
Abstract
Background
Musculoskeletal pain is one of the most complex and debilitating types of pain. Although different pharmacologic treatments are available, very few studies have explored the predictors for opioid analgesics prescription to manage this type of pain.
Objective
The aim of this study was to explore the predictors for opioid prescription in patients with acute musculoskeletal pain in Saudi Arabia.
Methods
This was a single-center, retrospective chart review of adult patients (≥18 yrs.) with an acute nociceptive musculoskeletal pain at a university-affiliated medical center in Riyadh, Saudi Arabia. Cancer patients and those with chronic neuropathic pain were excluded. Patients’ age, gender, number of comorbidities, duration of pain management, number of clinic visits for pain, and Numeric Pain Rating Scale (NPRS) scores at rest and with normal activities were collected. Multiple logistic regression was conducted to examine the relationship between the type of musculoskeletal pain and the prescription of opioid analgesics controlling for NPRS score on activity, age, gender, number of comorbidities, duration of pain treatment, and number of clinic visits for pain.
Results
The mean age of the 227 patients, who met the inclusion criteria, was 39 years and 68% of them were male. Sixty-three percent of the patients were prescribed opioid analgesics, and 61% of them had shoulder pain, 29% had back pain, and 10% had lower extremity pain (eg, hip, thigh, lower leg, knee, ankle, and foot pain). Tramadol was the most commonly prescribed opioid analgesic (82%), followed by codeine (13%). Ninety-seven percent of patients who were prescribed non-opioid analgesics had shoulder pain. Patients with shoulder pain had lower odds of receiving opioid analgesics (OR=0.019, P<0.0001, 95% CI=0.004–0.081) in comparison to their counterparts who had lower extremity or back pains. Moreover, the higher the pain score on activity was, the higher odds of receiving opioid analgesics (OR=1.317, P<0.0001, 95% CI=1.029–1.685).
Conclusion
Future studies should explore the impact of different opioid prescribing policies to improve the quality of patient care and reduce the unnecessary prescribing of opioids for patients with non-cancer musculoskeletal pain.
Introduction
Musculoskeletal disorders include more than 150 diagnoses affecting muscles, bones, joints and associated tissues, such as tendons and ligaments, as stated in the International Classification of Diseases.Citation1 These conditions can occur anytime during people’s lifetime resulting in persistent pain that negatively impact their quality of life. Musculoskeletal pain is one of the most commonly encountered pain in healthcare settings, and is considered the largest cause of disability in many countries, such as the United Kingdom.Citation2–Citation4 It was found to be one of the three major causes of the global burden of non-communicable diseases in 2016 representing about 16% of all disability adjusted life-years (DALYs).Citation5 Moreover, it was reported that musculoskeletal pain and disorders account for 22.6% of the total costs of illnesses in Sweden.Citation6 In the United Kingdom, the cost of opioid prescriptions for musculoskeletal pain management varied from £3 to £4,844 per patient per year, and the cost of opioid overprescription could exceed £100 million per year assuming that 40% of patients with musculoskeletal pain are overprescribed.Citation2 The cost of managing musculoskeletal pain is not limited to the cost of prescriptions or clinic visits; the productivity loss and absenteeism due to musculoskeletal pain is also significant.Citation7 In Saudi Arabia, few research studies have explored the prevalence of musculoskeletal pain among the public. In a questionnaire-based study that explored the prevalence of musculoskeletal pain among 165 construction workers in the cities of Riyadh and Dammam, 48.5% of the respondents reported having musculoskeletal pain, such as low back and knee pain.Citation8 Musculoskeletal pain was found to be also prevalent among medical professionals. In a study that explored the prevalence of musculoskeletal pain among medical and surgical residents at a tertiary care center in Riyadh, the majority of the respondents (82.5%) reported suffering from musculoskeletal pain at least once during their medical training, and the low back pain was the most prevalent (53%).Citation9 Low back pain is also prevalent among dental practitioners according to multiple studies that explored the prevalence of musculoskeletal pain among dentists in the Kingdom.Citation10–Citation12
Although multiple non-pharmacologic treatments, such as physiotherapy and acupuncture, are used in the management of musculoskeletal pain, pharmacotherapy (eg, nonsteroidal anti-inflammatory drugs (NSAIDs), selective COX-2 inhibitors, oral and injectable corticosteroids, and opioids) remains the mainstay of musculoskeletal pain treatment.Citation13 Opioids are the most commonly prescribed analgesics used in the management of acute musculoskeletal pain.Citation2 Nearly 90% of patients who visit pain clinics in the United Kingdom are prescribed some forms of opioid analgesics.Citation2 Although opioids are deemed to be the most effective analgesics in the management of acute musculoskeletal pain, their use is associated with higher risk of abuse, misuse, and serious adverse events.Citation14 Therefore, the lowest effective dose of opioids should be used for the shortest appropriate period of time whenever needed in the management of musculoskeletal pain.Citation15 Additionally, it was found that the early use of opioids in the management of both acute and chronic musculoskeletal pain has been associated poorer clinical outcomes especially in the case of low back pain according to a recently published systematic review of clinical practice guidelines.Citation16 However, another systematic review and meta-analysis has found that the use of opioids in the management of low back pain is associated with greater pain relief in the short term, but this effect was not observed in the long term.Citation17
There has been an upward trend in the opioids prescribing rate for both acute and chronic musculoskeletal pain globally over the last two decades particularly in the United States.Citation18,Citation19 It is believed the rate of opioids prescription for patients with musculoskeletal pain has seen a 50% increase between the years of 2001 and 2010.Citation18 This was accompanied with a significant increase in the rates of opioid-related death.Citation20 Unfortunately, research studies aimed at exploring the rates of opioids consumption are scarce in the Middle East.Citation21 Although the rates of opioids utilization in the management of pain states have significantly increased in the world over the last two decades, some Middle Eastern countries have seen either a modest increase or a decrease in the rates of opioids utilization.Citation21,Citation22 This could be attributed to several reasons, such as poor palliative care services, lack of essential opioid stock, and strict regulations.Citation22 Although no study has explored the pain management adequacy among patients with musculoskeletal disorders in Saudi Arabia, many believe that there is an underutilization of analgesics in general, and opioids in particular, in the management of musculoskeletal pain.Citation22 This assumption is mainly based on the findings of previously published studies that assessed the pain management adequacy among patients with more severe disease states, such as cancer and cardiac surgery.Citation23,Citation24 Moreover, very few tertiary care hospitals in Saudi Arabia have pain management clinics, and those with such clinics require special forms to be filled for any opioid prescriptions by a medical specialist or consultant only. These regulations besides the local drug enforcement laws that require a narcotic pharmacist to be in charge of auditing all narcotic prescriptions in each public or private hospital as well as the fact that those who engage in any prescription drug diversion can be sentenced to death could explain the reason behind the underutilization of opioid analgesics in Saudi Arabia.Citation22,Citation25 Understanding the predictors for opioids prescription should help in formulating a safe and effective opioid prescribing protocol for patients with musculoskeletal pain.
Therefore, the aim of this study was to explore the predictors for opioids prescription among a sample of patients with acute musculoskeletal pain in Saudi Arabia.
Methods
Study Design, Setting, and Subjects
This was a single-center, retrospective medical chart review study that was conducted at King Khalid University hospital, which is a university-affiliated hospital in Riyadh, Saudi Arabia. The hospital’s bed capacity is 1,200 beds, and it provides primary, secondary, and tertiary health services to university faculty and their families as well as to Saudi citizens on a referral basis. Although the hospital has recently established pain clinics for patients with chronic pain, patients with acute pain are treated with opioid or non-opioid analgesics based on physicians’ discretion. Furthermore, there are no published pain management guidelines for physicians to follow or adhere to. However, only licensed medical specialists or consultants can prescribe opioids for legitimate medical indications.
Adult patients (≥18 years old) with an acute nociceptive musculoskeletal pain who have been seen in the orthopedic outpatient clinics were identified via the hospital electronic health record (EHR) system (eg, Cerner Millennium). Patients with cancer, neuropathic pain, prior use of opioids or substance abuse history, osteoarthritis, and those with other pain disorders that necessitate long-term pain management (eg, inflammatory bowel disease, fibromyalgia, post-trauma or post-surgical pain) were excluded. Systematic random sampling was used by choosing every 100th patient health record of all patients who were prescribed opioid and/or non-opioid analgesics for acute musculoskeletal pain between May 2015 and December 2017. Patients’ age, gender, body mass index (BMI), number of clinic visits, pain location, number of comorbidities, number of prescription medications, duration of pain treatment which was written in the prescriptions for the different dispensed analgesics, and the Numeric Pain Rating Scale (NPRS) scores at rest and with normal activities were collected for both cases (patients on opioid analgesics) and controls (patients on non-opioid analgesics). The NPRS is an 11-point verbal scale which has been validated to assess the pain intensity across multiple patient populations and in different healthcare settings.Citation26 The study was approved by the institutional review board of King Saud University College of Medicine (Research Project No. E-17-2587). No patient consent form was required per the institutional policy since the study was a retrospective chart review, and no personal identifiers were collected. Furthermore, the study adhered to the ethical principles of the declaration Helsinki with regard to data storage and handling.Citation27
Statistical Analysis
Descriptive statistics using means, standard deviations, frequencies, and percentages were used to describe the patient characteristics. The baseline characteristics for the cases (patients on opioid analgesics) and controls (patients on non-opioid analgesics) were compared using Chi-square test, Fisher’s exact test, and Student’s t-test as appropriate. The pain location was dichotomized into shoulder pain versus the other types of pain. Multiple logistic regression analysis to identify the predictors for opioids prescription was conducted and included the following variables: age, gender, NPRS score on activity, number of comorbidities, number of clinic visits, duration of pain treatment, and pain location.Citation28 The minimum sample size for multiple logistic regression that included seven predictor variables for opioids prescription with at least 10 events (cases on opioids) per variable matched to controls (patients with musculoskeletal pain on non-opioid analgesics) based on a 1:1 ratio was estimated to be 140 patients.Citation29 All statistical analyses were conducted using SAS® version 9.4 (SAS institute, Cary, NC, USA).
Results
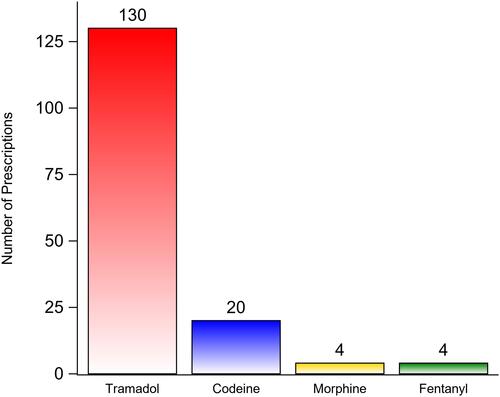
Out of 1,651 randomly selected patients who received prescription analgesics between May 2015 and December 2017, 227 patients met the inclusion criteria and were included in the study. Approximately 64% of the patients with acute musculoskeletal pain were prescribed opioid analgesics. The mean age of the patients was 39 years with no significant difference between the cases (patients on opioid analgesics) and controls (patients on non-opioid analgesics). Most of the patients were male (68.28%) with no significant difference in the percentages of males or females between the two groups. Most of the sampled patients had shoulder pain (60.79%), followed by back pain (29.07%), and lower extremity pain (eg, hip, thigh, lower leg, knee, ankle, and foot pain) (10.13%). The majority of the patients with shoulder pain (97.56%) were prescribed non-opioid analgesics (eg, nonsteroidal anti-inflammatory drugs, celecoxib, and acetaminophen), whereas only two patients with back pain and none of the patients with lower extremity pain were prescribed non-opioid analgesics (P<0.0001). Approximately 21% of the patients who were prescribed opioid analgesics had more than one comorbidity, and 17.24% were taking more than two prescription medications in comparison to 3.66% and 4.88%, respectively, among their counterparts who were prescribed non-opioid analgesics (P<0.05). The mean number of clinic visits for the patients was 1.72 visits with no significant difference between the two groups. Pain treatment mean duration was significantly higher among patients treated with opioid analgesics in comparison to their counterparts on non-opioid analgesics (19.14 days versus 10.44 days, P<0.0001). The mean NPRS scores with activity for patients who were prescribed opioid analgesics was slightly but significantly higher than their counterparts who were prescribed non-opioid analgesics (3.73 versus 3.06, P=0.0012). On the other hand, the mean NPRS scores at rest were not significantly different between the two groups. NO significant difference between the NPRS scores with activity and rest for the different pain locations (eg, lower limb, shoulder, and back pain) was found. The baseline characteristics of the patients are shown in . There were 158 opioid prescriptions dispensed for 145 patients who received opioid analgesics, and tramadol was the most commonly prescribed opioid (82.27%), followed by codeine (12.66%), morphine (2.53%), and fentanyl (2.53%) as shown in . Patients with shoulder pain had 98.1% lower odds of receiving opioid analgesics in comparison to their counterparts with back or lower extremity pain (OR=0.019, 95% CI= 0.004–0.081, P<0.0001) controlling for age, NPRS score with activity, gender, number of comorbidities, duration of pain treatment, and number of clinic visits. On the other hand, patients with lower limb or back pain had more than 50 times higher odds of receiving opioid analgesics in comparison to their counterparts with shoulder pain (OR=53.59, 95% CI= 12.34–232.74, P<0.0001) controlling for age, NPRS score with activity, gender, number of comorbidities, duration of pain treatment, and number of clinic visits. Moreover, every additional point in the NPRS score with activity was associated with 31.7% increase in the odds of receiving opioid analgesics (OR=1.317, 95% CI= 1.029–1.685, P=0.0285) controlling for pain location, age, gender, number of comorbidities, duration of pain treatment, and number of clinic visits. The results of the multiple logistic regression analysis are shown in .
Table 1 Patients’ Baseline Characteristics
Table 2 The Odds of Opioids Prescription Among Patients with Musculoskeletal Pain
Figure 1 The type and number of opioid analgesic prescriptions for 145 patients.
Discussion
The utilization of opioids in the management of chronic and acute pain has significantly increased worldwide especially in the western countries, such as the United States, where it largely contributed to the current opioid epidemic.Citation18–Citation20 However, there is a lack of studies that explored the predictors for opioids prescription in the management of musculoskeletal pain in the Middle East where the medical practice and the regulations that govern the prescription of opioids are starkly different.Citation21,Citation22 Thus, the findings of this study shed light on the prescribing pattern of opioid analgesics in the management of acute musculoskeletal pain, which is largely unknown in Saudi Arabia. Contrary to what was expected, opioids are not infrequently prescribed in the management of acute pain among the patients in the study. The vast majority of patients seen in the outpatient orthopedic clinics for acute back and lower extremity pain were prescribed opioid analgesics. Patients with lower extremity and back pain have more than 50 times higher odds of receiving opioid analgesics in comparison to their counterparts with shoulder pain despite controlling for a multitude of factors that are known to influence opioids prescription.Citation28 The high utilization rates of opioids in the management of lower extremity and back pain observed in this study are consistent with the reported high opioids utilization rates in the literature.Citation18–Citation20,Citation30 The use of opioids in the management of acute back and lower extremity pain for short term (eg, <90 days) result in greater pain relief according to a moderate level of evidence.Citation17 However, the results of recently published systematic reviews are against the use of opioids for acute and chronic musculoskeletal pain conditions.Citation16 Moreover, the use of opioids in the management of acute and chronic low back pain have not shown to be superior when compared to other non-opioid analgesics.Citation31
On the other hand, shoulder pain was associated with significantly lower odds of opioid prescription. The reasons behind that can be attributable to the increasing evidence that discourage the use of opioids in the management of shoulder pain.Citation32,Citation33 In a retrospective cohort study that examined the impact of opioids use on clinical outcomes among patients who underwent arthroscopic rotator cuff repair, patients who were treated with opioids pre-operatively did not reach the same level of functionality and required higher dosages of opioids post-operatively.Citation33 Additionally, patients with upper extremity pain are believed to require shorter period of opioids treatment in comparison to patients with other types of musculoskeletal pain.Citation34 However, the use of opioids in the management of other types of musculoskeletal pain, such as back pain, is not encouraged either.Citation31 Therefore, it is unclear why patients with back or lower extremity pain were more likely to be treated with opioid analgesics in comparison to their counterparts with shoulder pain despite the fact that the pain severity, as measured by the NPRS, was controlled for. This can be partly explained by the fact that physicians have different beliefs about the consequences of their prescribing decisions, emotionally charged physician–patient interactions, and patients’ and physicians’ characteristics, and preferences.Citation35,Citation36 The severity of pain, as measured by the NPRS, was positively associated with opioids prescribing, which is consistent with the preponderance of evidence.Citation28 However, female gender, age, duration of pain treatment, and number of clinic visits were not associated with opioid prescribing among the sample of patients in this study as shown in the adjusted odds ratios. On another note, tramadol was the most commonly prescribed opioid analgesics. This can be due to the beliefs among some physicians that tramadol is a safe and “opioid-lite”.Citation37 However, the use of tramadol for acute pain is associated with high risk of misuse, adverse effects, and chronic use after an acute pain episode.Citation38
Although this is the first study to the best of our knowledge that explored the predictors for opioids prescribing in Saudi Arabia, it has multiple limitations that must be acknowledged. First, this was a retrospective chart review study that is fraught with information bias, such as documentation and recall bias.Citation39 In addition, this was a single-center study with limited generalizability.Citation40 Furthermore, important variables, such as patient education level, prescribers’ characteristics (eg, education, years of experience, previous history of prescribing opioids), patient satisfaction with care, and patients’ perceptions about the adequacy of pain management, have not been collected and were not controlled for.Citation28 Moreover, not all patients with acute musculoskeletal pain were included in this study although systematic random sampling was used. Despite all of the above-mentioned limitations, this study highlights the gaps in knowledge about opioids prescribing for acute musculoskeletal pain in Saudi Arabia. Although it is largely believed that pain management is inadequate for some patient populations, such as cancer, this might not be the case for patients with acute musculoskeletal pain.Citation24 Future studies should examine the appropriateness and predictors of opioids prescribing in Saudi Arabia for patients with acute and chronic pain at a national level in order to formulate a national policy for opioids prescribing that ensures safe and effective management of pain.
Abbreviations
NPRS, Numeric Pain Rating Scale; DALYs, disability adjusted life-years; EHR, electronic health record.
Data Sharing Statement
Study data are available from the corresponding author (Yazed AlRuthia) upon request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Acknowledgment
The authors acknowledge financial support from Researchers Supporting Project number (RSP-2020/16), King Saud University, Riyadh, Saudi Arabia.
Disclosure
The authors report no conflicts of interest in this work.
References
- World Health Organization. Musculoskeletal conditions. Available from: https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions.
- Ashaye T, Hounsome N, Carnes D, et al. Opioid prescribing for chronic musculoskeletal pain in UK primary care: results from a cohort analysis of the COPERS trial. BMJ Open. 2018;8(6).
- Schnitzer TJ. Update on guidelines for the treatment of chronic musculoskeletal pain. Clin Rheumatol. 2006;25(1):22–29. doi:10.1007/s10067-006-0203-8
- Woolf AD, Akesson K. Understanding the burden of musculoskeletal conditions. BMJ. 2001;322:1079–1080. doi:10.1136/bmj.322.7294.1079
- Hay SI, Abajobir AA, Abate KH, et al. Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1260–1344.
- Jacobson L, Lindgren B. Vad Kostar Sjukdomarna? [What are the Costs of Illness?]. Stockholm: Socialstyrelsen (National Board of Health and Welfare); 1996.
- Punnett L, Wegman DH. Work-related musculoskeletal disorders: the epidemiologic evidence and the debate. J Electromyogr Kinesiol. 2004;14(1):13–23. doi:10.1016/j.jelekin.2003.09.015
- Alghadir A, Anwer S. Prevalence of musculoskeletal pain in construction workers in Saudi Arabia. Sci World J. 2015;2015:529873. doi:10.1155/2015/529873
- Alsultan A, Alahmed S, Alzahrani A, et al. Comparison of musculoskeletal pain prevalence between medical and surgical specialty residents in a major hospital in Riyadh, Saudi Arabia. J Musculoskelet Surg Res. 2018;2(4):161–166. doi:10.4103/jmsr.jmsr_36_18
- Meisha DE, Alsharqawi NS, Samarah AA, et al. Prevalence of work-related musculoskeletal disorders and ergonomic practice among dentists in Jeddah, Saudi Arabia. Clin Cosmet Investig Dent. 2019;11:171–179. doi:10.2147/CCIDE.S204433
- Al-Mohrej OA, AlShaalan NS, Al-Bani WM, et al. Prevalence of musculoskeletal pain of the neck, upper extremities and lower back among dental practitioners working in Riyadh, Saudi Arabia: a cross-sectional study. BMJ Open. 2016;6(6):e011100. doi:10.1136/bmjopen-2016-011100
- Aljanakh M, Shaikh S, Siddiqui AA, et al. Prevalence of musculoskeletal disorders among dentists in the Hail Region of Saudi Arabia. Ann Saudi Med. 2015;35(6):456–461.
- Babatunde OO, Jordan JL, Van der Windt DA, et al. Effective treatment options for musculoskeletal pain in primary care: a systematic overview of current evidence. PLoS One. 2017;12(6):e0178621.
- Vowles KE, McEntee ML, Julnes PS, et al. Rates of opioid misuse, abuse, and addiction in chronic pain: a systematic review and data synthesis. Pain. 2015;156(4):569–576. doi:10.1097/01.j.pain.0000460357.01998.f1
- Hsu JR, Mir H, Wally MK, Seymour RB. Orthopaedic trauma association musculoskeletal pain task force. Clinical practice guidelines for pain management in acute musculoskeletal injury. J Orthop Trauma. 2019;33(5):e158–e182.
- Lin I, Wiles L, Waller R, et al. What does best practice care for musculoskeletal pain look like? Eleven consistent recommendations from high-quality clinical practice guidelines: systematic review. Br J Sports Med. 2020;54(2):79–86. doi:10.1136/bjsports-2018-099878
- Shaheed CA, Maher CG, Williams KA, et al. Efficacy, tolerability, and dose-dependent effects of opioid analgesics for low back pain: a systematic review and meta-analysis. JAMA Intern Med. 2016;176(7):958–968. doi:10.1001/jamainternmed.2016.1251
- Larochelle MR, Zhang F, Ross‐Degnan D, et al. Trends in opioid prescribing and co‐prescribing of sedative hypnotics for acute and chronic musculoskeletal pain: 2001–2010. Pharmacoepidemiol Drug Saf. 2015;24(8):885–892. doi:10.1002/pds.3776
- Bedson J, Chen Y, Hayward RA, et al. Trends in long-term opioid prescribing in primary care patients with musculoskeletal conditions: an observational database study. Pain. 2016;157(7):1525–1531. doi:10.1097/j.pain.0000000000000557
- Blyth FM, Briggs AM, Schneider CH, Hoy DG, March LM. The global burden of musculoskeletal pain-where to from here? Am J Public Health. 2019;109(1):35–40. doi:10.2105/AJPH.2018.304747
- Wilby KJ, Wilbur K. Cross-national analysis of estimated narcotic utilization for twelve Arabic speaking countries in the Middle East. Saudi Pharm J. 2017;25(1):83–87. doi:10.1016/j.jsps.2016.01.001
- Cleary J, Silbermann M, Scholten W, et al. Formulary availability and regulatory barriers to accessibility of opioids for cancer pain in the Middle East: a report from the Global Opioid Policy Initiative (GOPI). Ann Oncol. 2013;24(11):xi51–xi59. doi:10.1093/annonc/mdt503
- Alharbi HA, Albabtain MA, Alobiad N, et al. Pain perception assessment using the short-form McGill pain questionnaire after cardiac surgery. Saudi J Anaesth. 2020;14(3):343–348. doi:10.4103/sja.SJA_34_20
- Al-Rowaili A, Al-Aqeel SA, Al-Naim LS, et al. Appropriateness of cancer pain management in Saudi teaching hospital. Breast. 2009;39(5):37–43.
- Alomi YA. National pharmacy pain management program at ministry of health in Saudi Arabia. J Pharmacol Clin Res. 2017;3(2):1–7. doi:10.19080/JPCR.2017.03.555606
- Bijur PE, Latimer CT, Gallagher EJ. Validation of a verbally administered numerical rating scale of acute pain for use in the emergency department. Acad Emerg Med. 2003;10(4):390–392. doi:10.1197/aemj.10.4.390
- Williams JR. The declaration of Helsinki and public health. Bull World Health Organ. 2008;86:650–652. doi:10.2471/BLT.08.050955
- Simon LS. Relieving pain in America: a blueprint for transforming prevention, care, education, and research. J Pain Palliat Care Pharmacother. 2012;26(2):197–198. doi:10.3109/15360288.2012.678473
- Peduzzi P, Concato J, Kemper E, et al. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49(12):1373–1379. doi:10.1016/S0895-4356(96)00236-3
- Azad TD, Zhang Y, Stienen MN, et al. Patterns of opioid and benzodiazepine use in opioid-naïve patients with newly diagnosed low back and lower extremity pain. J Gen Intern Med. 2020;35(1):291–297. doi:10.1007/s11606-019-05549-8
- Tucker H, Scaff K, McCloud T, et al. Harms and benefits of opioids for management of non-surgical acute and chronic low back pain: a systematic review. Br J Sports Med. 2020;54(11):664. doi:10.1136/bjsports-2018-099805
- Morris BJ, Sciascia AD, Jacobs CA, et al. Preoperative opioid use associated with worse outcomes after anatomic shoulder arthroplasty. J Shoulder Elbow Surg. 2016;25(4):619–623. doi:10.1016/j.jse.2015.09.017
- Williams BT, Redlich NJ, Mickschl DJ, et al. Influence of preoperative opioid use on postoperative outcomes and opioid use after arthroscopic rotator cuff repair. J Shoulder Elbow Surg. 2019;28(3):453–460. doi:10.1016/j.jse.2018.08.036
- Rodgers J, Cunningham K, Fitzgerald K, et al. Opioid consumption following outpatient upper extremity surgery. J Hand Surg Am. 2012;37(4):645–650. doi:10.1016/j.jhsa.2012.01.035
- Heins JK, Heins A, Grammas M, et al. Disparities in analgesia and opioid prescribing practices for patients with musculoskeletal pain in the emergency department. J Emerg Nurs. 2006;32(3):219–224. doi:10.1016/j.jen.2006.01.010
- Desveaux L, Saragosa M, Kithulegoda N, et al. Understanding the behavioural determinants of opioid prescribing among family physicians: a qualitative study. BMC Fam Pract. 2019;20(1):1–12. doi:10.1186/s12875-019-0947-2
- Stannard C. Tramadol is not “opioid-lite”. BMJ. 2019;365:2095. doi:10.1136/bmj.l2095
- Thiels CA, Habermann EB, Hooten WM, et al. Chronic use of tramadol after acute pain episode: cohort study. BMJ. 2019;57(4):595.
- Vassar M, Holzmann M. The retrospective chart review: important methodological considerations. J Educ Eval Health Prof. 2013;10:12. doi:10.3352/jeehp.2013.10.12
- Panacek EA. Performing chart review studies. Air Med J. 2007;26(5):206–210. doi:10.1016/j.amj.2007.06.007