
Abstract
Introduction
Non-specific neck pain (NSNP) is a rather common symptomatology, and various therapeutic approaches are aimed to treat it, in the field of manual therapy, physiotherapy and pharmacology.
Methods
This retrospective study analyzes 65 subjects treated for NSNP with a neurobiological stimulation administered by medical devices based on radio electric asymmetric conveyer (REAC) technology. Initially, a neuro stimulation treatment called neuro postural optimization (NPO) was administered to improve the coordination of muscle activity and reduce adaptive decompensations. Subsequently, the bio stimulation treatment called tissue optimization (TO) was administered to reduce the algodystrophic and muscle contracture component. The evaluation of the efficacy of these treatments was made through the subjective evaluation of pain by the patients. Data were collected by the use of the numeric pain rating scale (NPRS) and neck pain questionnaire (NPQ), administered before the treatments and at the end of the cycle of therapy.
Results
The analysis of the results shows that this type of approach and treatment scheme is effective in reducing the symptoms of NSNP in both male and female subjects, regardless of their age. Other subjective data not quantified in this study but reported by all subjects, during and after the treatment cycle, were a feeling of lower stiffness of neck and shoulder, a reduction in the thickening of the cervicobrachial tissues, and a clear and progressive reduction of pain perception during the skin rolling (SR) maneuver.
Conclusion
The combination of REAC-NPO neuromodulation and REAC-TO biomodulation treatments used in this study was shown to be effective in NPRS.
Introduction
The term non-specific neck pain (NSNP) describes a symptomatologic situation not determined by anatomical anomalies or specific diseases. NSNP is a musculoskeletal pain, particularly widespread among young people of working age, and it lacks of effectiveness of drug treatment. NSNP represents a serious public health problem and has also become a major cause of disability worldwide. Every year, 27% to 48% of workers suffer from NSNP.Citation1 Although there is no accepted definition for the acute, sub-acute or chronic concept of NSNP,Citation2 when the symptomatology has persisted for more than 12 weeks, NSNP is generally defined chronic.Citation3
The origin of NSNP is probably multifactorial,Citation4 and for this reason, it is difficult to formulate a precise treatment and prognosis.
Beyond age, gender, genetic factors and smoking, the main risk factors involved in NSNP can basically be divided into three branches, the first of a physical type such as physical stress from flawed positions,Citation5 postural imbalance or poor postural control.Citation6 The second branch of risk factors is of psychic types, such as psycho-emotional stress, anxiety, worries, and passive coping.Citation7 The third branch can be attribute to nonspecific autonomic dysfunctionsCitation8 and inflammatory pictures.
NSNP is generally not dangerous for the person’s life, but it can be very unpleasant for the quality of life. For this reason, various therapeutic approaches can be found in the literature, each aimed at treating specific components of NSNP’s multifactoriality.Citation2 Among these, we mention manual therapies, massages, physical therapies, such as transcutaneous electrical nerve stimulation (TENS),Citation9 percutaneous electrical nerve stimulation (PENS); laser and low-level laser therapy;Citation10 acupuncture;Citation11 pain killer steroids and non-steroidal anti-inflammatory drugs.
In some literature reviews, these treatments seem to have positive results in improving the symptomatic picture of NSNP,Citation3 while in others this efficacy is not confirmed.Citation2,Citation12
The only approach that demonstrates strong evidence of effectiveness is the chronic multimodal approach, which involves mobilizations/manipulations combined with supervised exercises.Citation2
Even with all the limitations of this type of study, this retrospective study aims to analyze the results obtained with a multimodal approach. This approach consisted of a neuromodulation treatment and subsequently a cycle of biomodulation treatments, using the radio electric asymmetric conveyer (REAC) biotechnology.
Materials and Methods
Study Design
Retrospective study in patients with NSNP.
Ethics
This study is part of a broad retrospective and prospective research plan in collaboration between the Postgraduate Program in Health Sciences, Federal University of Amapá, Macapá, Brazil and the Rinaldi Fontani Institute and Foundation, Florence, Italy. This research plan was approved by the ethical committee of the Federal University of Amapá with opinion number 3,640,674. The study was conducted in full compliance with the Declaration of Helsinki – Ethical principles for medical research involving human subjects.
At the time of admission into the clinic, during the preliminary medical examination, all patients received a detailed explanation about the treatments. Informed consent was obtained from all patients, granting researchers permission to access patient data for the purpose of scientific study and publication ensuring patient anonymity.
Population
In this study, we selected and analyzed the data of all the patients who came to our clinic exclusively for NSNP symptoms in the period from 2013 to 2019.
The total population was made up of 65 patients with an average age of 50.83 ± 13.38, including 54 women with an average age of 50.50 and 11 men with an average age of 52.45.
Time Line of the Study
Time zero (T0) patients preliminary assessments; T1 neuro postural optimization (NPO) neuro modulation treatment; T2 Verification of the effectiveness of the treatment NPO, by checking the disappearance of functional dysmetria (FD); T3 tissue optimization (TO) bio modulation treatment cycle; T4 final assessments.
Intervention
Assessment
All patients examined in this study presented spontaneously to the clinic for chronic NSNP symptomatology, in the absence of previous trauma, neuroanatomical alterations or previous or ongoing pathologies.
All patients had previously undergone various pharmacological and physiotherapeutic treatments without benefiting from them.
Before starting the treatment, to exclude a cervical radicular syndrome (CRS), each patient underwent the Valsalva’s manoeuvre, the Spurling’s test, the shoulder abduction sign and the cervical distraction test as well as an anamnestic collection (T0). The choice to use these tests was determined by the fact that these tests have different specificity and sensitivity to exclude CRS and confirm NSNP. In addition, patients were assessed using neck pain questionnaire (NPQ)Citation13 and numeric pain rating scale (NPRS)Citation14 to measure the pain severity of NSNP. Moreover, at T0 the subjects underwent to Functional Dysmetria (FD) assessment, to evaluate global adaptive decompensations in the coordination of muscle activity. This disorder of the neuromotor control can be easily evidenced in lower limbs, by symmetrically placing the operator’s hands on the femoral quadriceps of the subject being examined in supine position, taking care that the nails of the two left and right thumbs are perfectly aligned. When the subject moves from the supine to the sitting position, a progressive misalignment of the two thumbs can be observed and the operator can perceive the asymmetric activation of symmetrical muscle groups, such as the quadriceps muscles. When this altered execution of voluntary movements is present in healthy subjects,Citation15 it is correlated to phenomena of adaptive type at the base of the fluctuating asymmetry.Citation16
Neck Pain Questionnaire (NPQ)
The NPQCitation13 is easy to fill in and can be administered either as an interview or in self-compilation. The results are simple to evaluate and provide a measure to assess the situation of patients with symptomatic NSNP. The NPRS is the most commonly used numerical scale. NPRS is a subjective measure to rate the pain perceived/reported by the patient on an eleven-point numerical scale. Scale values range from 0, no pain, to 10, worst imaginable pain. The NPQ consists of nine items including pain intensity, duration of symptoms, pins and needles or numbness at night, pain affecting sleep, effect on social life, carrying, reading/watching television (TV), working/housework, and driving.Citation13 For each item, there are five potential responses describing a greater degree of difficulty (0 = no difficulty to 4 = severe difficulty). An overall percentage NPQ score is calculated by adding together the scores for each item (0–36) and calculating a percentage (total score/36 x 100%). If items are not applicable, the total potential score is reduced (eg, one item not applicable, total score out of 32). The NPQ has been validated in patients complaining of neck pain attending a rheumatology clinic in the United Kingdom (UK) where mean scores for each item were shown to correlate with intensity of pain.Citation13 It has also been shown to have acceptable test–retest reliabilityCitation13,Citation17 and sensitivity to change.Citation13
Treatments
Treatments consisted in a combination of an initial REAC neuromodulation treatment, followed by a REAC biomodulation treatment consisting of 12 sessions administered over 4/6 weeks. Neuro Postural Optimization (NPO) was the first REAC neuromodulation treatment and tissue optimization (TO-B) was the second REAC biomodulation treatment administered. The patients had never received REAC neurobiological treatments prior to commencing our treatments. Throughout the duration of the REAC NPO and TO-B treatments, patients did not receive any type of treatment, neither pharmacological nor rehabilitative. The treatments were administered using the BENE medical device (ASMED, Florence Italy), CE and ANVISA certified as medical device for neurobiological stimulation.
Radio Electric Asymmetric Conveyer Technology
All the activities of our organism are possible thanks to bioelectric phenomena. Bioelectricity is generated by ionic flows that produce currents and consequently endogenous bioelectric fields (EBF). EBFs are fundamental for neurotransmission and neuromodulation processes, and for reparative/regenerative and anti-inflammatory processes.Citation18 When the generation of EBF is altered by infectious, traumatic or epigenetic factors, the complex neurobiological activities that depend on them are in turn negatively affected. The EBF alterations produce negative modifications in neurotransmission, in reparative/regenerative and anti-inflammatory processes.
REAC technology was designed to reorganize the bioelectric asymmetricity at the base of the ionic flows, to carry out neurobiological stimulation treatments, through EBF manipulation.
Neuro Postural Optimization (NPO)
NPO is a REAC neuromodulation treatment. Thanks to its long action effectiveness, it is normally administered in a single session lasting a few milliseconds.Citation15 The effects of REAC NPO treatment clinically demonstrate an improvement in posture and motor strategies, even in neurodegenerative diseases.Citation19–Citation21 The effects of the REAC NPO treatment can also be assessed with fMRI techniques, through which it is possible to ascertain the positive and functional electrometabolic reorganization of the brain.Citation15,Citation22,Citation23
Tissue Optimization (TO)
TO are a family of REAC biomodulation treatments. The TO treatments (TO-B, TO-CO, TO-ACT, TO-MO, TO-RPR, TO-RGN) have the same general indication of use and administration procedure, but they differ in the timing, according to the type of tissue to be treated.
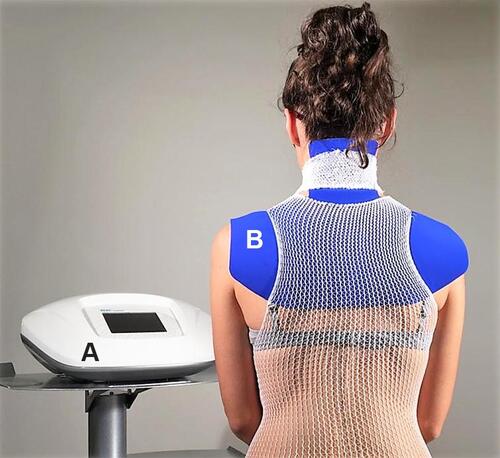
All TO treatments require that the area to be treated is covered by the device’s asymmetric conveyer probe (ACP), in order to focus the recovery of the ionic flows and therefore of the EBF in a localized way (). The clinical effects of TO treatments are basically improvement of tissue metabolism with consequent anti-edema, anti-inflammatory and regenerative effect.Citation24–Citation26 These effects have also been demonstrated with basic research at the molecular levelCitation27–Citation29 and on the animal model.Citation30–Citation33
Figure 1 The image shows the example of a patient suffering from non-specific neck pain during the administration of the tissue optimization treatment. (A) device based on REAC technology, model BENE 101 (ASMED, Florence, Italy); (B) asymmetric conveyer probe (ACP). The ACP is connected to device (A) via a specific connection cable. The ACP is held in place using an elastic tubular mesh.
Data and Statistic
The NPRS and NSNP data were collected during the first visit before any treatment and at the end of the treatments. The data extrapolated from the medical records and tests were reported on a spreadsheet and subsequently exported to the IBM SPSS 22 statistical software by an external expert who analyzed the data. The data set was not parametric and some columns were related themselves; therefore, the Wilcoxon test and the Sign test have been chosen for the statistical evaluation.
Results
Neuro Postural Optimization (NPO)
The clinical efficacy assessment of the REAC NPO treatment is carried out by evaluating the disappearance of the asymmetrical activation of the quadriceps muscles of the right and left legs during the transition from supine to sitting position and vice versa.
This phenomenon has been linked to epigenetic modifications, which can also express morphological changes.Citation16 This asymmetric activation defined by the authors' functional dysmetria (DF)Citation23 highlights a functional alteration fundamentally of the cerebellar circuits underlying motor coordination.Citation15,Citation22 In all patients, the presence of DF was found at T0, before NPO treatment. DF disappearance was found in all patients after NPO treatment (T1). DF disappearance has proven to be long lasting, up to the end of the treatments (T4). Although this data has not been quantified, after the NPO all subjects reported a feeling of greater postural comfort and stability and a feeling of looseness in the movements.
Tissue Optimization (TO)
The clinical efficacy assessment of the REAC TO treatment was fundamentally made on the basis of the reduction of algic symptomatology, evaluated with NPRS and NPQ, because it was the most perceived symptomatology and it most conditioned the patients’ quality of life.
NPRS and NPQ data set were statistically processed and a statistical significance p<0.005 was found considering each item ( and ).
Table 1 Wilcoxon and Sign Test Statistical Analysis Results for Numeric Pain Rating Scale Results
Table 2 Wilcoxon and Sign Test Statistical Analysis Results for Neck Pain Questionnaire
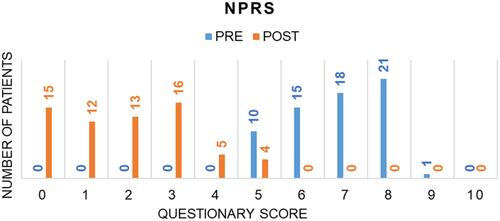
The initial NPRS average score at T0 was 6.81 and at T4 it was 1.94, with an average reduction of the symptom of 71.52% ().
Figure 2 Graphical representation of the variation in the distribution of the number of subjects by intensity of referred pain measured with the numeric pain rating scale, before (T3) and after (T4) the treatments.
NPQ data are shown in and -. For pain intensity, the average score at T0 was 2.58 and at T4 it was 0.57, with an average 77.91% reduction of the symptom (). For sleeping, the average score at T0 was 1.77 and at T4 it was 0.47, with an average 73.45% reduction of the symptom (). For numbness, the average score at T0 was 0.80 and at T4 it was 0.12, with an average 85% reduction of the symptom (). For duration, the average score at T0 was 2.87 and at T4 it was 0.61, with an average 78.75% reduction of the symptom (). For carrying, the average score at T0 was 2.27 and at T4 it was 0.86, with an average 62.12% reduction of the symptom (). For reading/television, the average score at T0 was 2.40 and at T4 it was 0.87, with an average 63.75% reduction of the symptom (). For work, the average score at T0 was 2.04 and at T4 it was 0.64, with an average 68.63% reduction of the symptom (). For social, the average score at T0 was 2.20 and at T4 it was 0.47, with an average 78.64% reduction of the symptom (). For driving, the average score at T0 was 2.46 and at T1 it was 0.69, with an average 71.96% reduction of the symptom ().
Table 3 Comparison Between the Data of the Neck Pain Questionnaire, Collected Before (T3) and After the Treatments (T4)
Figure 3 Graphical representation of the variation in the distribution of the number of subjects before (T3) and after (T4) the treatments, for the symptoms: intensity, sleeping, numbness, and duration evaluated with the neck pain questionnaire.
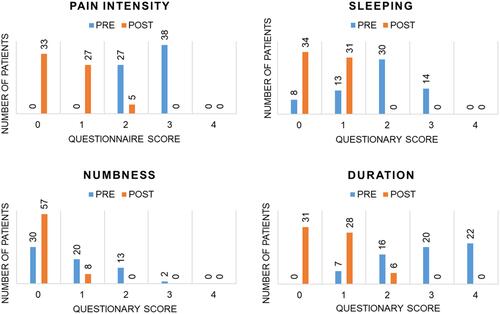
Figure 4 Graphical representation of the variation in the distribution of the number of subjects before (T3) and after (T4) the treatments, for carrying, reading/television, work, social, and driving evaluated with the neck pain questionnaire.
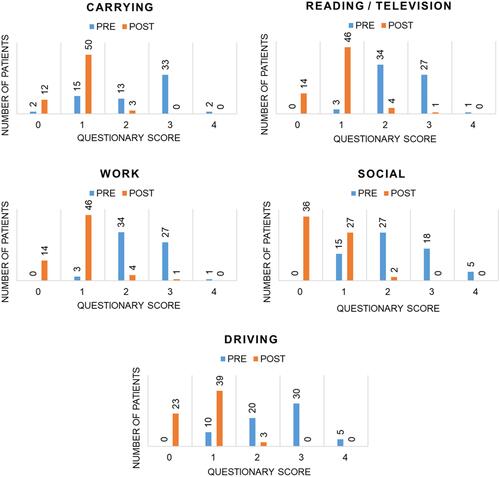
Figure 5 Graphical representation of the overall improvement percentage evaluated with the neck pain questionnaire at the end of the treatments (T4).
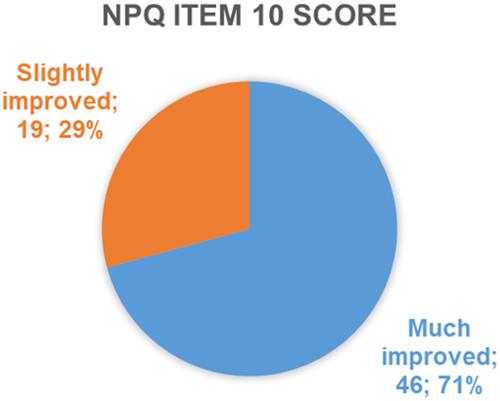
NPQ item 10 assesses how the patient perceives and reports his condition after the treatment, compared to his initial condition. At T4, 100% of the subjects reported having benefited from the treatment. In particular, 46 subjects, equal to 71%, reported being much improved and 19 subjects, equal to 29%, reported a slight improvement ().
Moreover, from a clinical semeiological point of view, the effectiveness of the TO treatment was assessed with the Skin rolling (SR) maneuver,Citation34 carried out in the cervicobrachial region of the subjects being treated. The SR or detachment maneuver affects the skin. It consists in lifting the skin between the thumb and forefinger joined, both hands or one hand. The SR determines a stimulation on the vascular sympathetic system, causing an ischemia followed by a longer-lasting hyperemia. Moreover, SR also tends to promote the mobility of the tissues on the deep planes and intensely stimulates the sensitive skin terminations, with the production of an algic response, sometimes very intense. All the subjects reported a feeling of less thickening and hardening of the tissues, and a clear and progressive reduction of the pain perception during the SR maneuver during and after the TO treatment cycle. This data has not been quantified, because there is no validated test and execution method of the SR maneuver.
Discussion
NSNP represents an increasingly widespread symptomatic picture, whose etiopathogenetic cause has not been precisely found, up to now. Currently, NSNP is believed to have a multifactorial origin, which involves causes due to working position, poor postural control, psycho-emotional factors, environmental stress, nonspecific autonomic dysfunctions,Citation8 and nonspecific inflammatory processes. Probably this is why the reviews of the specific literature highlighted how various treatments that have proven to be effective in other symptomatic pictures, have little or no efficacy in treating NSNP.
The importance of EBF in both non-excitable and excitable cells, such as nerve and muscle cells, has been a well-known fact for a long time.Citation18 Numerous studies have shown the fundamental importance of EBF in coordinating cell behavior and regulating cell migration, orientation, nerve growth and wound healing.Citation18
In this retrospective study, we can highlight a multifactorial approach with the REAC neurobiological stimulation treatments in NSNP. In fact, REAC neurobiological stimulation treatments addressed various components that contribute to producing and maintaining the symptoms of NSNP.
The NPO treatment is effective on the postural neuromotor component, which induces muscle tone dysfunction, muscle stiffness, reduced mobility, circulatory disorders, and pain. These disorders inhibit reparative processes, because the constant muscle tension affects muscle blood circulation, altering muscle metabolism. The consequent accumulation of catabolites induces the algodystrophic processes.
In order to improve muscle metabolism and reduce muscle microcirculatory suffering and its consequences, TO-B biostimulation treatment was used. The TO treatments are aimed at improving tissue metabolism and reducing the inflammatory-algodystrophic component underlining the vicious circuit that boosts the symptomatic picture. In fact, one of the major problems in chronic symptomatic pictures is the trigger of vicious circles. In the case of NSNP, the involuntary and unconscious constant contraction of the cervical musculature leads to circulatory distress of the muscles of this district. The results of this process are expressed in an altered cellular metabolism with the production of catabolites. Because of tissue microcirculatory suffering, the catabolites cannot be eliminated and therefore remain localized in the tissues, feeding the vicious circle and the symptomatic picture. At a molecular level, these processes are expressed as an alteration of ionic flows, thus altering the correct formation of EBF. To break this vicious circle, it is important to act at the molecular level, by restoring the correct activity of ionic fluxes, and then the EBF.
Conclusion
Generally, retrospective studies have important limitations in the quality and quantity of data available for analysis, since the data were rarely collected in accordance with the needs of the study. This study overcame this important limitation, as all the subjects included in this retrospective analysis from the first medical visit, had been carefully investigated for the anamnestic, semeiological, clinical, symptomatic and psychometric-specific aspects. This retrospective study collects and analyzes for the first-time data from subjects with NSNP treated in succession with two REAC treatment protocols, the first of neurostimulation: NPO and the second of biostimulation: TO. The NPRS and NPQ results confirm that this treatment scheme can be helpful in alleviating the symptoms of NSNP. Of course, studies conducted with more complex procedures will be useful to confirm the results of this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
- Rothfels P, Martin C, Noertjojo K. What’s new in the literature: nonspecific neck pain. BCMJ. 2010;52(3):123.
- Tsakitzidis G, Remmen R, Peremans L, et al. Non-specific neck pain: diagnosis and treatment. KCE reports 119C. Brussels: Belgian Health Care Knowledge Centre (KCE);2009.
- Jensen I, Harms-Ringdahl K. Strategies for prevention and management of musculoskeletal conditions. Neck pain. Best Pract Res Clin Rheumatol. 2007;21(1):93–108. doi:10.1016/j.berh.2006.10.003
- Misailidou V, Malliou P, Beneka A, Karagiannidis A, Godolias G. Assessment of patients with neck pain: a review of definitions, selection criteria, and measurement tools. J Chiropr Med. 2010;9(2):49–59. doi:10.1016/j.jcm.2010.03.002
- Waris P. Occupational cervicobrachial syndromes. A review. Scand J Work Environ Health. 1979;5(suppl 3):3–14. doi:10.5271/sjweh.2688
- Saadat M, Salehi R, Negahban H, Shaterzadeh MJ, Mehravar M, Hessam M. Postural stability in patients with non-specific chronic neck pain: a comparative study with healthy people. Med J Islam Repub Iran. 2018;32:33. doi:10.14196/mjiri.32.33
- Ortego G, Villafañe JH, Doménech-García V, Berjano P, Bertozzi L, Herrero P. Is there a relationship between psychological stress or anxiety and chronic nonspecific neck-arm pain in adults? A systematic review and meta-analysis. J Psychosom Res. 2016;90:70–81. doi:10.1016/j.jpsychores.2016.09.006
- Zaproudina N, Ming Z, Närhi M. Sensory and sympathetic disorders in chronic non-specific neck pain. Funct Neurol. 2015;30(3):165–171.
- Martimbianco ALC, Porfírio GJM, Pacheco RL, Torloni MR, Riera R. Transcutaneous electrical nerve stimulation (TENS) for chronic neck pain. Cochrane Database Syst Rev. 2019;(12). doi:10.1002/14651858.CD011927.pub2.
- Gross AR, Dziengo S, Boers O, et al. Low Level Laser Therapy (LLLT) for neck pain: a systematic review and meta-regression. Open Orthop J. 2013;7:396–419. doi:10.2174/1874325001307010396
- Trinh K, Graham N, Irnich D, Cameron ID, Forget M. Acupuncture for neck disorders. Cochrane Database Syst Rev. 2016;(5):Cd004870.
- InformedHealth.org. What can you do about non-specific neck pain? InformedHealth. Cologne, Germany: Institute for Quality and Efficiency in Health Care (IQWiG); 2015.
- Leak AM, Cooper J, Dyer S, Williams KA, Turner-Stokes L, Frank AO. The Northwick Park Neck Pain Questionnaire, devised to measure neck pain and disability. Br J Rheumatol. 1994;33(5):469–474. doi:10.1093/rheumatology/33.5.469
- Young I Pt D, Dunning J Pt DPT, Butts R Pt P, Mourad F Pt DPT, Cleland J Pt P. Reliability, construct validity, and responsiveness of the neck disability index and numeric pain rating scale in patients with mechanical neck pain without upper extremity symptoms. Physiother Theory Pract. 2019;35(12):1328–1335. doi:10.1080/09593985.2018.1471763
- Rinaldi S, Mura M, Castagna A, Fontani V. Long-lasting changes in brain activation induced by a single REAC technology pulse in Wi-Fi bands. Randomized double-blind fMRI qualitative study. Sci Rep. 2014;4:5668. doi:10.1038/srep05668
- Parsons PA. Fluctuating asymmetry: an epigenetic measure of stress. Biol Rev Camb Philos Soc. 1990;65(2):131–145. doi:10.1111/j.1469-185X.1990.tb01186.x
- Wlodyka-Demaille S, Poiraudeau S, Catanzariti JF, Rannou F, Fermanian J, Revel M. French translation and validation of 3 functional disability scales for neck pain. Arch Phys Med Rehabil. 2002;83(3):376–382. doi:10.1053/apmr.2002.30623
- Levin M, Pezzulo G, Finkelstein JM. Endogenous bioelectric signaling networks: exploiting voltage gradients for control of growth and form. Annu Rev Biomed Eng. 2017;19:353–387. doi:10.1146/annurev-bioeng-071114-040647
- Fontani V, Rinaldi S, Castagna A, Margotti ML. Noninvasive radioelectric asymmetric conveyor brain stimulation treatment improves balance in individuals over 65 suffering from neurological diseases: pilot study. Ther Clin Risk Manag. 2012;8:73–78.
- Olazaran J, Gonzalez B, Lopez-Alvarez J, et al. Motor effects of REAC in advanced Alzheimer’s disease: results from a pilot trial. J Alzheimers Dis. 2013;36(2):297–302. doi:10.3233/JAD-130077
- Olazaran J, Gonzalez B, Osa-Ruiz E, et al. Motor effects of radio electric asymmetric conveyer in Alzheimer’s disease: results from a cross-over trial. J Alzheimers Dis. 2014;42(1):325–332. doi:10.3233/JAD-140417
- Rinaldi S, Fontani V, Castagna A. Brain activity modification produced by a single radioelectric asymmetric brain stimulation pulse: a new tool for neuropsychiatric treatments. Preliminary fMRI study. Neuropsychiatr Dis Treat. 2011;7:649–654. doi:10.2147/NDT.S26123
- Mura M, Castagna A, Fontani V, Rinaldi S. Preliminary pilot fMRI study of neuropostural optimization with a noninvasive asymmetric radioelectric brain stimulation protocol in functional dysmetria. Neuropsychiatr Dis Treat. 2012;8:149–154.
- Castagna A, Fontani V, Rinaldi S, Mannu P. Radio electric tissue optimization in the treatment of surgical wounds. Clin Cosmet Investig Dermatol. 2011;4:133–137.
- Fontani V, Castagna A, Mannu P, Rinaldi S. Radioelectric asymmetric stimulation of tissues as treatment for post-traumatic injury symptoms. Int J Gen Med. 2011;4:627–634.
- Collodel G, Fioravanti A, Pascarelli NA, et al. Effects of regenerative radioelectric asymmetric conveyer treatment on human normal and osteoarthritic chondrocytes exposed to IL-1beta. A biochemical and morphological study. Clin Interv Aging. 2013;8:309–316.
- Maioli M, Rinaldi S, Santaniello S, et al. Radiofrequency energy loop primes cardiac, neuronal, and skeletal muscle differentiation in mouse embryonic stem cells: a new tool for improving tissue regeneration. Cell Transplant. 2012;21(6):1225–1233. doi:10.3727/096368911X600966
- Maioli M, Rinaldi S, Santaniello S, et al. Radio electric conveyed fields directly reprogram human dermal skin fibroblasts toward cardiac, neuronal, and skeletal muscle-like lineages. Cell Transplant. 2013;22(7):1227–1235. doi:10.3727/096368912X657297
- Maioli M, Rinaldi S, Santaniello S, et al. Radioelectric asymmetric conveyed fields and human adipose-derived stem cells obtained with a nonenzymatic method and device: a novel approach to multipotency. Cell Transplant. 2014;23(12):1489–1500. doi:10.3727/096368913X672037
- Lorenzini L, Giuliani A, Sivilia S, et al. REAC technology modifies pathological neuroinflammation and motor behaviour in an Alzheimer’s disease mouse model. Sci Rep. 2016;6:35719. doi:10.1038/srep35719
- Berlinguer F, Pasciu V, Succu S, et al. REAC technology as optimizer of stallion spermatozoa liquid storage. Reprod Biol Endocrinol. 2017;15(1):11. doi:10.1186/s12958-017-0229-6
- Sanna Passino E, Rocca S, Caggiu S, et al. REAC regenerative treatment efficacy in experimental chondral lesions: a pilot study on ovine animal model. Clin Interv Aging. 2017;12:1471–1479.
- Panaro MA, Aloisi A, Nicolardi G, et al. Radio electric asymmetric conveyer technology modulates neuroinflammation in a mouse model of neurodegeneration. Neurosci Bull. 2018;34(2):270–282. doi:10.1007/s12264-017-0188-0
- Bansevicius D, Pareja JA. The “skin roll” test: a diagnostic test for cervicogenic headache? Funct Neurol. 1998;13(2):125–133.