
Abstract
Background
Inflammation and cardiac fibrosis are important pathogenic drivers of heart failure. The fibrosis-4 index (FIB-4) is associated with a higher degree of fibrosis. The systemic immune inflammation index (SII) is associated with a higher degree of systemic inflammation status. Previous studies have shown that they are associated with a poor prognosis for cardiovascular disease. We sought to investigate the value of FIB-4 combined with the SII as a novel inflammation-fibrosis combined index (IFCI) in predicting left ventricular reverse remodeling (LVRR) and prognosis among reduced ejection fraction heart failure (HFrEF) patients.
Methods
A total of 895 patients with HFrEF were continuously recruited. Receiver operating characteristic curves were drawn to assess the abilities of inflammation-fibrosis indicators to predict LVRR. Multivariable Cox regression analysis was used to examine independent predictors of composite cardiac events and all-cause death.
Results
After six months of follow-up, 344 (38.4%) patients experienced LVRR. The IFCI had the largest area under the curve (0.835, P < 0.001). In multivariate-adjusted logistic regression analyses, FIB-4, SII, and IFCI were predictive of LVRR (P value < 0.05). The IFCI was associated with a 3.686-fold higher risk of non-LVRR (odds ratio [OR] = 3.686, P < 0.001). Moreover, an increased IFCI predicted a poor prognosis in HFrEF patients. The highest risk of composite cardiac events (hazard ratio [HR] = 2.716, P < 0.001) was observed in the top IFCI-tertile group, and similar results were found regarding independent risk indicators of all-cause death.
Conclusion
In summary, this study indicated that increased IFCI at admission offers good predictability regarding non-LVRR and predicts the risk of all-cause mortality or composite cardiovascular events due to HFrEF patients and could be used as a novel marker.
Introduction
Heart failure (HF) is a shared serious or terminal phase in the progression of various cardiovascular diseases (CVDs) and major causes of death.Citation1,Citation2 Mild dysfunction progresses to reduced ejection fraction HF (HFrEF, left ventricular ejection fraction (LVEF) ≤ 40%) because of progressive structural remodeling.Citation3,Citation4 With significant advances in medical treatment, the beneficial effects of optimal medical therapy based on guideline-directed (GDMT) and/or device therapy promote left ventricular reverse remodeling (LVRR) and reduce the rate of readmission of HF patients, all-cause mortality, and sudden cardiac death.Citation5,Citation6 Therefore, in HFrEF patients, it is essential to predict LVRR and distinguish prognosis, thereby helping clinicians identify high-risk patients early.Citation7,Citation8 LVRR was defined as a LVEF increase of ≥ 10% or a LVEF ≥ 50% and a decrease in indexed left ventricular end-diastolic diameter (LVEDDi) of ≥ 10% or LVEDDi of ≤ 33 mm/mCitation2 at least 6 months after the initial increase.Citation9,Citation10
HF resulting from complex and multifactorial factors, including inflammation and cardiac fibrosis, is an important pathogenic driver, eventually leading to cardiac dysfunction and patient death.Citation11 In patients with HFrEF, inflammation and cardiac fibrosis have been associated with a higher risk of cardiovascular events and are proposed to hinder LVRR, thereby conferring persistent vulnerability to hospitalization for heart failure and mortality in patients.Citation12 The systemic immune inflammation index (SII) is an innovative biomarker and is an excellent indicator of the local immune response and systemic inflammation that combines information regarding three significant immune cells represented by neutrophils, lymphocytes, and platelets, defined as platelet × neutrophil/lymphocyte.Citation13 SII has been shown to be associated with a poor prognosis of cardiovascular disease and to be a better representation of the systemic inflammation status with greater stability.Citation14,Citation15 In critical patients with congestive HF, the SII is positively correlated with short-term mortality, in-hospital mortality, and a poor prognosis.Citation16,Citation17 However, the SII has not been evaluated as a prognostic indicator of LVRR in patients with HFrEF.
The fibrosis-4 index (FIB-4) is a noninvasive, simple, and economical marker to evaluate liver fibrosis and the stage of hepatic disease and is easy to obtain, calculated by age (years) × aspartate transaminase (U/L)/(platelet count (109/L) × alanine transaminase (U/L)1/2).Citation18 The FIB-4 has been reported to predict mortality and HF readmission rates in patients with acute HF, which is positively correlated with poor prognosis.Citation19 In patients with HF with preserved ejection fraction, increased FIB-4 values are also an important predictor of cardiovascular events.Citation20 It was found that FIB-4 was independently associated with both cardiac and noncardiac death after stratification of patients with HF according to LVEF value.Citation21 There is no large sample study evaluating the diagnostic and prognostic value of FIB-4 for LVRR in patients with HFrEF.
The level of systemic inflammation affects the level of myocardial fibrosis, and a high level of inflammation means a high level of fibrosis, which in turn increases the risk of death during various diseases, including HFrEF.Citation12,Citation22 We integrated FIB4 and SII, two types of hematology indicators, as a novel inflammation-fibrosis combined index (IFCI), which is composed of the fibrosis index and systemic inflammation level. It is better to combine fibrosis and inflammation indicators since both inflammation and fibrosis may be related to the disease status and prognosis in HFrEF patients. Until now, the predictive effect of IFCI on LVRR has never been investigated in patients with HFrEF. Therefore, we designed this study to determine whether IFCI could provide a new leverage to personalize the risk of LVRR and prognosis. Targeted IFCI screening of individuals with HFrEF may pave the way for future personalized preventive treatment. In view of this, the present study attempted to elucidate: first, whether FIB-4, SII and the IFCI predict LVRR after 6 months in patients with HFrEF; second, whether these indices predict subsequent prognosis.
Methods
This study protocol was approved by the Medical Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University (Approval ID: 20170605–05) and conformed to the principles and guidelines of the Declaration of Helsinki. This study was registered in the Chinese Clinical Registry Center (registration no. ChiCTR1900021055).
Study Population
In this retrospective cohort study, patients were consecutively enrolled from January 2017 to January 2021, and 2,436 consecutive patients were diagnosed with LVEF of ≤ 40% (HFrEF) at the Xinjiang Medical University First Affiliated Hospital.
The inclusion criteria were hospital admission for those who were first diagnosed prior to enrollment, LVEF ≤ 40%, New York Heart Association (NYHA) class II–IV heart failure, and optimal medical therapy based on guidelines (GDMT).Citation1,Citation23
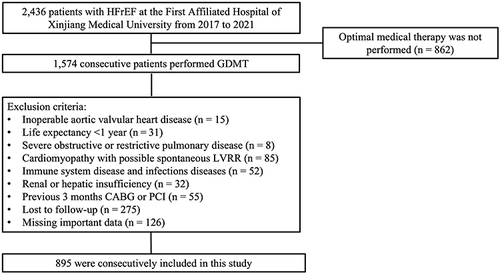
The exclusion criteria were severe renal and hepatic insufficiency defined as serum creatinine > 221 μmol/L, Child‒Pugh Class C, inoperable aortic valvular heart disease, life expectancy <1 year due to causes other than HF such as advanced cancer, cardiac transplantation or revascularization indicated or expected within 6 months, severe obstructive or restrictive pulmonary disease, coronary revascularization (PCI or CABG) within the previous 3 months, immune system disease and acute, chronic infection diseases.Citation24 Patients suffering from cardiomyopathy with possible spontaneous LVRR, such as patients suffering from tachycardia-induced cardiomyopathy, perinatal cardiomyopathy, myocarditis, and alcoholic dilated cardiomyopathy, were excluded.Citation25 In the present study, we finally enrolled 895 patients. The detailed recruitment protocol is shown in .
Figure 1 Flow chart of patient enrollment.
Clinical and Echocardiographic Variables
Baseline demographic, clinical, laboratory, and echocardiographic variables were evaluated. Clinical characteristics comprised type of HF, relevant medical history, comorbidities, and HF medication. Echocardiography was performed by a senior echocardiographer at admission and during the follow-up period and calculated according to established American Society of Echocardiography protocols.Citation26
The indices used in this study are described as follows:
was calculated based on the multivariate logistic regression model.
Study Outcomes and Endpoints
LVRR was defined as LVEF ≥ 50% or a ≥ 10% increase and LVEDDI [LVEDD/(body surface area)] ≤ 33 mm/m2 or a ≥ 10% decrease from baseline.Citation4,Citation29 The primary endpoints were composite cardiac events, including cardiac death, heart transplantation, hospitalization due to worsening heart failure, and lethal arrhythmia (hospitalization for sustained ventricular tachycardia or ventricular fibrillation). The secondary endpoint was all-cause mortality.
Statistical Analysis
The normality test was checked using the Shapiro–Wilk test for the continuous variables.Continuous variables were presented as mean ± standard deviations (SD) in cases of meeting the normality distribution or as median (quartiles Q1–Q3) in cases of not meeting the normality distribution. The parametric Student’s t-test and the non-parametric Mann–Whitney U-test were performed to compare the differences between the two groups. Classified data are presented as proportions and were evaluated by the chi-square test. The levels of biomarkers such as FIB-4, SII, IFCI and NT-pro-BNP and serum creatine were log10 transformed.
Receiver operating characteristic (ROC) curves were constructed, and the areas under the curves (AUC) were measured to estimate the ability of the FIB-4, SII and IFCI to predict LVRR. Combined ROC analysis based on the multivariate logistic regression model was conducted for the IFCI. Moreover, the comparisons of AUC values were performed using the DeLong test. To test whether IFCI improved LVRR prediction of the other clinical parameters, we used the continuous net reclassification index (NRI) and the integrated discrimination improvement (IDI).
Logistic regression analyses were performed to find the relationship between LVRR and FIB-4, SII and IFCI. Potential nonlinear associations between the levels of IFCI and the incidence of LVRR were examined with restricted cubic splines. Then, the IFCI was categorized into three groups according to the tertile points. The comparison of measurement data among tertiles of IFCI groups was based on one-way ANOVA.
Kaplan‒Meier analysis was used to compare the probability of composite cardiac events and all-cause mortality with HFrEF patients. Univariate and multivariable Cox regressions were used to analyze factors related to composite cardiac events and all-cause death. To avoid model overfitting, only parameters significantly associated with outcome in the univariate analyses were included in the multivariate Cox regression model performed using step-down procedures.
All statistical analyses were performed using SPSS version 26.0 (SPSS Inc., Chicago, IL, USA) and R software (version 4.0.1). A P value < 0.05 was considered statistically significant.
Results
Comparison of Baseline Characteristics
A total of 895 patients were divided into 2 groups according to whether they had LVRR. By 6 months of GDMT treatment, 344 (38.4%) patients were experiencing LVRR. An ischemic etiology of HF was present in 356 (39.8%) patients, and more ischemic cases were present in the non-LVRR group (48.6% vs 25.6%). Compared to non-LVRR patients, the prevalence rates of hypertension, coronary heart disease and diabetes mellitus were significantly higher in LVRR patients with heart failure (P < 0.05). Baseline laboratory results, including FIB-4 (2.30 [1.58, 6.41] vs 1.16 [0.62, 1.82], P < 0.001), SII (678.71 [440.14, 985.33] vs 395.98 [216.05, 604.76], P < 0.001) and NT-pro BNP (3320.00 [744.00, 5650.00] vs 813.00 [226.50, 3642.50], P < 0.001), were higher in non-LVRR patients than in LVRR patients. The available echocardiographic data at baseline and at the 6-month follow-up are included in . Compared to LVRR, the mean LVEDDi at baseline was 36.11 ± 5.43 mm/m2 (35.54 ± 5.37 vs 36.49 ± 5.45 mm/m2, P = 0.038), with a mean LVEF of 34.44 ± 5.05% (33.66 ± 4.65 vs 34.93 ± 5.24, P = 0.001).
Table 1 Baseline Characteristics of the Study Population
The FIB-4, SII and IFCI Were Able to Predict LVRR
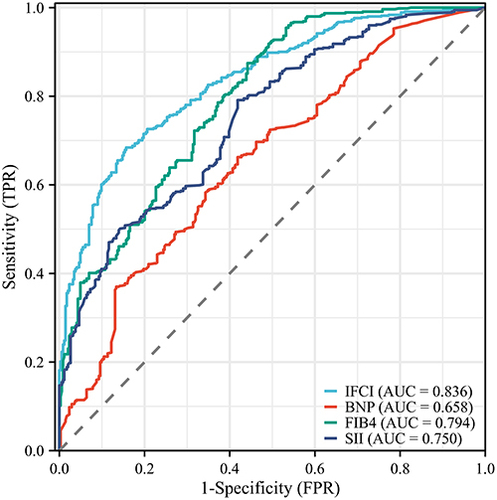
The performance of the predictive indicators is shown in . According to the results obtained for ROC analysis (), the AUCs for FIB4, SII, NT-pro BNP and IFCI were 0.794 (95% CI: 0.764–0.824), 0.750 (95% CI: 0.718–0.782), 0.658 (95% CI: 0.621–0.695) and 0.835 (95% CI: 0.809–0.860), respectively. The IFCI exhibited the largest AUC of all the scores (both P values < 0.01). After the DeLong test, the predictive ability of the IFCI was confirmed as being significantly higher than that of the other indicators, FIB4, SII and NT-pro BNP (Z value = 3.474, 7.715 and 7.597, respectively). The AIC decreased in IFCI to FIB-4, SII and NT-proBNP (IFCI: 874.69 vs FIB4: 985.14 vs SII:1016.56 vs 1155.88), which showed that IFCI improved the calibration of the predictive LVRR. Moreover, compared with NT-proBNP, the IFCI, FIB4 and SII have better predictive ability (IDI = 0.265, 0.151 and 0.121, both P values < 0.01; NRI = 0.864, 0.653, and 0.456, both P values < 0.01).
Table 2 The Predicting Ability of FIB-4, SII and IFCI with the LVRR
Figure 2 Receiver operating characteristic curves for FIB-4, SII, NT-proBNP and IFCI in predicting the incidence of LVRR.
Elevated FIB-4, SII and IFCI are Independent Risk Indicators for Non-LVRR
After adjusting for several potential risk indicators, such as type of heart failure, symptom duration, medical history, and baseline GDMT treatment, the SII (adjusted OR=1.003, 95% CI 1.002–1.004, P < 0.001), FIB-4 (adjusted OR = 1.778, 95% CI 1.567–2.018, P < 0.001), IFCI (adjusted OR = 3.686, 95% CI 2.937–4.627, P < 0.001), and log-NT-pro BNP (adjusted OR = 2.468, 95% CI 1.957–3.113, P < 0.001) remained independent risk indicators in the non-LVRR group ().
Table 3 Elevated Value of FIB-4, SII and IFCI are Independent Risk Factors of Non-LVRR
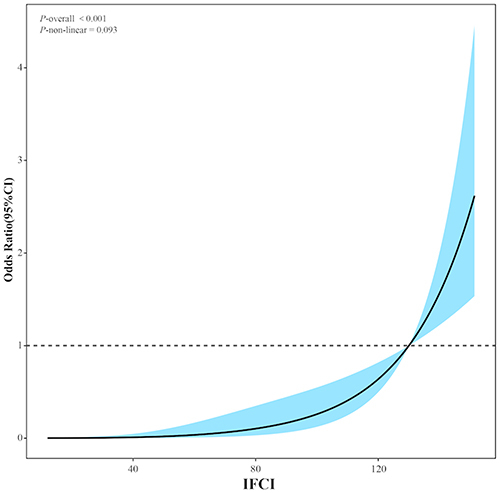
To characterize the relationship between IFCI and the odds ratio for LVRR at the 6-month follow-up, a spline curve was fitted in adjustment for a potential confounder model, which demonstrated there is significant relationship between IFCI levels and LVRR and had linear association (). The study population was stratified according to IFCI tertiles: the baseline tertiles of the IFCI (group 1: <37.94, group 2: 37.94–59.03, group 3: ≥59.03). All participants were categorized into 3 groups. The clinical characteristics of the 3 groups are shown in . Patients in the top IFCI tertiles group had higher levels of age, symptom duration of HF, medical history of coronary heart disease, LVEDD, LVEDDi, LVESD and NT-pro BNP and lower levels of LVEF; moreover, this group exhibited the highest incidence of composite cardiac events and mortality (all P values <0.05). Making the IFCI a categorical variable (tertiles analysis), compared to the lower tertiles, the top tertile group exhibited the highest OR of incident non-LVRR [30.792 (18.346–51.356), P < 0.001] after adjusting for potential risk indicators.
Table 4 Baseline Characteristics of Study Population According to Tertiles of Inflammation-Fibrosis Combined Index
Figure 3 Spline curve plotting baseline IFCI against the odds ratio o of non-LVRR.
Increased IFCI Predicts Poor Prognosis in HFrEF Patients
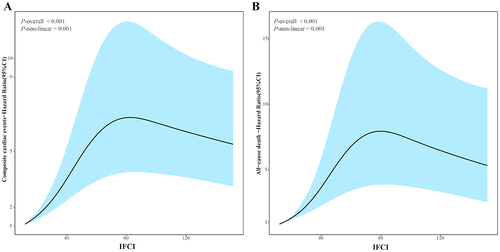
During a median of 17 (Q1:9 ~ Q3:29) months of follow-up, 331 (37.0%) patients had composite cardiac events, and 160 (17.9%) died from any cause. By applying a cubic spline curve, we attempted to explore a potential association between poor prognosis and IFCI. After conducting significance testing, it was determined that there is significant relationship between the IFCI levels and poor prognosis, including composite cardiac events and all-cause death. In addition, it was found that poor prognosis had a nonlinear association with IFCI levels. The illustrates the specific results.
Figure 4 Spline curve plotting baseline IFCI against the Hazard ratio odds ratio of poor prognosis, including composite cardiac events (A) and all-cause death (B).
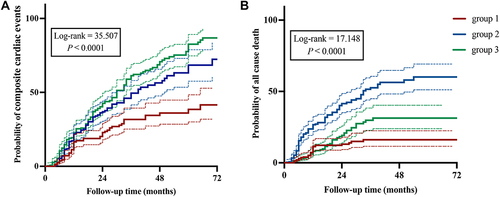
Patients in the top tertiles of the IFCI had a significantly increased risk of composite cardiac events compared with other groups, as demonstrated in (log-rank χ2 = 35.507, P <0.001) and an increased risk of all-cause mortality (log-rank χ2 = 17.148, P <0.001).
Figure 5 Kaplan‒Meier curves. Probability of a composite endpoint(A) and all causes of death (B) in the IFCI tertile groups.
After adjusting for several potential risk indicators, such as type of heart failure, symptom duration, medical history, and baseline GDMT treatment, the values of SII (adjusted HR=2.212, 95% CI 1.520–3.218, P < 0.001), FIB-4 (adjusted HR = 1.052, 95% CI 1.019–1.086, P = 0.002), IFCI (adjusted HR = 1.007, 95% CI 1.004–1.010, P < 0.001), and NT-pro BNP (adjusted HR = 1.270, 95% CI 1.080–1.492, P = 0.004) remained independent risk indicators of composite cardiac events. When the IFCI was made a categorical variable (tertiles analysis), compared to the first tertiles, the top tertile group exhibited the highest HR of incident composite cardiac events [2.716 (1.777–4.151), P < 0.001] after adjusting for potential risk indicators, and similar results were seen regarding the independent risk indicators of all-cause death ().
Table 5 Elevated Value of Inflammation-Fibrosis Combined Index are Independent Risk Factors of Poor Prognosis in HFrEF Patients
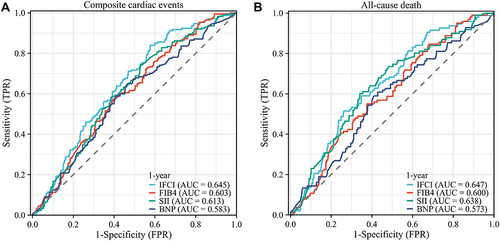
The performance of predicting 1-year prognostic ability, including composite cardiac events and all-cause death, of NT-pro BNP, IFCI, FIB4 and SII is shown in . According to the results obtained for the time-dependent ROC curves, the IFCI exhibited the largest AUC of all the scores (both P values < 0.01). The AIC decreased in IFCI to FIB-4, SII and NT-proBNP, which showed that IFCI improved the calibration of the 1-year prognosis, including composite cardiac events and all-cause death. Moreover, compared with NT-proBNP, the IFCI has better predictive ability for the 1-year prognosis of the 1-year prognosis, including composite cardiac events and all-cause death. Compared with NT-pro BNP, the predictive ability of FIB4 and SII was not significantly different ().
Table 6 The Predicting Ability of FIB-4, SII and IFCI with the 1-Year Prognostic
Figure 6 Time-dependent ROC curves for FIB-4, SII, NT-proBNP and IFCI in predicting the incidence of a composite endpoint (A) and all causes of death (B) in 1 year.
Discussion
To our knowledge, this is the first study to demonstrate that (1) the FIB-4, SII and IFCI at admission provided good predictability of LVRR after 6 months of GDMT treatment. (2) Lower levels of FIB-4, SII and IFCI were also identified as reduced independent risk indicators for non-LVRR, all-cause death and composite cardiac events. In addition, the IFCI was the strongest predictor of non-LVRR, and an increased IFCI predicted poor prognosis. Furthermore, this study is the first to report the association between the IFCI and LVRR in patients with HFrEF.
In general, LVRR involves restoring chamber geometry and improving chamber contractility, as well as beneficial changes in molecular, metabolic, and extracellular matrix. Increased inflammation has been proposed as a predictor of impaired LVRR because the activation of inflammatory cells and responses results in the secretion of proinflammatory cytokines, further enhancing the inflammatory state in the progression of HF.Citation30,Citation31 In this study, the SII could be used to predict LVRR after 6 months of GDMT treatment. After adjusting for confounding factors, increased SII was also identified as an independent risk factor for non-LVRR and was predictive of poor prognosis in patients with HF. The mechanisms of the relationship between the SII and LVRR and adverse prognosis in HF patients remain unclear. A substantial number of neutrophils were found in myocardial tissue in a model of HF, and elevated neutrophils were associated with cardiovascular outcomes, leading to myocardial infarction and cardiac death.Citation32–34 Aside from increased levels of neutrophils, increasing platelet levels also contribute to SII elevation. PLTs are related to atherosclerosis, coronary artery disease, cerebrovascular disease, and systemic inflammatory disorders, all of which contribute to the pathogenesis of HF.Citation35–37 Furthermore, significant abnormalities caused by HF lead to decreased levels of lymphocytes, resulting in an elevated value of the SII. First, lymphocyte counts in patients with HF were found to be lower than those in the normal population, and lymphopenia serves as an independent predictor of poor cardiovascular outcomes in patients with chronic and advanced HF.Citation38,Citation39 A 36-month follow-up study of myocardial infarction found that patients with low lymphocyte counts within 96 hours of admission had an elevated risk of serious cardiovascular events.Citation40,Citation41 However, the role of the platelet count in the two formulas was the opposite. We therefore analyzed the correlation between each of the components of the formula and the prognosis of HFrEF. We found that there was a significant correlation and a consistent trend for neutrophil count, ALT and AST, while there was no significant correlation for platelet count. Overall, the SII has a higher predictive value as a biomarker than a single leukocyte subtype indicator due to its ability to reflect the balance of platelets and lymphocytes in the body as well as the overall immune response in patients with HF. Regarding its role as a novel biomarker, using the SII is simple and fast, involving an inexpensive routine blood examination for almost all hospitalized patients. Compared with NT-proBNP, the SII enables more effective identification of high-risk patients as well as the prediction of prognosis without additional cost; it has broad application prospects.
HF is caused by cardiac remodeling as a result of cardiac inflammation and fibrosis.Citation42 Both cardiac inflammation and fibrosis could be targets of new heart failure therapies.Citation43 In patients with HF, the FIB‐4 index increased with NT‐pro‐BNP and right atrial pressure, and a high FIB‐4 was associated with an increase in all‐cause mortality in acute HF.Citation44–46 Our results indicate that FIB-4 is both a biomarker of LVRR and a predictor of cardiovascular events in HFrEF patients. However, the possible mechanism by which FIB-4 is predictive of prognosis in HF patients has not been fully clarified. Liver dysfunction and cardiac dysfunction are thought to interact mutually. HFrEF often causes liver dysfunction or abnormal liver enzyme levels and leads to systemic venous congestion and arterial perfusion reduction, resulting in cardiac cirrhosis and cardiogenic hypoxic hepatitis.Citation47 Dysfunction and fibrosis of the liver increase the risk of heart failure and decrease prodrug transformation into active metabolites (eg, some ACE inhibitors and ARBs, enalapril, fosinopril, and losartan).Citation48 This is why some patients cannot tolerate medication treatment or why the effect of the pharmaceutical is poor. A shortage of drug tolerance will result in center-of-gravity failure, triggering a vicious cycle. Additionally, hepatic fibrosis is associated with CVD pathogenesis through different mechanisms, and increased plasma inflammatory mediators play a substantial role. This is one reason why readily accessible markers for liver fibrosis might also be used as indicators for cardiac fibrosis, which is why the evaluation of FIB-4 in this study was recommended.Citation49 At the same time, calculating FIB-4 is quick and straightforward, and the FIB-4 results are available immediately.
In a large cohort of patients with HFrEF, this study indicated that an increased IFCI at admission offers good predictability regarding non-LVRR and predicts the risk of all-cause mortality or composite cardiovascular events in patients with HFrEF. It may be used as a promising biomarker. Therefore, the IFCI reflects key processes such as inflammation and cardiac remodeling in patients with HFrEF and has been shown to have incremental prognostic value over NT-proBNP, the gold standard biomarker in HF. This further denotes several different underlying pathophysiological pathways that contribute to HF progression and suggests that the IFCI as a marker provides additional information compared with NT-proBNP.Citation50 HF remains a complex disease, but even though IFCI is representative of several pathological conditions, it enables us to elucidate the disease status of HF and its impact on prognosis. Notably, the IFCI exhibits less intraindividual biological variation than NT-proBNP. Therefore, applying a combination of biomarkers would more reliably predict risk at the individual patient level than relying on a single marker.
Study Limitations
First, the single-center, retrospective cohort design was an inherent limitation. Second, after adjusting for well-established predictive indicators, the remaining confounding factors cannot be entirely ruled out because the three groups (low, medium, and high groups) had a wide range of baseline variations in characteristics. Therefore, large-scale prospective randomized studies are needed to further determine the impact of these indices on the LVRR. At the time of study conduction, SGLT2 inhibitor (SLGT2i) therapy and ARN inhibitor (ARNi) therapy were not part of standard GDMT. Treatment of HFrEF with SGLT2i and ARNi has been associated with a reduction in sudden death and improved LVEF and could therefore also affect our results.Citation51 In the end, the study neglects to evaluate the burden of comorbidity and thromboembolic risk for HFrEF patients.Citation52,Citation53
Conclusion
In a large cohort of patients with HFrEF, this study indicated that an increased inflammation-fibrosis combined index at admission offers good predictability regarding non-LVRR and predicts the risk of all-cause mortality or composite cardiovascular events in patients with HFrEF. It may be used as a promising biomarker that may complement or even outperform traditional markers, such as N-terminal pro-brain natriuretic peptide.
Ethics Approval and Statement
This study protocol was approved by the Medical Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University (Approval ID: 20170605-05).
To preserve patient privacy and data confidentiality, patient data have been identified before analysis. All analyses in this retrospective study were performed based on the data from anonymized patients. Due to the retrospective nature of this study, the Ethics Committee of First Affiliated Hospital of Xinjiang Medical University approved the study and determined that written informed consent was not required.
Consent to Participate (Include Appropriate Statements)
Due to the retrospective design of this study, informed consent was not required.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that there are no competing interests associated with this manuscript.
Data Sharing Statement
Data of this study were available from the corresponding author upon request.
Additional information
Funding
References
- McDonagh TA, Metra M, Adamo M, et al. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599–3726. doi:10.1093/eurheartj/ehab368
- Yancy CW, Jessup M, Bozkurt B, et al. ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American college of cardiology/American heart association task force on clinical practice guidelines and the heart failure society of America. J Am Coll Cardiol. 2017;70(6):776–803. doi:10.1016/j.jacc.2017.04.025
- Cescau A, Van Aelst LNL, Baudet M, Cohen Solal A, Logeart D. High body mass index is a predictor of left ventricular reverse remodelling in heart failure with reduced ejection fraction. ESC Heart Fail. 2017;4(4):686–689. doi:10.1002/ehf2.12172
- Merlo M, Pyxaras SA, Pinamonti B, Barbati G, Di Lenarda A, Sinagra G. Prevalence and prognostic significance of left ventricular reverse remodeling in dilated cardiomyopathy receiving tailored medical treatment. J Am Coll Cardiol. 2011;57(13):1468–1476. doi:10.1016/j.jacc.2010.11.030
- Januzzi JL Jr, Prescott MF, Butler J, et al. Association of change in n-terminal pro-b-type natriuretic peptide following initiation of sacubitril-valsartan treatment with cardiac structure and function in patients with heart failure with reduced ejection fraction. JAMA. 2019;322(11):1085–1095. doi:10.1001/jama.2019.12821
- Wang Y, Zhou R, Lu C, Chen Q, Xu T, Li D. Effects of the angiotensin-receptor neprilysin inhibitor on cardiac reverse remodeling: meta-analysis. J Am Heart Assoc. 2019;8(13):e012272. doi:10.1161/jaha.119.012272
- Savarese G, Vedin O, D’Amario D, et al. Prevalence and prognostic implications of longitudinal ejection fraction change in heart failure. JACC Heart Fail. 2019;7(4):306–317. doi:10.1016/j.jchf.2018.11.019
- Aimo A, Vergaro G, González A, et al. Cardiac remodelling - Part 2: clinical, imaging and laboratory findings. A review from the Study group on biomarkers of the Heart failure association of the European society of cardiology. Eur J Heart Fail. 2022;24(6):944–958. doi:10.1002/ejhf.2522
- Hazebroek MR, Moors S, Dennert R, et al. Prognostic Relevance of gene-environment interactions in patients with dilated cardiomyopathy: applying the MOGE(S) Classification. J Am Coll Cardiol. 2015;66(12):1313–1323. doi:10.1016/j.jacc.2015.07.023
- Packer M, McMurray JJV. Rapid evidence-based sequencing of foundational drugs for heart failure and a reduced ejection fraction. Eur J Heart Fail. 2021;23(6):882–894. doi:10.1002/ejhf.2149
- Dick SA, Epelman S. Chronic heart failure and inflammation: what do we really know? Circ Res. 2016;119(1):159–176. doi:10.1161/circresaha.116.308030
- Wang M, Pan W, Xu Y, Zhang J, Wan J, Jiang H. Microglia-mediated neuroinflammation: a potential target for the treatment of cardiovascular diseases. J Inflamm Res. 2022;15:3083–3094. doi:10.2147/jir.S350109
- Wang BL, Tian L, Gao XH, et al. Dynamic change of the systemic immune inflammation index predicts the prognosis of patients with hepatocellular carcinoma after curative resection. Clin Chem Lab Med. 2016;54(12):1963–1969. doi:10.1515/cclm-2015-1191
- Yang YL, Wu CH, Hsu PF, et al. Systemic immune-inflammation index (SII) predicted clinical outcome in patients with coronary artery disease. Eur J Clin Invest. 2020;50(5):e13230. doi:10.1111/eci.13230
- Agus HZ, Kahraman S, Arslan C, et al. Systemic immune-inflammation index predicts mortality in infective endocarditis. J Saudi Heart Assoc. 2020;32(1):58–64. doi:10.37616/2212-5043.1010
- Tang Y, Zeng X, Feng Y, et al. Association of systemic immune-inflammation index with short-term mortality of congestive heart failure: a Retrospective Cohort study. Front Cardiovasc Med. 2021;8:753133. doi:10.3389/fcvm.2021.753133
- Yuan M, Ren F, Gao D. The value of sii in predicting the mortality of patients with heart failure. Dis Markers. 2022;2022:3455372. doi:10.1155/2022/3455372
- Shibata N, Kondo T, Kazama S, et al. Impact of predictive value of Fibrosis-4 index in patients hospitalized for acute heart failure. Int J Cardiol. 2021;324:90–95. doi:10.1016/j.ijcard.2020.09.056
- Kawahira M, Tamaki S, Yamada T, et al. Prognostic value of impaired hepato-renal function and liver fibrosis in patients admitted for acute heart failure. ESC Heart Fail. 2021;8(2):1274–1283. doi:10.1002/ehf2.13195
- Takae M, Fujisue K, Yamamoto E, et al. Prognostic significance of liver stiffness assessed by fibrosis-4 index in patients with heart failure. ESC Heart Fail. 2021;8(5):3809–3821. doi:10.1002/ehf2.13351
- Shirakabe A, Okazaki H, Matsushita M, et al. Type III procollagen peptide level can indicate liver dysfunction associated with volume overload in acute heart failure. ESC Heart Fail. 2022;9(3):1832–1843. doi:10.1002/ehf2.13878
- Mann DL. Innate immunity and the failing heart: the cytokine hypothesis revisited. Circ Res. 2015;116(7):1254–1268. doi:10.1161/circresaha.116.302317
- Crespo-Leiro MG, Anker SD, Maggioni AP, et al. European society of cardiology heart failure long-term registry (ESC-HF-LT): 1-year follow-up outcomes and differences across regions. Eur J Heart Fail. 2016;18(6):613–625. doi:10.1002/ejhf.566
- Shah R, Ziegler O, Yeri A, et al. MicroRNAs associated with reverse left ventricular remodeling in humans identify pathways of heart failure progression. Circ Heart Fail. 2018;11(2):e004278. doi:10.1161/circheartfailure.117.004278
- Hellawell JL, Margulies KB. Myocardial reverse remodeling. Cardiovasc Ther. 2012;30(3):172–181. doi:10.1111/j.1755-5922.2010.00247.x
- Lang RM, Bierig M, Devereux RB, et al. Recommendations for chamber quantification: a report from the American society of echocardiography’s guidelines and standards committee and the chamber quantification writing group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005;18(12):1440–1463. doi:10.1016/j.echo.2005.10.005
- Sterling RK, Lissen E, Clumeck N, et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology. 2006;43(6):1317–1325. doi:10.1002/hep.21178
- Hu B, Yang XR, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20(23):6212–6222. doi:10.1158/1078-0432.Ccr-14-0442
- Hnat T, Veselka J, Honek J. Left ventricular reverse remodelling and its predictors in non-ischaemic cardiomyopathy. ESC Heart Fail. 2022;9(4):2070–2083. doi:10.1002/ehf2.13939
- Hanna A, Frangogiannis NG. Inflammatory Cytokines and Chemokines as Therapeutic Targets in Heart Failure. Cardiovasc Drugs Ther. 2020;34(6):849–863. doi:10.1007/s10557-020-07071-0
- Halade GV, Lee DH. Inflammation and resolution signaling in cardiac repair and heart failure. EBioMedicine. 2022;79:103992. doi:10.1016/j.ebiom.2022.103992
- Wang Y, Sano S, Oshima K, et al. Wnt5a-mediated neutrophil recruitment has an obligatory role in pressure overload-induced cardiac dysfunction. Circulation. 2019;140(6):487–499. doi:10.1161/circulationaha.118.038820
- Valiente-Alandi I, Potter SJ, Salvador AM, et al. Inhibiting fibronectin attenuates fibrosis and improves cardiac function in a model of heart failure. Circulation. 2018;138(12):1236–1252. doi:10.1161/circulationaha.118.034609
- Ndumele CE, Coresh J, Lazo M, et al. Obesity, subclinical myocardial injury, and incident heart failure. JACC Heart Fail. 2014;2(6):600–607. doi:10.1016/j.jchf.2014.05.017
- Soydinc S, Turkbeyler IH, Pehlivan Y, et al. Mean platelet volume seems to be a valuable marker in patients with systemic sclerosis. Inflammation. 2014;37(1):100–106. doi:10.1007/s10753-013-9716-x
- Mehta J, Mehta P. Platelet function studies in heart disease. VI. Enhanced platelet aggregate formation activity in congestive heart failure: inhibition by sodium nitroprusside. Circulation. 1979;60(3):497–503. doi:10.1161/01.cir.60.3.497
- Ponikowski P, Voors AA, Anker SD, et al. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37(27):2129–2200. doi:10.1093/eurheartj/ehw128
- Charach G, Grosskopf I, Roth A, et al. Usefulness of total lymphocyte count as predictor of outcome in patients with chronic heart failure. Am J Cardiol. 2011;107(9):1353–1356. doi:10.1016/j.amjcard.2010.12.049
- Vaduganathan M, Ambrosy AP, Greene SJ, et al. Predictive value of low relative lymphocyte count in patients hospitalized for heart failure with reduced ejection fraction: insights from the EVEREST trial. Circ Heart Fail. 2012;5(6):750–758. doi:10.1161/circheartfailure.112.970525
- Targher G, Dauriz M, Tavazzi L, et al. Prognostic impact of in-hospital hyperglycemia in hospitalized patients with acute heart failure: results of the IN-HF (Italian Network on Heart Failure) outcome registry. Int J Cardiol. 2016;203:587–593. doi:10.1016/j.ijcard.2015.10.207
- Núñez J, Núñez E, Miñana G, et al. Effectiveness of the relative lymphocyte count to predict one-year mortality in patients with acute heart failure. Am J Cardiol. 2011;107(7):1034–1039. doi:10.1016/j.amjcard.2010.11.029
- Burchfield JS, Xie M, Hill JA. Pathological ventricular remodeling: mechanisms: part 1 of 2. Circulation. 2013;128(4):388–400. doi:10.1161/circulationaha.113.001878
- Bacmeister L, Schwarzl M, Warnke S, et al. Inflammation and fibrosis in murine models of heart failure. Basic Res Cardiol. 2019;114(3):19. doi:10.1007/s00395-019-0722-5
- Nakashima M, Sakuragi S, Miyoshi T, et al. Fibrosis-4 index reflects right ventricular function and prognosis in heart failure with preserved ejection fraction. ESC Heart Fail. 2021;8(3):2240–2247. doi:10.1002/ehf2.13317
- Maeda D, Sakane K, Ito T, Kanzaki Y, Sohmiya K, Hoshiga M. Fibrosis-4 index reflects right-sided filling pressure in patients with heart failure. Heart Vessels. 2020;35(3):376–383. doi:10.1007/s00380-019-01505-y
- Sato Y, Yoshihisa A, Kanno Y, et al. Liver stiffness assessed by Fibrosis-4 index predicts mortality in patients with heart failure. Open Heart. 2017;4(1):e000598. doi:10.1136/openhrt-2017-000598
- Møller S, Bernardi M. Interactions of the heart and the liver. Eur Heart J. 2013;34(36):2804–2811. doi:10.1093/eurheartj/eht246
- Ouwerkerk W, Voors AA, Anker SD, et al. Determinants and clinical outcome of uptitration of ACE-inhibitors and beta-blockers in patients with heart failure: a prospective European study. Eur Heart J. 2017;38(24):1883–1890. doi:10.1093/eurheartj/ehx026
- Anstee QM, Mantovani A, Tilg H, Targher G. Risk of cardiomyopathy and cardiac arrhythmias in patients with nonalcoholic fatty liver disease. Nat Rev Gastroenterol Hepatol. 2018;15(7):425–439. doi:10.1038/s41575-018-0010-0
- Vickery S, Price CP, John RI, et al. B-type natriuretic peptide (BNP) and amino-terminal proBNP in patients with CKD: relationship to renal function and left ventricular hypertrophy. Am J Kidney Dis. 2005;46(4):610–620. doi:10.1053/j.ajkd.2005.06.017
- McMurray JJV, Solomon SD, Inzucchi SE, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019;381(21):1995–2008. doi:10.1056/NEJMoa1911303
- Wei D, Sun Y, Chen R, Meng Y, Wu W. The Charlson comorbidity index and short-term readmission in patients with heart failure: a retrospective cohort study. Medicine (Baltimore). 2023;102(6):e32953. doi:10.1097/md.0000000000032953
- Sonaglioni A, Lonati C, Rigamonti E, et al. CHA(2)DS(2)-VASc score stratifies mortality risk in heart failure patients aged 75 years and older with and without atrial fibrillation. Aging Clin Exp Res. 2022;34(7):1707–1720. doi:10.1007/s40520-022-02107-x