
Abstract
Introduction
Using data from Malawi Demographic and Health Survey (2015–16), in the present study, we aimed to assess the role of exposure to family planning information through various mass media on the utilization of maternal healthcare services.
Methods
The sample population included 13,217 women aged 15–49 years with a history of at least one childbirth. Outcome measures included essential maternal healthcare services such as early and adequate use of antenatal care, skilled delivery service. Multivariate logistic regression models were used to find the association between maternal healthcare services and exposure to family planning messages by controlling for sociodemographic characteristics.
Results
Women who reported receiving family planning message through internet [odds ratio=1.48, 95% CI=1.15, 1.91], radio [odds ratio=1.15, 95% CI=1.05, 1.26], TV [odds ratio=1.53, 95% CI=1.32, 1.76] and mobile phone [odds ratio=1.23, 95% CI=1.02, 1.48] had higher odds of having timely ANC care. For using adequate number of ANC, the associations were significant for TV [odds ratio=1.41, 1.23, 1.62] and mobile phone [odds ratio=1.20, 95% CI=1.01, 1.43] only. For the use of facility delivery, a strong association was observed for poster [odds ratio=1.43, 95% CI=1.12, 1.82] and TV [odds ratio=2.99, 95% CI=1.78, 5.03]. The odds of using all three services varied noticeably between urban and rural areas, eg, receiving family planning messages through internet increased the odds of antenatal care and facility delivery services in the urban areas only, whereas that from poster was associated only for facility delivery and only in the rural areas.
Conclusion
The findings indicate a positive association on media communication regarding family planning on the uptake of maternal healthcare services.
Background
Maternal mortality refers to
the death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the duration and the site of the pregnancy, from any cause related to or aggravated by the pregnancy or its management but not from accidental or incidental causes.Citation1
Figure 1 Percentage of women receiving family planning text messages. As shown in , radio (42.8%) was the most commonly cited source of family planning messages followed by drama (31.8%) and poster (27%).
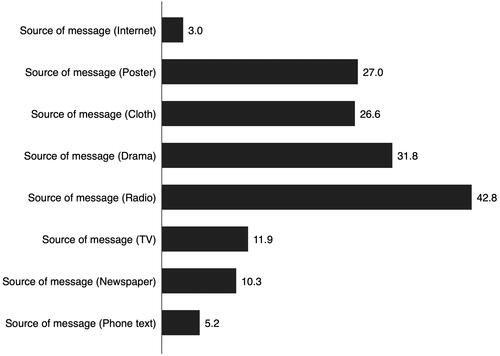
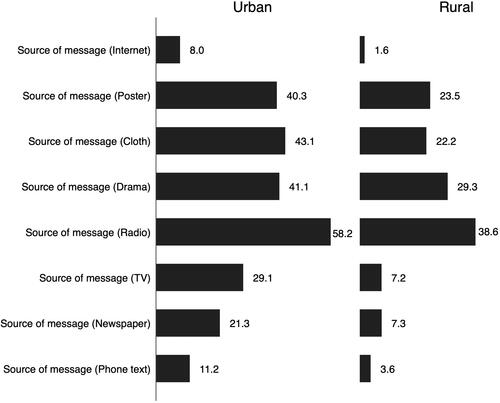
Figure 2 Urban rural difference in the percentage of women receiving family planning text messages. Its shows the urban rural difference in receiving family planning messages by the types of sources. It was evident that the percentages were noticeably higher in urban for all types of sources with the largest difference being reported for internet (8% in urban vs 1.6% in rural).
Malawi has one of the highest maternal mortality rates globally, with about 439 maternal deaths per 100,000 live birthsCitation2 compared with 16 deaths per 100 000 live births in the European region.Citation3 Malawi is also one of the poorest countries in the region and underperform in the key human development indicators. Despite that, the country has been able to improve its emergency and obstetric care infrastructure through the establishment of primary or community healthcare systems as well as maternity units and health centres across urban and rural areas. A range of government, non-profit and private providers are involved in family planning and other reproductive health services; however, only government institutions provide the services without any charge.Citation4 However, existing resources are not enough for the reproductive healthcare needs of the population; only 65% of these facilities provide prenatal services and there are only 0.2 doctors and 3.4 nurses and midwives 10,000 people in the country.Citation4 The effect of inadequate healthcare infrastructure gets aggregated by low health literacy, lack of awareness, cultural beliefs and perceived need for pregnancy care.Citation5 Even when service is available, one’s perception of pregnancy and healthcare needs can act as a barrier to availing the existing services. For instance, a qualitative research reported that the belief and practice regarding disclosure of pregnancy status prohibit women from seeking prenatal care on timely basis.Citation5
Reproductive healthcare-seeking as a behaviour can be characterised as an outcome of people’s sociocultural background as well as self-efficacy and belief systems.Citation6–Citation9 Behavioral modification is a challenging task in terms of healthcare; however, a large number of studies have been carried out regarding the ways to improve health literacy encourage healthcare seeking.Citation10–Citation12 In the field of maternal healthcare, knowledge sharing and awareness building through various community programs have also produced positive results.Citation9,Citation13 Health communication through various traditional and electronic media function as strong information and awareness building tool that enable communities shape their health beliefs and perceptions, correct the practices based on unscientific backgrounds. Women who are able to receive family-planning-related information through social media are expected to be able to make better health decisions by informing about the risk factors, preventive actions, availability of professional services.Citation10,Citation14–Citation17 However, currently there are no empirical studies on the relation between exposure to such media communication in the context of maternal healthcare seeking in Malawi. To fill this research gap, this present study was undertaken using national population data from Malawi Demographic and Health Survey of 2015–16. The main objectives were to explore the prevalence of adequate ANC attendance according to the guidelines by World Health Organization, and to investigate whether women’s exposure to mass media had any beneficial role in the utilisation of ANC and skilled childbirth services.
Methods
Data Source
This study is based on open access data from the Malawi Demographic and Health Survey (MDHS) that was conducted in 2015–16. Detailed procedures used in this study have been described in detail elsewhere.Citation18 In brief, the MDHS is a cross-sectional study and designed to yield a nationally representative sample using a two-stage sampling design. The first stage selected 850 clusters, also known as standard enumeration areas (SEAs), proportional to the population. The second stage involved the selection of a total of 27,531 households from the SEAs with an equal probability systematic selection. The MDHS collected data using face-to-face interviews from women of reproductive age (15–49 years) who had children <5 y of age. The survey was designed to collect information on population health measures, including sociodemographic, environmental, anthropometry, immunization and child health care indicators. In the interviewed households, 24,562 of the 25,146 eligible women were interviewed, representing a 98% response rate.
Inclusion Criteria
All participants for whom data on the maternal healthcare services (MHS) utilisation were available.
Outcome Variables
The outcome variables included: 1) timing of antenatal care (“within first trimester=Timely”, and “first trimester=Late”),Citation19 2) adequate utilization of antenatal care (“Inadequate=0–3 visits” and “adequate=4+visits”),Citation19 and 3) use of skilled/professional childbirth services (delivered at health facility vs delivered at home “Non-use of professional services”).Citation20
Explanatory Variables
Main explanatory variables were exposure to family planning information by mass media (Radio, Television, Newspaper) and contact with health facilities/workers ( and ). These were measured by asking the respondents whether or not they have encountered any FP-related information on Radio, TV, Newspaper; whether or not they were visited by a FP worker.Citation14,Citation15 We also considered the respondent’s health facility visit during last 12 months a possible source of family planning/maternal health communication based on the ground that the visit is most likely to involve a consultation about gestational health.
Control Variables
Besides the main explanatory variables, there following factors were likely to be correlated with ANC and facility delivery service utilisation: Age groups (15–24/25–29/30–34/35–49), Residency (rural/urban), Religion (Christian/Other), Education (Nil/Primary/Secondary/Higher), Wealth index (Poorest, Poorer, Middle, Richer, Richest), Occupation (Unemployed/Blue Collar/White Collar), Parity (1–2/3–4/>4).Citation21,Citation22
Statistical Analysis
Data were analysed using Stata version 16.1. At first, we applied svy command to adjust for the clustered nature of the survey. The proportion of the outcome variables (ANC timing, ANC frequency and Place of delivery) across the mass media exposure and the sociodemographic variables were described by percentages with 95% CIs. Following that, the association between the media use variables with the three outcomes were measured using binary logistic regression while controlling for the potentially confounding variables. Three separate regression models were run for each of the outcome variables (overall sample, urban sample, and rural sample). This stratification was guided by previous evidence on the significant urban-rural difference in healthcare use. Model fitness was verified by the Hosmer-Lemeshow goodness-of-fit test. Hosmer–Lemeshow goodness-of-fit statistic was conducted and the values ranged from 0.7 to 1.2 (p > 0.05), which indicated good model fit. Multicollinearity tests were conducted using the VIF command in Stata following each of the regression models. There was no indication of multicollinearity in any of the models (VIF<5). All tests were two-tailed and were considered significant at 5%.
Results
Basic sociodemographic characteristics of the sample population was supplied in the Appendix. presents the percentage of sample population according to the use of ANC and professional delivery services. The prevalence of timely ANC visit was 24.41% [95% CI=23.28, 25.58] and that of having at least four ANC visits was 50.96% [95% CI=49.65, 52.27]. A large percentage of women reported delivering at a health facility 93.70% [95% CI=92.80, 94.49] (not shown in the table). In general, the percentage of women who reported timely and adequate use of ANC and facility delivery was higher among those aged between 20 to 34 years, followers of Christianity, had primary level education, rural resident, from households with higher wealth quintile, employed in blue-collar jobs, and had 1–2 children.
Table 1 Prevalence of Maternal Healthcare Use by Sociodemographic Variables (N=13,217)
The percentages of sample population according to the use of ANC and professional delivery services by media use status are shown in . A larger percent of women who used all three types of maternal healthcare services were in the group who did not receive any family-planning-related message through the media channels. The table also shows that the percentage of using the maternal healthcare services were relatively higher among those who had exposure to family planning messages through these channels. For instance, among those who reported receiving family planning through internet, the percentage of having timely (1.94% vs 3.73%) and adequate use of ANC (1.75% vs 3.02%) and facility delivery (0.44% vs 2.53%) were relatively higher.
Table 2 Prevalence of Maternal Healthcare Use by Sources of FP Message
The results of regression analyses are presented in . Women who reported receiving family planning message through internet [Odds ratio=1.48, 95% CI=1.15, 1.91], radio [Odds ratio=1.15, 95% CI=1.05, 1.26], TV [Odds ratio=1.53, 95% CI=1.32, 1.76] and mobile phone [Odds ratio=1.23, 95% CI=1.02, 1.48] had higher odds of having timely ANC care. For using adequate number of ANC, the associations were significant for TV [Odds ratio=1.41, 1.23, 1.62] and mobile phone [Odds ratio=1.20, 95% CI=1.01, 1.43] only. For the use of facility delivery, a strong association was observed for poster [Odds ratio=1.43, 95% CI=1.12, 1.82] and TV [Odds ratio=2.99, 95% CI=1.78, 5.03]. The odds of using all three services varied noticeably between urban and rural areas. For instance, receiving family planning message through internet increased the odds of ANC and facility delivery services in the urban areas only, whereas that from poster was associated only for facility delivery and only in the rural areas.
Table 3 Association Between of Maternal Healthcare Use by Media Use Variables
Discussion
Based on data from Malawi Demographic and Health Survey, the present study aimed to explore whether or not mass media communication on family planning has any positive association with the utilisation of ANC and facility delivery services. Overall, the findings showed a beneficial effect of exposure to media communication on the uptake of these services, implying the fact that increasing mass media communication can be an effective channel for improving maternal healthcare service uptake. This finding is in line with those from a community-based study in Nepal. The study reported that mass media exposure had a positive influence on the utilisation of antenatal care services in Nepal.Citation23 A more recent study in rural Malawi reported that women who had exposure to community-led mass media campaigns were more likely to access maternal health care services than those with no exposure.Citation16 However, previous studies were limited in scope, both in terms of national population coverage and the number of different types of media channels.
The present study reaffirms the past findings regarding the positive effect of mass media communication, and advances the field of research by showing the comparative effective of a range of media channels. Health researchers and policymakers are increasingly interested in internet technology-based solutions to the long-standing challenges faced by the public health system.Citation24,Citation25 Leveraging the beneficial role of media communication, countries with higher maternal mortality rates such as Malawi may be able to accelerate the progress towards the health-related Sustainable Development Goals.Citation26–Citation28
In addition to the findings regarding the beneficial influence of mass media exposure about family planning on the uptake of maternal healthcare services, our findings also revealed a significant regional difference in the association among urban and rural areas. Firstly, despite a larger proportion of the sample population being from rural areas, the percentage of women who reported exposure to such messages was higher for all eight types of media, with the largest difference being observed for internet. This finding is rather predictable given the lower penetration of modern technologies and media channels in the rural areas. This was true even for the traditional media including radio and TV as a higher percentage of women in the urban areas reported receiving family planning messages through these channels. Apart from this, variation was observed in the strength of the associations as well. For instance, receiving family planning messages through the internet showed increased odds ANC and facility delivery services in the urban areas only. In contrast, receiving messages from posters was positively associated only with facility delivery and only in the rural areas. Regional disparity in healthcare-related indicators is a common issue and is a major concern especially for critical areas such as maternal and child health.Citation7,Citation29,Citation30 Based on our findings, it is suggestible that health promotion programs pay special attention to addressing the regional gap to ensure equitable exposure to health communication channels which might prove beneficial to service uptake rates.
Maternal mortality to a great extent reflects women’s access to and utilisation of quality healthcare. While socioeconomic status has the recognition of being a dominant determinant of health service uptake, the role of other major driving factors such as individual perception and understanding of the healthcare needs during pregnancy and the motivation to access or seek care is absolutely crucial. In most cases, especially among primigravid women who are more likely to lack the experience and knowledge of the danger signs and complications associated with pregnancy, and the health risks of delivering without a skilled professional; health communication programs through community health workers and mass media can serve as a key strategy to promote awareness and uptake of essential maternal health services, eg, ANC and delivery care.Citation15,Citation31 Regular exposure to reinforcing information can encourage interpersonal discussion and collective social learning that can spur consequent changes in values and healthcare-seeking behaviour.Citation17,Citation26 Finally, the positive association between media exposure of FP related message on the use of ANC and skilled childbirth services warrant for a more context-specific approach to promote the use of these services. Arguably, if the information communicated through the media were on timely initiation and adequate ANC use and skilled care at birth, the effect would have been more pronounced. Or else, had the outcome studied were family planning utilization, more strong association would have been detected.
As far as we are concerned, this is the first study to demonstrate the relationship between family planning exposure on mass media and maternal healthcare service utilization in Malawi. The sample was large and nationally representative, and thereby making the results generalizable to the entire women population of the same age group. This is also the first study in this area to include eight different types of media channels as a source of family planning messages. These findings provide important insight for policy analysts and future researchers. Apart from the strengths, there are several limitations to report as well. Firstly, the data were cross-sectional and therefore the associations cannot indicate causation. Secondly, there was no concrete information on the exact content of the messages and at what frequency were they received/seen. It is possible that the effectiveness of a certain type of media depends on the efficacy of the content. Women with limited educational qualifications are less likely to have exposure to more modern technologies such as internet. As such, the effectiveness of certain types of media is dependent on the capacity of the population to process the information. So we were unable to shed light on this, More in-depth studies should be carried out to assess the relative ease of use and efficacy of different media channels. We were unable to control for these factors due to lack of adequate data. Lastly, the variables were reported subjectively and are susceptible to reporting/recall bias.
Conclusion
In conclusion, our findings suggest a beneficial role of communication through mass media on maternal healthcare utilisation in Malawi. Based on these findings, it is recommendable that maternal health programs in Malawi emphasize developing more innovative approaches to incorporate mass media exposure for delivering maternal health-related information to the communities. Special strategies are required to improve the coverage of the media communicable by reducing the regional gaps. Ours is the first study to include eight different types of media channels as a source of family planning messages; however, there was no data on the content of the media which could help to better understand the relative efficacy of these channels. Further studies are therefore necessary to focus on the effectiveness of media communication and maternal healthcare seeking by including more diverse range of mass media. The findings indicate a positive association on media communication regarding family planning on the uptake of maternal healthcare services. Critical health-related knowledge and information can empower women and help make more informed decision to prevent pregnancy complications and adverse childbirth outcomes. Healthcare programs in Malawi should invest in increasing awareness among women through mass media and making reproductive health information more accessible regardless of socioeconomic and geographic barriers.
Abbreviations
ANC, Antenatal care; LMICs, Low-and-middle-income countries; MMR, Maternal mortality rates; SDG, Sustainable Development Goals.
Data Sharing Statement
All data are available through the DHS website.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Patwardhan M, Eckert LO, Spiegel H, et al. Maternal death: case definition and guidelines for data collection, analysis, and presentation of immunization safety data. Vaccine. 2016;34:6077–6083. doi:10.1016/j.vaccine.2016.03.042
- Maternal, neonatal, and child health. Malawi: U.S. Agency for International Development; 2019. Available from: https://www.usaid.gov/malawi/global-health/maternal-neonatal-and-child-health. Accessed August 19, 2020.
- Data and statistics. Available from: https://www.euro.who.int/en/health-topics/Life-stages/maternal-and-newborn-health/data-and-statistics. Accessed August 19, 2020.
- Mchenga M, Burger R, von Fintel D. Examining the impact of WHO’s Focused Antenatal Care policy on early access, underutilisation and quality of antenatal care services in Malawi: a retrospective study. BMC Health Serv Res. 2019;19:295. doi:10.1186/s12913-019-4130-1
- Roberts J, Marshak HH, Sealy D-A, Manda‐Taylor L, Mataya R, Gleason P. The role of cultural beliefs in accessing antenatal care in Malawi: a qualitative study. Public Health Nurs. 2017;34:42–49. doi:10.1111/phn.12242
- Abubeker FA, Fanta MB, Dalton VK. Unmet need for contraception among HIV-positive women attending HIV care and treatment service at Saint Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia. Int J Reprod Med. 2019;2019:1–7. doi:10.1155/2019/3276780
- Achyut P, Mishra A, Montana L, Sengupta R, Calhoun LM, Nanda P. Integration of family planning with maternal health services: an opportunity to increase postpartum modern contraceptive use in urban Uttar Pradesh, India. J Fam Plann Reprod Health Care. 2016;42:107–115. doi:10.1136/jfprhc-2015-101271
- Akeju DO, Oladapo OT, Vidler M, et al. Determinants of health care seeking behaviour during pregnancy in Ogun State, Nigeria. Reprod Health. 2016;13(Suppl 1). doi:10.1186/s12978-016-0139-7
- Asefa A, Beyene H. Awareness and knowledge on timing of mother-to-child transmission of HIV among antenatal care attending women in Southern Ethiopia: a cross sectional study. Reprod Health. 2013;10:66. doi:10.1186/1742-4755-10-66
- Bergsma LJ, Carney ME. Effectiveness of health-promoting media literacy education: a systematic review. Health Educ Res. 2008;23:522–542. doi:10.1093/her/cym084
- Gele AA, Pettersen KS, Torheim LE, Kumar B. Health literacy: the missing link in improving the health of Somali immigrant women in Oslo. BMC Public Health. 2016;16. doi:10.1186/s12889-016-3790-6
- Ishikawa H, Kiuchi T. Health literacy and health communication. Biopsychosoc Med. 2010;4:18. doi:10.1186/1751-0759-4-18
- Ramoshaba R, Sithole SL. Knowledge and awareness of MTCT and PMTCT post-natal follow-up services among HIV infected mothers in the Mankweng Region, South Africa. Open AIDS J. 2017;11:36–44. doi:10.2174/1874613601711010036
- Ajaero CK, Odimegwu C, Ajaero ID, Nwachukwu CA. Access to mass media messages, and use of family planning in Nigeria: a spatio-demographic analysis from the 2013 DHS. BMC Public Health. 2016;16:16. doi:10.1186/s12889-016-2979-z
- Asp G, Pettersson KO, Sandberg J, Kabakyenga J, Agardh A. Associations between mass media exposure and birth preparedness among women in southwestern Uganda: a community-based survey. Glob Health Action. 2014;7(1):22904. doi:10.3402/gha.v7.22904
- Zamawe COF, Banda M, Dube AN. The impact of a community driven mass media campaign on the utilisation of maternal health care services in rural Malawi. BMC Pregnancy Childbirth. 2016;16:21. doi:10.1186/s12884-016-0816-0
- Wakefield MA, Loken B, Hornik RC. Use of mass media campaigns to change health behaviour. Lancet. 2010;376(9748):1261–1271. doi:10.1016/S0140-6736(10)60809-4
- Nkoka O, Ntenda PAM, Senghore T, Bass P. Maternal overweight and obesity and the risk of caesarean birth in Malawi. Reprod Health. 2019;16. doi:10.1186/s12978-019-0700-2
- Yaya S, Bishwajit G, Ekholuenetale M, Shah V, Kadio B, Udenigwe O. Timing and adequate attendance of antenatal care visits among women in Ethiopia. PLoS One. 2017;12:e0184934. doi:10.1371/journal.pone.0184934
- The impact of healthcare insurance on the utilisation of facility-based delivery for childbirth in the Philippines. Available from: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0167268. Accessed February 17, 2019.
- Ghose B, Feng D, Tang S, et al. Women’s decision-making autonomy and utilisation of maternal healthcare services: results from the Bangladesh Demographic and Health Survey. BMJ Open. 2017;7(9):e017142. doi:10.1136/bmjopen-2017-017142
- Benova L, Campbell OM, Sholkamy H, Ploubidis GB. Socioeconomic factors associated with maternal health-seeking behaviours among women from poor households in rural Egypt. Int J Equity Health. 2014;13:13. doi:10.1186/s12939-014-0111-5
- Acharya D, Khanal V, Singh JK, Adhikari M, Gautam S. Impact of mass media on the utilization of antenatal care services among women of rural community in Nepal. BMC Res Notes. 2015;8(1). doi:10.1186/s13104-015-1312-8
- Anderson-Lewis C, Darville G, Mercado RE, Howell S, Di Maggio S. mHealth technology use and implications in historically underserved and minority populations in the United States: systematic literature review. JMIR MHealth UHealth. 2018;6(6):e128. doi:10.2196/mhealth.8383
- Destigter K. mHealth and developing countries: a successful obstetric care model in Uganda. Biomed Instrum Technol. 2012;Suppl:41–44. doi:10.2345/0899-8205-46.s2.41
- Hornik R, McAnany E. Theories and evidence: mass media effects and fertility change. Commun Theory. 2001;11:454–471. doi:10.1111/j.1468-2885.2001.tb00253.x
- Konkor I, Sano Y, Antabe R, Kansanga M, Luginaah I. Exposure to mass media family planning messages among post-delivery women in Nigeria: testing the structural influence model of health communication. Eur J Contracept Reprod Health Care. 2019:1–6.
- Moorhead SA, Hazlett DE, Harrison L, Carroll JK, Irwin A, Hoving C. A new dimension of health care: systematic review of the uses, benefits, and limitations of social media for health communication. J Med Internet Res. 2013;15:e85. doi:10.2196/jmir.1933
- Bishwajit G, Kpoghomou M-A. Urban-rural differentials in the uptake of mammography and cervical cancer screening in Kenya. J Cancer Policy. 2017;12:43–48. doi:10.1016/j.jcpo.2017.03.005
- le Booysen FR. Urban–rural inequalities in health care delivery in South Africa. Dev South Afr. 2003;20:659–673. doi:10.1080/0376835032000149298
- Schiavo R. The importance of community-based communication for health and social change. J Commun Healthc. 2016;9:1–3. doi:10.1080/17538068.2016.1154755