
Abstract
Objective
Previous evidence has recommended conservative interventions as the best treatment in individuals with chronic low back pain (CLBP). However, the influence of psychosocial factors on the treatment outcomes is unclear. Therefore, this systematic review aimed to address the psychosocial factors that influence changes in pain and disability in patients with CLBP after a guideline-based conservative intervention.
Methods
Four electronic databases were systematically searched from inception until September 2020 for prospective studies examining the relationship between psychosocial factors and the outcomes of pain and disability after conservative intervention. All included studies were selected, extracted, and critically evaluated by two independent reviewers.
Results
In total, 15 studies were included in this systematic review. The results support the link between the baseline fear of movement, depression, self-efficacy, and catastrophizing with future functional disability outcomes after conservative interventions. However, these factors were less likely to predict changes in pain intensity outcomes after conservative interventions. Self-efficacy seems to mediate between some of the baseline psychosocial factors (eg, fear) and future pain and disability.
Conclusion
Fear of movement, self-efficacy, catastrophizing and depression were consistently reported to predict disability outcomes irrespective of the type of conservative intervention. This highlights the importance of addressing these factors in conservative management of CLBP.
Background
Lower back pain (LBP) is a common health condition and one of the leading causes of disability worldwide.Citation1 The prevalence of LBP has recently increased in the general population with varying outcome degrees, ranging from spontaneous recovery to progression to the chronic stage.Citation1–Citation3 Previous research has found that 10–40% of individuals suffering from LBP develop chronic symptoms and suffer some form of disability.Citation4
It is important to note that psychosocial factors contribute significantly to pain persistence, response to conservative treatment and rehabilitation, and the likelihood of developing disability.Citation5–Citation9 For example, self-efficacy belief has been identified as a mediator in the relationship between depressive symptoms and affective pain intensity,Citation10 in which individuals with higher self-efficacy were significantly more tolerant of pain and capable of performing daily-life activities.Citation10 Further, individuals who have a higher level of catastrophizing may perceive and report a higher pain level.Citation7 Thus, several studies have analyzed the potential link between psychosocial factors such as catastrophizing and fear avoidance and response to treatment in patients with chronic low back pain (CLBP).Citation2,Citation5,Citation7,Citation8,Citation11,Citation12
Many previous systematic reviews have presented the relationship between disability and psychosocial factors in patients with LBP.Citation12 These reviews investigated topics related to catastrophizing thoughts and disability,Citation13,Citation14 depression association with disability,Citation13,Citation15–Citation17 the predictive value of self-efficacy on changes in disability,Citation13,Citation18 functional coping mechanisms,Citation19 and fear-avoidance beliefs as examined extensively in several different publications.Citation12–Citation15,Citation20 For the most part, studies on this topic are based on a prognostic study model, which attempts to examine the predictive value of these psychosocial factors on outcomes changes without considering the specific types of treatment administered.Citation21 Considering the type of treatment may improve the design of available interventions for people with low back pain and improve their clinical outcomes.Citation21
Further, most of the aforementioned studies and reviews highlight the importance of psychosocial factors as predictors of changes in disability level and the subsequent recovery from pain in mixed groups of LBP (ie, chronic and acute), as well as patients in both prospective cohorts and cross-sectional studies.Citation8 However, previous reviews have underlined that most of the included studies were not high quality, the patient population was heterogeneous, and the study design was sometimes inappropriate.Citation22 As a result, it is often impossible to draw solid and reliable conclusions from this type of review.
Although psychosocial factors to predict outcome in LBP may be similar in acute and chronic conditions,Citation23,Citation24 it is noteworthy that acute and chronic LBP have different associations with psychosocial factors.Citation23,Citation25 This suggests that some psychosocial factors might be more prognostic in LBP when considering disease duration (chronicity).
Apart from Wessels et al,Citation19 none of the reviews mentioned above have explored the psychosocial factors associated with changes in pain and disability in people with CLBP after conservative therapy. However, this review only included six studies related to this association and suggested that no conclusion could be drawn due to this limited number of studies. Although a similar systematic review was published,Citation22 it has some limitations. First, the cross-sectional studies included could not explain the change after the intervention. Secondly, limiting the search terms to only “physiotherapy” might miss multiple studies. Therefore, it is crucial to further examine the predictive ability of psychosocial factors on changes in pain and disability among individuals with CLBP. Understanding this association is vital to establish appropriate interventions targeting psychosocial factors in practice.
Aim
The aim of this study was to identify the prognostic value of psychosocial factors on the change in pain and/or disability in participants with CLBP following conservative interventions as recommended by clinical guidelines (NICE, 2016).
Methods
Protocol Registration
The systematic review protocol was registered in PROSPERO (registration number: CRD 42020131481) and conformed to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.Citation26
Eligibility Criteria
Participants
Research studies published in English and that met the following inclusion criteria were included in the review. Studies were included if participants were adults aged 18 years or over and diagnosed with CLBP. CLBP is defined as a pain between the bottom of the ribs and the buttock creases that lasts for at least three months.Citation27 Studies were excluded where participants had any identified pathoanatomical diagnosis of CLBP such as stenosis, fracture, malignancy, vertebral fracture, infections, or cardiovascular, respiratory, neurological, gastrointestinal, urogenital, or related conditions.Citation27 All studies must provide information that CLBP patients received a guideline-recommended conservative intervention either alone or as part of a multidisciplinary approach.
Study Design
Only research studies with prospective designs were included. Studies must report the psychosocial outcomes (fear, anxiety, etc.) and their correlation with pain and disability. Studies with mixed patient groups (acute and chronic) were included if a separate analysis of patients with chronic cases was reported.
Outcome Measures
Primary outcome measures of the included studies included pain, disability, and/or psychosocial outcome measures. Studies must report predictive measures like odds ratio (OR), relative risk (RR), and regression coefficient. Studies reporting only Pearson correlation coefficients were excluded.
Information Source
Two independent reviewers (AH, MA) conducted a comprehensive search using four electronic databases (PubMed, Medline, CINAHL, and PsycINFO) from inception to September 2020 to extract relevant studies. In addition, the reference lists of the extracted articles were manually searched to include any articles missed by the electronic search.
Search Strategy
Searching the electronic databases involved the following three steps, which were combined with an “AND” statement:
Studies related to CLBP populations were identified using the following keywords: Low Back Pain, Recurrent Low Back Pain, Lower Back Aches, Low Back, Back Pains, Lower Back Pain, Back Ache, Chronic Low Pains, Chronic Lower Back Pain; Low Back Ache, Back Aches, Low Back Aches, Low Backache, Backache, Low Backaches, Backaches. In combination with the “OR” statement.
The NICE guideline recommends the following non-invasive treatments for LBP: self-management, exercise, manual therapy, psychological therapy, and combined psychological and physical therapy programs. Therefore, the following words were used to identify studies with the intervention of interest: Exercise; Psychosocial Therapy, Self-management, Psychological Therapy, Manipulation; Mobilization, Soft Tissue Techniques, Cognitive Behavioral Therapy, Psychosocial Approach; Education; Multi-Disciplinary, Biopsychosocial Rehabilitation, Physiotherapy, Physical Therapy, Rehabilitation, Active Therapy. In combination with the “OR” statement.
The study included psychosocial outcomes identified using the following words: Sensitivity, Anxiety, Vigilance, Hypervigilance, Attention, Kinesiophobia, Fear, Fear Avoidance Beliefs, Beliefs, Cognitive, Depression, Coping, Pain Coping, Fear, Avoidance; Anxiety, Return to Work, Absentees; Self-Efficacy, Sick Leaves, Mediation, Predictors, Prognostic. Combined with the “OR” statement.
Study Selection
All titles and abstracts were screened independently by two reviewers (AA and MA). Studies with acute LBP or no separate data for CLBP were excluded. A third reviewer was brought in to resolve any disagreements. Finally, all excluded studies and reasons for exclusion were logged.
Extraction Procedure
Two independent reviewers (AA and MA) carried out the data extraction of all included studies. Data included: title and authors, objectives and study design, duration of study participation, description of the population from which the participants were drawn, type of intervention, inclusion and exclusion criteria, baseline pain severity, mean age, psychosocial outcome reported; and the study outcomes, conclusions, and limitations reported by the authors.
Quality and Risk of Bias Assessment
The Newcastle-Ottawa quality assessment scale for observational studies was used to examine the quality of prospective cohort studies.Citation20 The scale consists of eight questions covering three domains: selection, comparability, and outcome assessment. A higher score indicates good quality, and the overall rating is based on the scores good, fair, and poor quality. This scale was chosen as it is simple to use and has been validated in case-control and prospective investigations. Inter-rater reliability was moderate to good (ICC = 0.52; CI = 0.14–0.76).Citation28
A secondary analysis of previously-published RCTs was used in five studies to find the prognostic psychosocial factors, and the quality of these studies was assessed using the Quality in Prognostic Studies (QUIPS) tool.Citation29 This tool has six domains covering study participation, attrition, prognostic factor measurement, outcome measurement, confounding, and statistical analysis and reporting.
Results
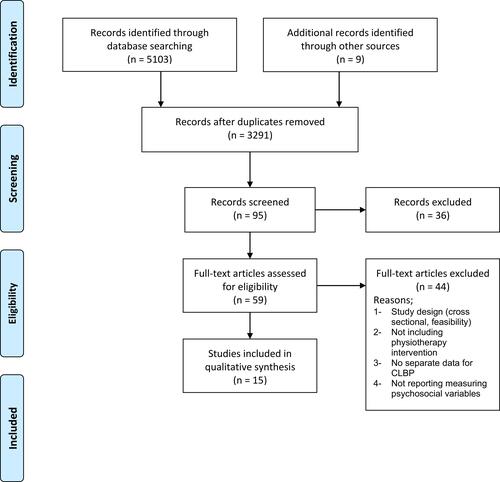
A total of 15 studies met the inclusion criteria after the full-text screening. The process using the PRISMA flowchart is shown in . The number of participants was 4496 (range, 26–1760) with a mean age of 44.1 ± 5.1 years, and a higher proportion of women (60%). The mean pain intensity measured at baseline in the reported studies was 5.1 ± 0.86. The mean dropout rate was 16%. All prospective cohort studies reported measurements before and after each intervention ().
Table 1 Characteristics of the Included Studies
Figure 1 Flowchart.
Methodological Quality and Risk of Bias
The overall quality of the prospective cohort studies was fair as per the Newcastle-Ottawa quality assessment scale, with four studies scored as good, two as fair, and four as poor quality. The QUIPS assessment tool for prognostic studies for the remaining studies showed a low risk of bias. Details of scores can be found in and .
Table 2 Quality Assessment of Cohort Studies
Table 3 Quality Assessment of Other Prognostic Studies
Synthesis of the Results
The included studies investigated different conservative interventions and used various outcome measures when reporting the association between the intervention and outcome. Therefore, proceeding with meta-analysis was not feasible. Only two studies reported a mediation relationship between disability and pain with psychosocial outcome measures, and the remaining 13 studies were concerned with the prognostic association.
Several psychosocial factors -presented below- correlated with pain and disability outcomes following conservative interventions in patients with CLBP. Additionally, Different outcome measures were used in the selected studies ().
Table 4 Summary of Reported Pain and Disability Outcomes, Type of Association and Type of Intervention in the Included Studies
Fear and Avoidance
Fear-avoidance factors were a significant predictor of disability outcomes in four studies,Citation25,Citation30–Citation32 with regression coefficient β ranging from 0.08 to 0.30. Moreover, one more study reported an OR value of 1.11.Citation33
Only one study reported baseline fear-avoidance as a predictor of pain level after treatment.Citation30 The relationship between pain-related fear with disability and pain was mediated by self-efficacy. The outcome measures used to measure fear and avoidance were the Tampa scale of kinesiophobia in three studies and the fear-avoidance belief questionnaire.
Self-Efficacy
Baseline self-efficacy was reported to predict disability outcomes in three studiesCitation10,Citation32,Citation34 with regression coefficient β ranging from 0.21 to 0.37. Further, one study reported an OR of 9.8 of self-efficacy to predict the disability outcomes.Citation35
The reduction in disability outcomes was 28.3%, mediated by a change in self-efficacy outcomes.Citation36 With regard to pain intensity, three studies reported a predictive role of low self-efficacy to high pain intensity in CLBP with regression coefficient β ranging from 0.23 to 0.56.Citation32,Citation34 Further, one study reported an OR value of 1.150.Citation37
Outcome measures used were the pain self-efficacy questionnaire, self-efficacy scale, and chronic pain self-efficacy scale.
Catastrophizing and Pain Coping
Scoring a high level of catastrophizing and pain coping outcomes was a prognostic indicator of higher disability with regression coefficient β of 0.11 and an OR of 1.5.Citation25,Citation37
The outcome measure used in these studies were, the catastrophizing pain scale for catastrophizing and coping strategies questionnaire used for pain coping.
Depression
Two studies reported a predictive relationship between depression and disability and pain. A higher depression score at baseline was a predictor of poor improvement in pain and disability, with regression coefficients β of 0.24 and 0.17, respectively.Citation10,Citation38
Each study used two different outcome measures, namely the depression symptoms checklist SCL-90 and the hospital anxiety and depression scale.
Work
Two studies reported a positive association between work outcomes and pain and disability outcomes. Work participation is a prognostic indicator for improvement in pain and disability with OR values of 1.21 and 1.34, respectively.Citation39 The number of days missed because of CLBP was reported to be predictive, with higher disability levels in one study.Citation40
STarT Back Tool
High and medium modifiable psychological risk factors were associated with a greater risk of poor recovery on the disability scale compared to the lower risk group, according to the STarT Back Tool in one study.Citation23
Discussion
This study aimed to identify the psychosocial factors that influence changes in pain and disability in patients with CLBP after guideline-based conservative intervention. The results highlight that fear-avoidance beliefs, self-efficacy, catastrophizing, pain coping, depression, days missed due to back pain, work participation, and STarT back questionnaire score could predict disability status among CLBP patients receiving conservative interventions according to average-fair quality studies. However, change in pain score was predicted by only two psychosocial factors: self-efficacy and depression according to average-poor quality studies.
This paper builds on the findings established by the systematic review of Wessels et al,Citation19 that functional coping and pain intensity are correlated with post-treatment disability level, as reported in six studies. On the one hand, Wessels et alCitation19 suggested that conclusions cannot be drawn from such a limited number of heterogeneous studies. On the other hand, in this systematic review, many psychosocial factors have been identified as being consistent predictors of change to disability level after conservative (non-surgical) interventions have been conducted.
This systematic review established that self-efficacy and fear-avoidance belief had significant weight as predictors of change in disability, following conservative interventions in people with CLBP. These findings are in line with the results published in Wertli et alCitation14 related to the moderating role of fear-avoidance in the efficacy of treatment of patients with subacute LBP and previously-reported reviews.Citation12–Citation16 Furthermore, the correlation between fear avoidance and disability level was found to be mediated by two factors in two different studies:Citation10,Citation34 self-efficacy and depression. However, it should be noted that formal mediation analysis and preferred study design were not applied to one of the studies.Citation21
The results of this systematic review also highlighted the influence of catastrophizing and depression when it comes to any change to disability score after conservative intervention was applied for participants with CLBP.
Psychosocial factors can predict poor treatment outcomes, and this is indeed a challenge for clinicians.Citation21 Psychosocial factors may play a key role in persistent symptoms, disability, and the development of chronic pain.Citation21 These types of factors can affect the patient’s reaction to the treatment they are given. This aspect of CLBP presents itself clinically in psychological comorbidities such as different forms of anxiety, depressive symptoms, and elevated somatic awareness.
The application of psychosocial based treatment showed disappointing results when studied in RCTs without classifying LBP according to psychosocial risk.Citation41 Therefore, a screening tool (STarT Back tool) was developed to stratify patients according to the risk of psychosocial factors, allowing them to be assigned the most appropriate treatment for their LBP.Citation42 The RCT results for LBP showed an improvement in disability scores and a remarkable reduction in the cost of care.Citation43 Furthermore, the STarT Back tool was predictive for the disability level of CLBP after a one-year follow-up. However, its ability to predict pain after 12 months was not nearly as effective.Citation23
The identification of statistical correlation does not necessarily mean there is any causation.Citation44,Citation45 Therefore, there is a need for mediation studies that can better explain the extent to which these psychosocial factors explain the changes noticed when it comes to pain and disability. For example, a systematic review involving 12 studies examining what mediates disability in patients with back and neck painCitation46 identified that fear, self-efficacy, and psychological distress were mediating towards the relationship between pain and disability. However, one limitation reported by the author is that more than half of the included studies were cross-sectional designs, which means that a definitive conclusion about causality might not be possible.
From the current study, identifying these factors will help further research determine which factors are effective treatment modifiers for people with CLBP undergoing conservative treatment, allowing clinicians to choose appropriate treatment strategies to improve clinical outcomes.
Limitations
The exclusion of studies not reported in English might mean that this review overlooks certain important contributions to the literature. For example, the previous review by Wessels et alCitation19 reported studies in English and German. In addition, other comorbidities and factors were not considered in the included studies and may affect the prognostic utility of the psychosocial factors for pain and disability. Finally, the variability in follow-up duration (1 to 36 months) limits the generalizability of this study.
Conclusion
This systematic review has extended the knowledge available regarding the psychosocial factors associated with pain and disability in CLBP following conservative treatments. The fact that the studies consistently found psychosocial factors, including fear of movement, self-efficacy, catastrophizing, and depression, to predict disability outcomes irrespective of the type of conservative intervention suggests the importance of addressing these factors in the screening of CLBP individuals undergoing conservative intervention treatments. More research is needed to understand to what extent these factors explain the changes in pain levels among CLBP patients.
Acknowledgment
We are immensely grateful to the Deanship of Scientific Research at Prince Sattam bin Abdulaziz University, Al-Kharj, Saudi Arabia, for their support.
Disclosure
The authors report no conflicts of interest in this work.
References
- Hoy D, Bain C, Williams G, et al. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012;64(6):2028–2037. doi:10.1002/art.34347
- Kamper SJ, Apeldoorn AT, Chiarotto A, et al. Multidisciplinary biopsychosocial rehabilitation for chronic low back pain. Cochrane Database Syst Rev. 2014. doi:10.1002/14651858.cd000963.pub3
- Jarvik JG, Deyo RA. Diagnostic evaluation of low back pain with emphasis on imaging. Ann Intern Med. 2002;137(7):586. doi:10.7326/0003-4819-137-7-200210010-00010
- Hartvigsen J, Hancock MJ, Kongsted A, et al. What low back pain is and why we need to pay attention. Lancet. 2018;391(10137):2356–2367. doi:10.1016/s0140-6736(18)30480-x
- Leeuw M, Goossens MEJB, Linton SJ, Crombez G, Boersma K, Vlaeyen JWS. The fear-avoidance model of musculoskeletal pain: current state of scientific evidence. J Behav Med. 2006;30(1):77–94. doi:10.1007/s10865-006-9085-0
- Vlaeyen JWS, Linton SJ. Fear-avoidance and its consequences in chronic musculoskeletal pain: a state of the art. Pain. 2000;85(3):317–332. doi:10.1016/s0304-3959(99)00242-0
- Crombez G, Eccleston C, Van Damme S, Vlaeyen JWS, Karoly P. Fear-avoidance model of chronic pain. Clin J Pain. 2012;28(6):475–483. doi:10.1097/ajp.0b013e3182385392
- Giusti EM, Manna C, Varallo G, et al. The predictive role of executive functions and psychological factors on chronic pain after orthopaedic surgery: a Longitudinal Cohort Study. Brain Sci. 2020;10(10):685. doi:10.3390/brainsci10100685
- Wideman TH, Asmundson GGJ, Smeets RJEM, et al. Rethinking the fear avoidance model: toward a multidimensional framework of pain-related disability. Pain. 2013;154(11):2262–2265. doi:10.1016/j.pain.2013.06.005
- Skidmore JR, Koenig AL, Dyson SJ, Kupper AE, Garner MJ, Keller CJ. Pain self-efficacy mediates the relationship between depressive symptoms and pain severity. Clin J Pain. 2015;31(2):137–144. doi:10.1097/ajp.0000000000000094
- Gheldof ELM, Crombez G, van den Bussche E, et al. Pain-related fear predicts disability, but not pain severity: a path analytic approach of the fear-avoidance model. Eur J Pain. 2010;14(8):870.e1–870.e9. doi:10.1016/j.ejpain.2010.01.003
- Pincus T, Burton AK, Vogel S, Field AP, Systematic A. Review of psychological factors as predictors of chronicity/disability in prospective cohorts of low back pain. Spine. 2002;27(5):E109–E120. doi:10.1097/00007632-200203010-00017
- Geisser ME, Robinson ME, Keefe FJ, Weiner ML. Catastrophizing, depression and the sensory, affective and evaluative aspects of chronic pain. Pain. 1994;59(1):79–83. doi:10.1016/0304-3959(94)90050-7
- Wertli MM, Rasmussen-Barr E, Weiser S, Bachmann LM, Brunner F. The role of fear avoidance beliefs as a prognostic factor for outcome in patients with nonspecific low back pain: a systematic review. Spine J. 2014;14(5):816–836.e4. doi:10.1016/j.spinee.2013.09.036
- Linton SJ. A review of psychological risk factors in back and neck pain. Spine. 2000;25(9):1148–1156. doi:10.1097/00007632-200005010-00017
- Artus M, Campbell P, Mallen CD, Dunn KM, van der Windt DAW. Generic prognostic factors for musculoskeletal pain in primary care: a systematic review. BMJ Open. 2017;7(1):e012901. doi:10.1136/bmjopen-2016-012901
- Ramond A, Bouton C, Richard I, et al. Psychosocial risk factors for chronic low back pain in primary care–a systematic review. Fam Pract. 2010;28(1):12–21. doi:10.1093/fampra/cmq072
- Jackson T, Wang Y, Wang Y, Fan H. Self-efficacy and chronic pain outcomes: a meta-analytic review. J Pain. 2014;15(8):800–814. doi:10.1016/j.jpain.2014.05.002
- Wessels T, van Tulder M, Sigl T, Ewert T, Limm H, Stucki G. What predicts outcome in non-operative treatments of chronic low back pain? A systematic review. Eur Spine J. 2006;15(11):1633–1644. doi:10.1007/s00586-006-0073-4
- Verkerk K, Luijsterburg PAJ, Miedema HS, Pool-Goudzwaard A, Koes BW. Prognostic factors for recovery in chronic nonspecific low back pain: a systematic review. Phys Ther. 2012;92(9):1093–1108. doi:10.2522/ptj.20110388
- Hill JC, Fritz JM. Psychosocial influences on low back pain, disability, and response to treatment. Phys Ther. 2011;91(5):712–721. doi:10.2522/ptj.20100280
- Alhowimel A, AlOtaibi M, Radford K, Coulson N. Psychosocial factors associated with change in pain and disability outcomes in chronic low back pain patients treated by physiotherapist: a systematic review. SAGE Open Med. 2018;6:2050312118757387. doi:10.1177/2050312118757387
- Kendell M, Beales D, O’Sullivan P, Rabey M, Hill J, Smith A. The predictive ability of the STarT back tool was limited in people with chronic low back pain: a prospective cohort study. J Physiother. 2018;64(2):107–113. doi:10.1016/j.jphys.2018.02.009
- Balagué F, Mannion AF, Pellisé F, Cedraschi C. Non-specific low back pain. Lancet. 2012;379(9814):482–491. doi:10.1016/s0140-6736(11)60610-7
- Grotle M, Foster NE, Dunn KM, Croft P. Are prognostic indicators for poor outcome different for acute and chronic low back pain consulters in primary care? Pain. 2010;151(3):790–797. doi:10.1016/j.pain.2010.09.014
- Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. doi:10.1371/journal.pmed.1000097
- Amundsen PA, Evans DW, Rajendran D, et al. Inclusion and exclusion criteria used in non-specific low back pain trials: a review of randomised controlled trials published between 2006 and 2012. BMC Musculoskelet Disord. 2018;19(1):113. doi:10.1186/s12891-018-2034-6
- Hootman JM, Driban JB, Sitler MR, Harris KP, Cattano NM. Reliability and validity of three quality rating instruments for systematic reviews of observational studies. Res Synth Methods. 2011;2(2):110–118. doi:10.1002/jrsm.41
- Hayden JA, van der Windt DA, Cartwright JL, Côté P, Bombardier C. Assessing bias in studies of prognostic factors. Ann Intern Med. 2013;158(4):280. doi:10.7326/0003-4819-158-4-201302190-00009
- Grotle M, Brox JI, Glomsrød B, Lønn JH, Vøllestad NK. Prognostic factors in first-time care seekers due to acute low back pain. Eur J Pain. 2007;11(3):290–298. doi:10.1016/j.ejpain.2006.03.004
- Woby SR, Watson PJ, Roach NK, Urmston M. Are changes in fear-avoidance beliefs, catastrophizing, and appraisals of control, predictive of changes in chronic low back pain and disability? Eur J Pain. 2004;8(3):201–210. doi:10.1016/j.ejpain.2003.08.002
- Woby SR, Roach NK, Urmston M, Watson PJ. Outcome following a physiotherapist-led intervention for chronic low back pain: the important role of cognitive processes. Physiotherapy. 2008;94(2):115–124. doi:10.1016/j.physio.2007.08.008
- Trinderup JS, Fisker A, Juhl CB, Petersen T. Fear avoidance beliefs as a predictor for long-term sick leave, disability and pain in patients with chronic low back pain. BMC Musculoskelet Disord. 2018;19(1):431. doi:10.1186/s12891-018-2351-9
- Evans DD, Carter M, Panico R, Kimble L, Morlock JT, Spears MJ. Characteristics and predictors of short-term outcomes in individuals self-selecting yoga or physical therapy for treatment of chronic low back pain. PM&R. 2010;2(11):1006–1015. doi:10.1016/j.pmrj.2010.07.006
- Rasmussen-Barr E, Campello M, Arvidsson I, Nilsson-Wikmar L, Äng B-O. Factors predicting clinical outcome 12 and 36 months after an exercise intervention for recurrent low-back pain. Disabil Rehabil. 2011;34(2):136–144. doi:10.3109/09638288.2011.591886
- Sherman KJ, Wellman RD, Cook AJ, Cherkin DC, Ceballos RM. Mediators of yoga and stretching for chronic low back pain. Evid Based Complement Alternat Med. 2013;2013:130818. doi:10.1155/2013/130818
- Macedo LG, Maher CG, Hancock MJ, et al. Predicting response to motor control exercises and graded activity for patients with low back pain: preplanned secondary analysis of a randomized controlled trial. Phys Ther. 2014;94(11):1543–1554. doi:10.2522/ptj.20140014
- van der Hulst M, Mmr V-H, Kgm G-O, Hermens HJ. Multidisciplinary rehabilitation treatment of patients with chronic low back pain: a prognostic model for its outcome. Clin J Pain. 2008;24(5):421–430. doi:10.1097/ajp.0b013e31816719f5
- Verkerk K, Luijsterburg PAJ, Heymans MW, et al. Prognosis and course of pain in patients with chronic non-specific low back pain: a 1-year follow-up cohort study. Eur J Pain. 2015;19(8):1101–1110. doi:10.1002/ejp.633
- Niemistö L, Sarna S, Lahtinen‐Suopanki T, Lindgren K, Hurri H. Predictive factors for 1‐year outcome of chronic low back pain following manipulation, stabilizing exercises, and physician consultation or physician consultation alone. J Rehabil Med. 2004;36(3):104–109. doi:10.1080/16501970310019151
- Smeets RJEM, Vlaeyen JWS, Hidding A, et al. Active rehabilitation for chronic low back pain: cognitive-behavioral, physical, or both? First direct post-treatment results from a randomized controlled trial [ISRCTN22714229]. BMC Musculoskelet Disord. 2006;7:5. doi:10.1186/1471-2474-7-5
- Pincus T, Smeets RJEM, Simmonds MJ, Sullivan MJL. The fear avoidance model disentangled: improving the clinical utility of the fear avoidance model. Clin J Pain. 2010;26(9):739–746. doi:10.1097/ajp.0b013e3181f15d45
- Saunders B, Hill JC, Foster NE, et al. Stratified primary care versus non-stratified care for musculoskeletal pain: qualitative findings from the STarT MSK feasibility and pilot cluster randomized controlled trial. BMC Fam Pract. 2020;21(1):31.
- Maxwell SE, Cole DA. Bias in cross-sectional analyses of longitudinal mediation. Psychol Methods. 2007;12(1):23–44. doi:10.1037/1082-989x.12.1.23
- Palinkas LA. Causality and causal inference in social work: quantitative and qualitative perspectives. Res Soc Work Pract. 2014;24(5):540–547. doi:10.1177/1049731514536056
- Lee H, Hübscher M, Moseley GL, et al. How does pain lead to disability? A systematic review and meta-analysis of mediation studies in people with back and neck pain. Pain. 2015;156(6):988–997. doi:10.1097/j.pain.0000000000000146
- Woby SR, Urmston M, Watson PJ. Self-efficacy mediates the relation between pain-related fear and outcome in chronic low back pain patients. Eur J Pain. 2007;11(7):711–718. doi:10.1016/j.ejpain.2006.10.009