
Abstract
Introduction and objective
The diagnosis of primary headaches is based on the International Classification of Headache Disorders (ICHD-3). Cluster headache (CH), a debilitating primary headache, is often misdiagnosed as migraine. In the absence of biological markers, a new visual screening tool with images depicting pain could aid the correct diagnosis of CH. The objective of the study is to test the tool on healthy participants and participants with CH and migraine.
Methods
In phase 1, 6 images portraying people with pain were tested on 150 healthy participants. The healthy participants were asked to rate the images as mild, moderate, severe or excruciating pain. In phase 2, the images were further tested on 116 participants with headache (16 participants with CH, 100 participants with migraine). The participants were recruited prospectively from a tertiary headache center between February and May 2017. The participants were asked to choose which image best illustrated their headache attacks.
Results
Phase 1 results showed that the images represent a range of headache pain severities from mild to excruciating as rated by healthy participants. They rated two images as excruciating, one image as severe, one image as moderate/severe, one image as moderate and one image as mild. Phase 2 results showed that two-thirds of participants with CH (69%) and half of the participants with migraine (52%) chose an image described as excruciating by the healthy participants.
Conclusion
We developed a screening tool with six drawings depicting headache pain severities from mild to excruciating as rated by the healthy participants. Although the images did not differentiate between CH and migraine, the study indicated the potential of using visual aids to assess headache severity.
Introduction
Headache disorders are the second leading cause of years lived with a disability worldwide and interventions are urgently needed to reduce this burden throughout the world.Citation1 Cluster headache (CH), a severe primary headache,Citation2 is often referred as “suicide headache” because of the suicide rate among CH sufferers.Citation3 Females with CH have described their cluster attacks as worse than childbirth.Citation4 Although CH is not a rare condition, with a prevalence (1/1000)Citation5 similar to the prevalence of multiple sclerosis (0.9/1000)Citation6 and Parkinson’s disease (1–3/1000),Citation7 it is not well known across both primary and secondary health care settings and therefore often misdiagnosed.Citation8 It is difficult for health professionals who are non-headache specialists to diagnose CH.Citation8 The delays in diagnosis and misdiagnosis (and subsequent mistreatment) occurs primarily because CH is confused with migraine.Citation9,Citation10 Migraine patients describe the headache pain as moderate and severe, during an attack they prefer to lie down in a dark room and avoid physical activity.Citation11 The intensity of migraine attack develops over hours and can last up to three days.Citation2,Citation12 In contrast to migraine, the pain intensity of CH is excruciating and is described as one of the most painful conditions known to mankind.Citation13 A CH attack starts abruptly and usually ends within three hours, these are associated with severe restlessness during the attacks.Citation5 A correct diagnosis is important as CH and migraine are managed differently.Citation14 CH is treated with high flow oxygen, subcutaneous triptans as abortive medication and verapamil as preventative treatment.Citation15 Migraine attacks are treated with oral triptans and tricyclic antidepressants, and b-blockers or antiepileptic medication to prevent attacks from occurring.Citation16
To date, there is only limited research evidence on visual aids during headacheCitation17 or pain consultations.Citation18–Citation20 One study explored the usefulness of a visual diagnostic aid for paediatric headaches.Citation17 Drawings made by children of their headache pain and associated symptoms (eg vomiting, sensitivity to lights, visual aura) were found to be useful to differentiate migraine from non-migraine headache.Citation17 Other studies found that laminated photographs suggestive of pain could improve the communication during pain consultations.Citation18–Citation20 To date, the diagnosis of CH is based on clinical historyCitation2 and there are no biological markers.Citation21 In the absence of such biomarkers, a new visual screening tool with images representing different pain severities could aid health professionals in assessing whether the patient suffers from migraine or CH and decrease common misdiagnosis and delays in diagnosis.
There are two things that lay at the inceptions of this study. Firstly, a small interview study conducted by FA in our research team, in which CH and migraine patients were interviewed and a set of images was used to identity their symptoms and capture their verbal description of pain.Citation22 Secondly, the ARTe Cluster Project, led by Claudio Geraci, that collects and exhibits artistic renditions of CH to raise awareness of the huge impact the disease has on CH sufferers.Citation23,Citation24 We developed the visual screening tool with two objectives in mind: (1) to determine if six images depict are range of pain severities from mild to excruciating. This was achieved by asking healthy participants to score the images; (2) to test the visual tool on participants with CH and migraine to determine which image best represented the pain during their headache attacks.
Methods
Screening tool development
We decided to use a range of images that depict headache pain in different ways, inspired on real life pictures and images frequently used on CH websites.Citation24 The same person sketched six drawings as we wanted all the images to have similar characteristics (color saturation and chromatic range) in order to avoid the influence of color on attentional bias.Citation25 All images were printed in black-and-white on the same size.
Phase 1
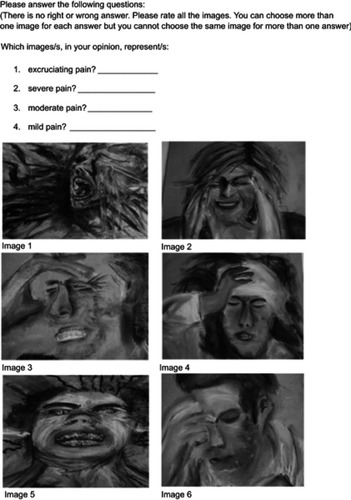
The screening tool was tested on 150 healthy participants to determine if the images depict a range of pain severities. These were people without a history of headaches or chronic pain conditions. The healthy participants were asked to rate each image as showing mild, moderate, severe or excruciating pain. They had the option to choose multiple answers or not to answer ().
Figure 1 Visual tool tested on healthy participants.
Phase 2
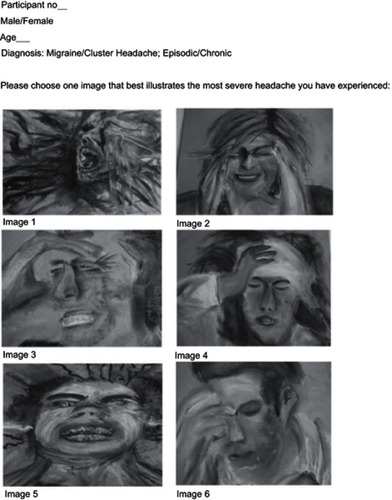
The screening tool was further tested on 116 participants with headache (16 participants with CH, 100 participants with migraine). Participants received a prior diagnosis of CH or migraine (control group) based on the ICHD-3bCitation26 criteria before they were enrolled in the study. The participants were recruited prospectively from a tertiary headache center between February-May 2017. The participants were asked to choose which image best illustrated their headache attacks ().
Figure 2 Visual tool tested on participants with cluster headache and migraine.
Ethics
This study received ethical approvals from the local University of Hull Research Ethics Committee (1613/27.09.2016) and from the UK Health and Social Care Research Ethics Committee (HSC REC) (16/NI/0269). Written informed consent was obtained from all participants before taking part in the study.
Results
Phase 1
One hundred and fifty healthy participants were included in the study. Our findings are that the participants agreed that the six images in the screening tool are depicting a range of pain severities from mild to excruciating ( and ). The participants rated image 1 (n=131/150, 87%) and 5 (n=93/150; 63%) as “excruciating”. Twenty-one percent (n=32/150) of the participants chose not to rate image 5. Therefore, image 1 seems to be more representative for expressing an excruciating level of pain. Image 2 was rated as either moderate (n=60/150; 40%) or severe (n=59/150; 39%). The participants rated image 3 (n=93/150; 62%), image 4 (n=88/150; 58%) and image 6 (n=129/150; 86%) as showing severe, moderate and mild level of pain respectively.
Figure 3 Image selection by healthy participants.
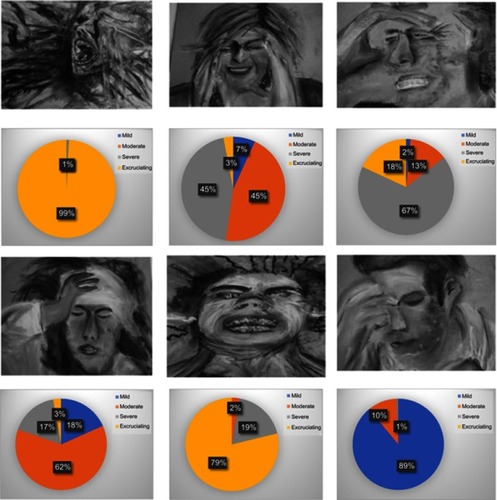
Table 1 Image rating according to severity
Phase 2
One hundred and sixteen participants were included: 100 participants with migraine (93 participants with chronic migraine; seven participants with episodic migraine) and 16 participants with CH (nine participants with chronic CH; seven participants with episodic CH). Eighty-six percent (86%) of the participants with migraine are females and 14% males with a mean age of 44 (SD 11) (females n=86/100; males n=14/100). Nineteen percent (19%) of participants with CH were females and 81% males with a mean age of 48 (SD 14) (females n=3/16; males n=13/16) ().
Table 2 Demographics of the study population
Two-thirds of the participants with CH (n=11/16; 69%) and half of the participants with migraine (n=52/100; 52%) chose image 1 as being the most representative for their headache attacks ( and and ). Image 2 or image 3 are representative for the attacks of 41% (n=41/100) participants with migraine (and 25% participants with CH; n=4/16). Image 4 was chosen by 4% (n=4/100) of participants with migraine and 6% (n=1/16) of participants with CH. Image 5 and 6 are representative for the attacks of 3% (n=3/100) of participants with migraine whilst no participants with CH have chosen these two images.
Figure 4 Image selection by participants with cluster headache.
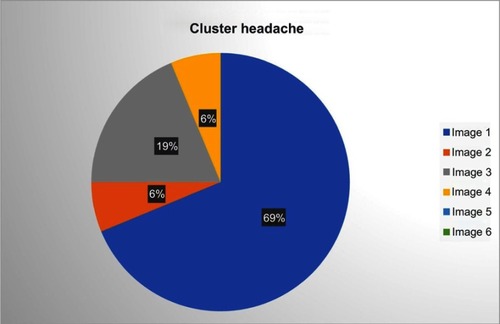
Figure 5 Image selection by participants with migraine.
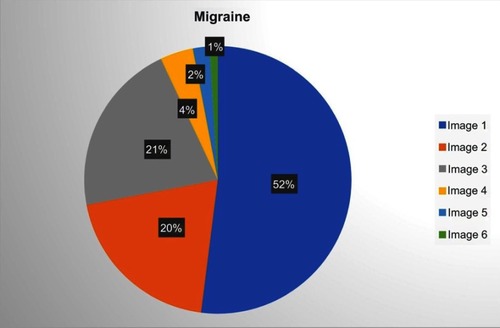
Table 3 Image selection classified by diagnosis
Discussion
Healthy participants determined that the six images in the new screening tool portray a range of pain severities from mild to excruciating. Our findings indicate that two-thirds of the participants with CH chose image 1, rated as excruciating by healthy participants to represent their attacks. This could imply that participants with CH regard their pain as “excruciating”, which is consistent with the current literature.Citation4,Citation27 According to the International Classification of Headache Disorders, migraine is described as moderate/severe pain whereas CH as severe/very severe painCitation2 of excruciating quality.Citation4 Furthermore, the intensity of pain is regarded as a key feature in differentiating CH from migraine.Citation2 CH is described by female sufferers as worse than childbirthCitation4 or as the worst pain one can expeerince.Citation13 Half of the participants with migraine in this study (52%) chose image 1 as representing their attacks. This could indicate that the pain perceived by half of the migraine participants could be interpreted as “excruciating”. However, this was suggested from the image chosen, which was rated by healthy participants. A previous survey study reported on the presence of “excruciating pain” in CH and other primary headaches.Citation28 The “excruciating pain” had a low specificity (34%) in detecting CH which suggests that the participants with non-CH in this study (migraine and tension type headache) chose “excruciating pain” to describe their attacks.Citation28 However, the question addressed to patients “Is the pain severe and/or unbearable?” was interpreted by the authors as “excruciating pain”.Citation28
Image 5 was rated in the same way as image 1 by healthy participants although none of the participants with CH have chosen this image to describe their attacks. Image 5 not rated by 20% of the healthy participants. Although the reason was not captured, we could speculate that the level of pain depicted by image 5 is not clear to both healthy participants and participants with CH. Although migraine is described as moderate/severe pain in the literature,Citation2 4% of participants with migraine chose image 4 rated as moderate by healthy participants. None of the six images in this study were able to differentiate between CH and migraine.
Strengths and limitations
This is the first study to explore the use of visual aids to assess and facilitate the diagnosis of primary headaches. The main limitation is that the ratio between participants with CH versus those with migraine (16 vs 100). However, this ratio reflects the prevalence of migraine (12%)Citation29 versus CH (0.1%).Citation5 Although the images in this study did not differentiate between CH and migraine, the study did indicate the potential of using visual aids to depict headache severity.
Future directions
The aim of future research is to establish whether the findings of this study will be replicated in a larger study with a bigger population which is currently being undertaken.Citation30 The study is testing a screening tool for CH which includes images depicting pain, verbal descriptors of pain and key questions able to differentiate between CH and migraine.Citation30 A comparison of the characteristics of these two conditions will be performed, aiming to establish the clinical features that best differentiate between the two. Future studies could explore whether images depicting headache pain could be a useful diagnostic aid in patients with language barriers.
Conclusion
Healthy participants rated the six drawings in a new screening tool as showing a rage of pain severities from mild to excruciating. Although both CH and migraine participants chose similar images to describe their headache attacks, the study indicated the potential of using images to depict headache severity.
Acknowledgment
We would like to thank Claudio Geraci for his work on the ARTe Cluster Project which inspired the research team to explore the potential of using images in screening for primary headaches.
Disclosure
FA served as an advisory board member and received honoraria from Allergan, Novartis, TEVA, Electrocore and Eneura, which he donated to charitable organisations (Migraine Trust, BASH and ADMA). The other authors report no conflicts of interest in this work.
References
- Saylor D, Steiner TJ. The global burden of headache. Semin Neurol. 2018;38(2):182–190. doi:10.1055/s-0038-164694629791944
- ICHD-3. Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211. doi:10.1177/0333102417738202
- Robbins MS. The psychiatric comorbidities of cluster headache. Curr Pain Headache Rep. 2013;17(2):313. doi:10.1007/s11916-012-0313-823296640
- May A, Schwedt TJ, Magis D, Pozo-Rosich P, Evers S, Wang S-J. Cluster headache. Nat Rev Dis Primers. 2018;4:18006. doi:10.1038/nrdp.2018.629493566
- Wei DY-T, Yuan Ong JJ, Goadsby PJ. Cluster headache: epidemiology, pathophysiology, clinical features, and diagnosis. Ann Indian Acad Neurol. 2018;21(Suppl 1):3–8. doi:10.4103/aian.AIAN_349_1729720791
- Leray E, Moreau T, Fromont A, Edan G. Epidemiology of multiple sclerosis. Rev Neurol (Paris). 2016;172(1):3–13. doi:10.1016/j.neurol.2015.10.00626718593
- Elbaz A, Carcaillon L, Kab S, Moisan F. Epidemiology of Parkinson’s disease. Rev Neurol (Paris). 2016;172(1):14–26. doi:10.1016/j.neurol.2015.09.01226718594
- Buture A, Ahmed F, Dikomitis L, Boland JW. Systematic literature review on the delays in the diagnosis and misdiagnosis of cluster headache. Neurol Sci. 2019;40(1):25–39. doi:10.1007/s10072-018-3598-530306398
- Van Alboom E, Louis P, Van Zandijcke M, Crevits L, Vakaet A, Paemeleire K. Diagnostic and therapeutic trajectory of cluster headache patients in Flanders. Acta Neurol Belg. 2009;109(1):10–17.19402567
- Sanchez Del Rio M, Leira R, Pozo-Rosich P, Laínez JM, Alvarez R, Pascual J. Errors in recognition and management are still frequent in patients with cluster headache. Eur Neurol. 2014;72(3–4):209–212. doi:10.1159/00036251725227490
- Gupta R, Bhatia MS. Comparison of clinical characteristics of migraine and tension type headache. Indian J Psychiatry. 2011;53(2):134–139. doi:10.4103/0019-5545.8253821772645
- Kim BK, Chung YK, Kim J-M, Lee K-S, Chu MK. Prevalence, clinical characteristics and disability of migraine and probable migraine: a nationwide population-based survey in Korea. Cephalalgia. 2013;33(13):1106–1116. doi:10.1177/033310241348499023615490
- Bahra A, May A, Goadsby PJ. Cluster headache: a prospective clinical study with diagnostic implications. Neurology. 2002;58(3):354–361. doi:10.1212/wnl.58.3.35411839832
- Gooriah R, Buture A, Ahmed F. Evidence-based treatments for cluster headache. Ther Clin Risk Manag. 2015;11:1687–1696. doi:10.2147/TCRM.S9419326635477
- Schurks M, Kurth T, de Jesus J, Jonjic M, Rosskopf D, Diener H-C. Cluster headache: clinical presentation, lifestyle features, and medical treatment. Headache. 2006;46(8):1246–1254. doi:10.1111/j.1526-4610.2006.00534.x16942468
- Sun-Edelstein C, Rapoport AM. Update on the Pharmacological Treatment of Chronic Migraine. Curr Pain Headache Rep. 2016;20(1):6. doi:10.1007/s11916-015-0533-926728188
- Stafstrom CE, Rostasy K, Minster A. The usefulness of children’s drawings in the diagnosis of headache. Pediatrics. 2002;109(3):460–472. doi:10.1542/peds.109.3.46011875142
- Padfield D, Omand H, Semino E, de C Williams AC, Zakrzewska JM. Images as catalysts for meaning-making in medical pain encounters: a multidisciplinary analysis. Med Humanit. 2018;44:74–81. doi:10.1136/medhum-2017-01141529895594
- Padfield D, Janmohamed F, Zakrzewska JM, Pither C, Hurwitz B. A slippery surface … can photographic images of pain improve communication in pain consultations? Int J Surg. 2010;8(2):144–150. doi:10.1016/j.ijsu.2009.11.01420064481
- Ashton-James CE, Dekker PH, Addai-Davis J, et al. Can images of pain enhance patient–clinician rapport in pain consultations? Br J Pain. 2017;11(3):144–152. doi:10.1177/204946371771712528785410
- Buture A, Boland JW, Dikomitis L, Ahmed F. Update on the pathophysiology of cluster headache: imaging and neuropeptide studies. J Pain Res. 2019;12:269–281. doi:10.2147/JPR.S17531230655693
- Khan I, Ahmed F. Visual images can prove to be an import tool to aid in the diagnosis of cluster headache. J Headache Pain. 2014;15(Suppl1:I1–I1. doi:10.1186/1129-2377-15-S1-I1
- Rossi P, Geraci C, Navarro FM. ARTe Cluster project. Cluster Headache Pain Inspiration. 2014;15(Suppl 1):C55.
- Al. Ce.Cluster. Available from: http://alcecluster.cefalea.it/. Accessed 227, 2019
- Bekhtereva V, Müller MM. Bringing color to emotion: the influence of color on attentional bias to briefly presented emotional images. Cogn Affect Behav Neurosci. 2017;17:1028–1047. doi:10.3758/s13415-017-0530-z28699142
- ICHD3beta. The international classification of headache disorders: 3rd edition (beta version). Cephalalgia. 2013;33(9):629–808. doi:10.1177/033310241348565823771276
- Lambru G, Matharu MS. Trigeminal autonomic cephalalgias: a review of recent diagnostic, therapeutic and pathophysiological developments. Ann Indian Acad Neurol. 2012;15(Suppl 1):51–61. doi:10.4103/0972-2327.10000722412275
- Torelli P, Beghi E, Manzoni GC. Validation of a questionnaire for the detection of cluster headache. Headache. 2005;45(6):644–652. doi:10.1111/j.1526-4610.2005.05131.x15953296
- Yeh WZ, Blizzard L, Taylor BV. What is the actual prevalence of migraine? Brain Behav. 2018;8(6):e00950. doi:10.1002/brb3.2018.8.issue-630106228
- Buture A, Dikomitis L, Boland JW, Ahmed F. Images depicting pain-a screening tool for cluster headache. Cephalalgia. 2018;38(1S):114.