
Abstract
Objective
Our study aimed to investigate the effects of computer-assisted cognitive remediation therapy (CCRT) on cognitive function, social function and quality of life in patients with vascular dementia (VD).
Methods
Ninety-eight patients with VD were treated with CCRT in four 45-minute sessions per week over a course of 40 sessions to exercise four cognitive functions, including flexibility, working memory, plan execution and social cognition. The Mini-Mental State Examination (MMSE), Social Disability Screening Schedule (SDSS), Personal and Social Performance Scale (PSP), and Generic Quality of Life Inventory-74 (GQOL-74) were used to assess before and after treatment.
Results
(1) The scores of orientation (5.60 ± 1.35), calculation (2.20 ± 0.79), verbal ability (7.10 ± 0.36), spatial ability (0.78 ± 0.42), immediate memory (2.42 ± 0.53), short-term memory (1.17 ± 0.78) and MMSE (23.36 ± 2.98) were all improved after treatment (P < 0.05) compared with those before treatment; (2) The scores of SDSS, PSP and Activities of Daily Living (ADL) after treatment were 8.23 ± 0.94, 81.36 ± 14.23, and 32.7 ± 12.1, and all of which improved (P < 0.05); (3) The scores of physical health were 68.24 ± 7.44, mental health were 69.75 ± 7.15, social function were 69.08 ± 7.43, material life were 37.46 ± 4.85 and the total score were 230.79 ± 9.56, all of which improved (P < 0.05).
Conclusion
For patients with VD, CCRT can improve their cognitive function, social function, daily life ability and quality of life.
Introduction
Vascular dementia (VD) is caused by cerebrovascular disease that results in neurological damage to the brain,Citation1,Citation2 which progresses in a stepwise manner. The patient’s memory and intelligence are obviously decreased, while personality and understanding are relatively intact, and the disease can be reversed if treated early.Citation3 At present, clinical treatment of VD mostly adopts pharmacotherapy, which can control the disease, but the effect of improving cognitive and social functions is less satisfactory, and it is difficult for patients to return to society. Currently, computer-assisted cognitive remediation therapy (CCRT) is widely used to treat mental disorders to improve patients’ memory and intelligence. Studies have shown that CCRT improves cognitive function while enhancing patients’ social function and ability to live and work and is a non-pharmacological treatment and rehabilitation measure for mental disability with definite efficacy and wide application prospects. The approach taken in the CCRT treatment is human-computer interaction, using the CCRT system as a tool for cognitive training under the guidance of therapists 4–5 times a week for 45 minutes per session, usually over a course of 40 sessions. Studies have confirmed that CCRT significantly improves the cognitive and social function of patients with schizophrenia and significantly improves the brain function of the prefrontal lobe and other areas of the brain simultaneously.Citation4,Citation5 However, CCRT is seldom used in the treatment of VD, and its effect on the recovery of functions in these patients remains unknown. Further study of the efficacy of CCRT in patients with VD will help elucidate the pathophysiology of VD and provide a promising approach for future treatment. Therefore, in this study, CCRT was performed on 98 patients with VD to investigate the effects of CCRT on cognitive function, social function and quality of life in patients with VD.
Materials and Methods
Participants
Patients with VD who had received treatment in our hospital from January 2017 to January 2018 were selected for this study. Patients who were diagnosed as VD according to the NINDS–AIREN criteria were considered for recruitment.Citation6 The causes of VD were: 1) cerebral infarction; 2) cerebral haemorrhage; 3) cerebral infarction combined with cerebral haemorrhage. Exclusion criteria: 1) diagnosis of Alzheimer’s Disease according to National Institute of NINDS–AIREN criteria;Citation6 2) patients with psychiatric disorders, such as bipolar disorder, depression and anxiety diagnosed according to DSM IV criteria;Citation7 3) drug allergy (clozapine, risperidone, olanzapine, ziprasidone, quetiapine, etc.); 4) other serious underlying diseases, such as abnormal kidney and cardiopulmonary function, and coagulation abnormalities. This study was conducted with approval from the Ethics Committee of our hospital. Written informed consent was obtained from all participants.
Methods
In this cross-sectional study, the therapist treated patients with VD with CCRT and instructed the patients to practise graduated training to exercise four cognitive functions, including flexibility, working memory, plan execution, and social cognition. Each domain of the training included 3 to 10 different cognitive correction exercises, and each exercise had 10 to 25 difficulty levels. During the treatment, the computer automatically evaluated the correctness of the patient’s response, provided timely feedback, and automatically adjusted the treatment plan according to the patient’s treatment performance. CCRT was conducted in four 45-minute sessions per week over a course of 40 sessions.
The CCRT system correction task covered six treatment modules: motor speed, attention and vigilance, perceptual processing, working memory, executive function and social cognition. This system mainly included graphic reasoning, searching coins, distinguishing positive and negative numbers, looking for single and double numbers, fast matching, searching birds, sequence of numbers, graphics matching, sounds matching, practice of single finger, continuous matching, finding different words, digital memory, pattern classification, flying birds searching, counting order attachment, numerical reasoning, building blocks, digital search, shopping plan, emotional management, sorting, classification, searching differences, emotion inference, lexical raindrops, sustained attention, four finger exercises, facial expression recognition and other training.
Assessment
Before and after treatment, patients’ cognitive function, social function, daily life ability and quality of life were assessed with Mini-Mental State Examination (MMSE), Social Disability Screening Schedule (SDSS), Personal and Social Performance Scale (PSP), Activities of Daily Living (ADL) and Generic Quality of Life Inventory-74 (GQOL-74).Citation8,Citation9
Statistical Analysis
Calculation of sample size and statistical analysis was performed using SPSS 24.0 software. The quantitative data that obey the normal distribution were expressed as mean ± standard deviation (), and an independent sample t-test was used for comparison before and after treatment. Quantitative data that did not follow a normal distribution were represented by the median (min. max.), and the Mann–Whitney U-test was used for comparison before and after treatment. The qualitative data were expressed by percentages (n,%), and the χ2 test was used for comparison before and after treatment. P-values <0.05 indicated that the difference was statistically significant.
Results
General Information
A total of 98 patients with VD were enrolled in this study, which consisted of 54 males and 44 females, aged between 58 and 82 years, mean (62.47 ± 10.23) years, and the duration of VD was from 6 to 23 months, mean (14.16 ± 1.27) months. The basic characteristics of the included population are shown in .
Table 1 Baseline Characteristics of Included Population
Cognitive Function Scores of Patients with VD Before and After CCRT Treatment
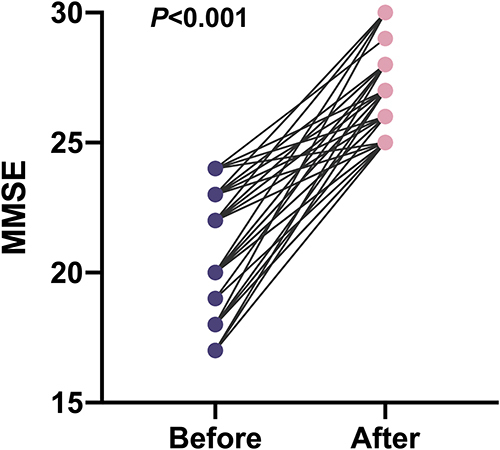
As the 98 patients with VD were treated with CCRT, the individual scores and total scores of orientation, numeracy, verbal ability, spatial ability, immediate memory and short-range memory on the MMSE improved compared with those before treatment (), and the differences were statistically significant (P < 0.05) as shown in .
Table 2 Comparison of Cognitive Function Scores in Patients with Vascular Dementia Before and After Treatment (Scores, )
Figure 1 Scatter plot of MMSE total score before and after the intervention of CCRT.
Social Function and Daily Life Ability Scores of Patients with VD Before and After CCRT Treatment
The 98 patients with VD treated with CCRT had improved scores on the SDSS, PSP and ADL compared with those before treatment, and the differences were all statistically significant (P < 0.05), as shown in .
Table 3 Comparison of Scores for Social Function and Daily Life Ability in Patients with Vascular Dementia Before and After Treatment (Scores, )
Quality of Life Scores of Patients with VD Before and After CCRT Treatment
After treatment with CCRT, the scores of physical health, mental health, social function and material life of GQOL-74 in 98 patients with VD were significantly higher than those before treatment (P < 0.05), as shown in .
Table 4 Comparison of Quality of Life Scores in Patients with Vascular Dementia Before and After Treatment (Scores, )
Discussion
CCRT is widely used in the psychiatric community. It is a method of reinforcement correction by an error-free and synchronised programme, which allows patients to carry out task training according to computer operations. The operation is simple and can guide patients in cognitive training from different angles. However, CCRT is more frequently used in the treatment of schizophrenia and less frequently used in vascular dementia.
In contrast to Alzheimer’s dementia or irreversible cognitive impairment, the treatment and prevention of vascular cognitive impairment caused by cerebrovascular illness are feasible since the risk factors for the condition are established. Therefore, individuals with vascular cognitive impairment who now have a moderate cognitive impairment but have underlying risk factors for worsening may benefit from early identification, prevention, and therapy. Various medications have been shown in several clinical studies to improve vascular cognitive impairment, although few of these medications have received formal licensing.Citation10 Drug treatment provides the benefit of enhancing a few functional and behavioural elements of a patient’s life, but because of its possible side effects or unproven effectiveness, nondrug therapy is largely used to make up for its shortcomings.Citation11 In Eastern medicine, electroacupuncture (EA) is a procedure that delivers a mild current via a needle stimulator into two or more acupuncture sites to offer electrical stimulation, which has been shown to improve cognitive impairment.Citation12 A growing body of evidence suggests that cognitive corrective training (CRT) is effective in improving cognitive deficits and concomitant dysfunction in patients with schizophrenia. Penadés et alCitation13 reported that, compared to social skills training, paper-and-pencil task CRT produces significantly greater improvements in the fractional anisotropy index of white matter in the corpus callosum and the right posterior thalamic radiation. Eack et alCitation14 showed that computer-assisted CRT protects against GM loss in the hippocampus, parahippocampal gyrus, and left fusiform gyrus, as evidenced by a 2-year follow-up study that compared patients with and without CRT.
The results of this study showed that the individual scores and total scores of the MMSE in patients with VD improved after CCRT compared with the pre-treatment scores, and this study further confirmed that CCRT has an auxiliary effect on improving intelligence. Scores on the SDSS, PSP and ADL also improved in 98 patients with VD after CCRT treatment compared with those before treatment.
This study found that the MMSE, SDSS, PSP, ADL and GQOL-74 scores of patients with VD improved after CCRT treatment, which is consistent with the findings of domestic scholars.Citation15–17 It is suggested that CCRT can improve attention, memory and learning ability through visual stimulation and optimal training for patients with VD, thus improving their cognitive function. With the improvement of cognitive function in patients with VD, the social function, daily life ability and quality of life of patients also gradually improved, which also improved the quality of life of patients’ families, and greatly encouraged the attitude of patients and their families towards the disease and life and increased the social recognition of treatment and rehabilitation of patients with dementia. As has been seen in more recent years, the COVID epidemic has led to a new method for telemedicine, and various research has attempted to determine the viability of technology equipment for evaluating and enhancing treatment for individuals with dementia. The treatment of patients with dementia and the assistance of their carers has shown promise with non-pharmacological approaches and innovative technology.Citation18,Citation19 The translational strategy for these approaches involves transferring what is technologically possible remotely. Therefore, CCRT is a tool with great potential that may benefit from the current new technological paradigm.Citation20–22
Conclusion
In summary, CCRT for patients with VD can improve patients’ memory, comprehension, judgement, intelligence and other cognitive functions, thereby improving their daily life ability and quality of life.
Abbreviations
CCRT, computer-assisted cognitive remediation therapy; VD, vascular dementia; MMSE, Mini-Mental State Examination; SDSS, Social Disability Screening Schedule; AD, Alzheimer’s disease; PSP, Personal and Social Performance; ADL, Activities of Daily Living; GQOL-74, Generic Quality of Life Inventory-74.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics approval and consent to participate
This study was conducted in accordance with the declaration of Helsinki. This study was conducted with approval from the Ethics Committee of Wuhan Wudong Hospital. Written informed consent was obtained from all participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
Acknowledgments
No funding or sponsorship was received for this study or publication of this article.
Additional information
Funding
References
- Ou CY, Li CL. Research progress in the mechanism of vascular dementia-related risk factors. Chin J Clin. 2016;10:248–251. doi:10.3877/cma.j.issn.1674-0785.2016.02.021
- Zhou XF, Ji QM, Li MC. Effects of computer cognitive correction therapy on social functioning in vascular dementia. Front Med. 2018;31:355–356. doi:10.3969/j.issn.2095-1752.2018.31.300
- Kalaria RN. Neuropathological diagnosis of vascular cognitive impairment and vascular dementia with implications for Alzheimer’s disease. Acta Neuropathol. 2016;131(5):659–685. doi:10.1007/s00401-016-1571-z
- Zou YZ, Tan SP, Zhou DF, et al. Research and application of computerized cognitive correction therapy (CCRT) technology Beijing Huilongguan Hospital; 2012. Available from: https://d.wanfangdata.com.cn/cstad/ChFDc3RhZE5ld1MyMDIyMDkwMRIKMTIwMDIxMDM1MBoIOHpva2lyN2g%3D
- Ji QM, Li MC. Advances in CCRT on cognitive function in schizophrenia. Med info. 2015;28(19):346. doi:10.3969/j.issn.1006-1959.2015.19.521
- Román GC, Tatemichi TK, Erkinjuntti T, et al. Vascular dementia: diagnostic criteria for research studies. Report of the NINDS-AIREN International Workshop. Neurology. 1993;43(2):250–260. doi:10.1212/wnl.43.2.250
- American Psychiatric Association. Diagnostic Criteria from DSM-IV, by the American Psychiatric Association. Washington, DC: American Psychiatric Press Inc; 1994.
- American Psychiatric Association. Application of Diagnostic and Statistical Manual of Mental Disorders (DSM) [M]. Beijing: Peking University Press; 2016:1–362.
- Jia YJ, Han N, Wang MR, et al. Application of MoCA and MMSE in screening for cognitive impairment in acute ischemic stroke. Chin J Behavior Med Brain Sci. 2017;26(1):46–50. doi:10.3760/cma.j.issn.1674-6554.2017.01.010
- Ritter A, Pillai JA. Treatment of Vascular Cognitive Impairment. Curr Treat Options Neurol. 2015;17(8):367. doi:10.1007/s11940-015-0367-0
- Na R, Yang JH, Yeom Y, et al. A systematic review and meta-analysis of nonpharmacological interventions for moderate to severe dementia. Psychiatry Investig. 2019;16(5):325–335. doi:10.30773/pi.2019.02.11.2
- Cao H, Wang Y, Chang D, Zhou L, Liu J. Acupuncture for vascular mild cognitive impairment: a systematic review of randomised controlled trials. Acupunct Med. 2013;31(4):368–374. doi:10.1136/acupmed-2013-010363
- Penadés R, Pujol N, Catalán R, et al. Brain effects of cognitive remediation therapy in schizophrenia: a structural and functional neuroimaging study. Biol Psychiatry. 2013;73(10):1015–1023. doi:10.1016/j.biopsych.2013.01.017
- Eack SM, Hogarty GE, Cho RY, et al. Neuroprotective effects of cognitive enhancement therapy against grey matter loss in early schizophrenia: results from a 2-year randomized controlled trial. Arch Gen Psychiatry. 2010;67(7):674–682. doi:10.1001/archgenpsychiatry.2010.63
- Zhu WR, Zhang FL, Xu T, Mu Y. Vascular dementia with different treatments for the impact analysis of its cognitive function. J Int Psychlatry. 2015;42(2):56–59.
- Zhang JQ, Yang Y. Effects of computer assisted training combined with the actual environment training on vascular cognitive impairment with no dementia after stoke. Chin J Physic Med Rehabilitat. 2015;37(5):344–347. doi:10.3760/cma.j.issn.0254-1424.2015.05.006
- Ma RQ. Clinical efficacy and prognosis of NIMOTOP and GINATON combined with rehabilitation training in patients with mild to moderate vascular dementia. Chin J Convalescent Med. 2017;26(9):926–927. doi:10.13517/j.cnki.ccm.2017.09.013
- Toniolo S, Scarioni M, Di Lorenzo F, et al. Dementia and COVID-19, a bidirectional liaison: risk factors, biomarkers, and optimal health care. J Alzheimers Dis. 2021;82(3):883–898. doi:10.3233/JAD-210335
- Bombaci A, Abbadessa G, Trojsi F, et al. Telemedicine for management of patients with amyotrophic lateral sclerosis through COVID-19 tail. Neurol Sci. 2021;42(1):9–13. doi:10.1007/s10072-020-04783-x
- Wei CX, Huang J, Huang XQ. Efficacy of hyperbaric oxygen with computer-assisted cognitive training in the treatment of vascular cognitive disorders. Chin J Pract Nervous Dis. 2016;19(3):123. doi:10.3969/j.issn.1673-5110.2016.03.079
- Yang YY, Yang ZM, Tang JW, Zhou DS, Yu RP. Effects of computer cognitive correction therapy on social function and quality of life in chronic schizophrenia patients. J Clin Psychiatric Med. 2017;27(1):59. doi:10.3969/j.issn.1005-3220.2017.01.023
- Zhou XF, Li MC, Ji QM. Effects of computer cognitive correction therapy on social functioning in vascular dementia. China Rural Health. 2018;24:5.