index; SBP, Systolic blood pressure; DBP, Diastolic blood pressure; FBG, Fasting blood glucose; HbA1c, Glycosylated hemoglobin A1c; TC, Total cholesterol; TG, Triglycerides; HDL-C, High-density lipoprotein cholesterol; LDL-C, Low-density lipoprotein cholesterol; WBC, white blood cell; NE, Neutrophils; MO, monocyte; LYM, Lymphocyte; PLT, Platelet; BMI, body mass index; IQR, Interquartile range; OR, odds ratio; CI, confidence interval; β, regression coefficient.
Data Sharing Statement
The data supporting the research results can be obtained from the corresponding author.
Ethics Approval and Informed Consent
All research data were obtained from the hospital’s medical record system, and informed consent was not obtained. To protect patients’ privacy, the information included in our research was anonymous, and all traceable personal identifiers were deleted from the analysis dataset; hence, the need for patients’ informed consent was waived. All researchers involved in this study have the responsibility to protect patient data. All research data of this study should be kept strictly confidential, and the leaker should bear any consequences caused by leakage. This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the Tianjin University of Traditional Chinese Medicine (TJUTCM-EC2019008). It has been registered in the Clinical Trials.gov (registration number: NCT04026724), and the Chinese Clinical Trial Registration Centre (registration number: ChiCTR1900024535).
Acknowledgments
We would like to thank six hospitals in Tianjin that provided data from the First Teaching Hospital of Tianjin University of Traditional Chinese Medicine, Second Hospital of Tianjin University of Traditional Chinese Medicine, Tianjin Chest Hospital, Tianjin Nankai Hospital, Tianjin Medical University General Hospital, and Tianjin Academy of Traditional Chinese Medicine Affiliated Hospital. Mei Ma, Yijia Liu, and Lichun Wang are co-first authors for this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that there is no conflict of interest regarding the publication of this article.