
Abstract
Objective
Fibromyalgia patients frequently report cognitive abnormalities. As the hippocampus plays an important role in learning and memory, we determined whether individuals with fibromyalgia had smaller hippocampal volume compared with healthy control participants.
Methods
T1-weighted structural magnetic resonance imaging (MRI) scans were acquired from 40 female participants with fibromyalgia and 22 female healthy controls. The volume of the hippocampus was estimated using the software FreeSurfer. An analysis of covariance model controlling for potentially confounding factors of age, whole brain size, MRI signal quality, and Beck Depression Inventory scores were used to determine significant group differences.
Results
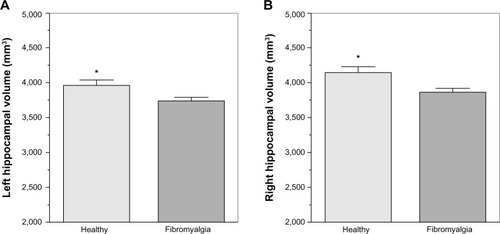
Fibromyalgia participants had significantly smaller hippocampi in both left (F[1,56]=4.55, P=0.037, η2p=0.08) and right hemispheres (F[1,56]=5.89, P=0.019, η2p=0.10). No significant effect of depression was observed in either left or right hemisphere hippocampal volume (P=0.813 and P=0.811, respectively).
Discussion
Potential mechanisms for reduced hippocampal volume in fibromyalgia include abnormal glutamate excitatory neurotransmission and glucocorticoid dysfunction; these factors can lead to neuronal atrophy, through excitotoxicity, and disrupt neurogenesis in the hippocampus. Hippocampal atrophy may play a role in memory and cognitive complaints among fibromyalgia patients.
Keywords:
Introduction
Fibromyalgia (FM) is a disorder characterized by chronic, widespread pain in the muscles, ligaments, tendons, and other connective tissues.Citation1 Approximately five million people in the United States suffer from FM; annual costs of the disease are estimated around $6,000 per person annually.Citation2,Citation3 The exact etiology of FM is unknown;Citation4 however, evidence of abnormalities in brain structure has been reported.Citation5 FM is currently thought of as a complex disorder involving multiple systems, including both peripheral and central nervous system components.
FM patients have been shown to have reductions in cortical gray matter volumes in numerous areas associated with the pain experience, including the insular and anterior cingulate cortices.Citation6–Citation8 However, FM is a disorder characterized by numerous symptoms besides pain, such as sleep disturbance, mood disorders, and cognitive dysfunction. Morphometric changes in FM have been described in areas outside the typically reported cortical “pain regions”, such as reduced gray matter in the amygdala.Citation6,Citation9
Changes to limbic morphometry in regions such as the cingulate, amygdala, thalamus, and the parahippocampal gyrus, have previously been reported in patients with FM.Citation6–Citation10 Although reports of alterations in hippocampal volume among chronic pain conditions are sparse, a pivotal role for the hippocampus in FM has been proposed.Citation11 Using proton magnetic resonance imaging (MRI) spectroscopy, Wood et al found abnormal ratios of N-acetylaspartate to creatine in the right hippocampus of FM patients compared with healthy controls; significant correlations were observed between these abnormalities and FM symptom severity.Citation12 While the cause for such changes is currently unknown, excessive excitatory neurotransmission in the hippocampus may occur in FM, which can lead to potential dysfunction and atrophy.
Hippocampal atrophy resulting from FM may, in turn, worsen or exacerbate FM symptomatology. For example, FM patients often report a subjective worsening of cognitive function characterized by short-term memory problems (ie, the “fibro fog”).Citation13 Furthermore, the hippocampal atrophy and dysfunction may “feed forward”, resulting in more severe pain, discomfort, and anxiety in FM patients, due to its central role in limbic circuits and pain modulation networks.Citation14
While having a strong theoretical backing, conflicting empirical evidence regarding hippocampal volumes in chronic pain conditions exists in the literature. Mutso et alCitation15 found significant bilateral decreases in hippocampal volumes, compared with healthy controls, in complex regional pain syndrome (CRPS) patients and chronic back pain patients but not in osteoarthritis patients. However, Maleki et alCitation16 found no significant reduction in hippocampal volumes among high-frequency migraine patients relative to controls. Zimmerman et alCitation17 reported trend-level (P=0.06) reductions in hippocampal volume in elderly individuals with chronic pain symptoms. While, Lutz et alCitation18 reported highly significant (P<0.001) reductions in bilateral hippocampal volume among FM patients; however, depressive symptomology was not explicitly controlled. Similar reductions in cortical gray matter density have been reported in the parahippocampal gyri among FM patients.Citation7,Citation10
In order to test the hypothesis that FM patients would have decreased hippocampal volume compared with an asymptomatic control sample, an in vivo proxy of hippocampal gray matter volume was used. We also explored whether any reductions in hippocampal volume were related to severity and chronicity of FM symptomology.
Materials and methods
Participants
A total of 22 healthy control (HC) females (mean age =43.43 years) and 40 FM females (mean age =50.17 years) were recruited from the University of Florida and surrounding community through radio, newspaper, and television advertisements. HC participants were excluded if they had a history of painful neuropathies, diabetes, or cancer and/or were currently regularly taking the following medications: nonsteroidal anti-inflammatory drugs (NSAIDs), antidepressants, antihistamines, any analgesics, anticonvulsants, muscle relaxants, or benzodiazepines. FM participants were sourced from a larger clinical trial investigating comorbid FM and insomnia. Inclusion criteria for FM were: a) age 18 years or older; b) individual reports widespread pain; c) FM confirmed by tender point test, using guidelines established by the American College of Rheumatology (with application of 4 kg force, participant reported pain in at least eleven of 18 points, including points in all four body quadrants);Citation19 d) no prescribed or over-the-counter sleep medication for at least 1 month, or stabilized on medication for at least 6 months; and e) able to read and understand English.
Exclusion criteria were: a) sleep disorder other than insomnia (eg, sleep apnea or periodic limb movement disorder), assessed through structured interview and single-night ambulatory monitoring (disqualified if Apnea–Hypopnea Index or myoclonus arousals greater than 15/hour, or between 10–15/hour with oxygen saturation below 88%); b) bipolar disorder or seizure disorder; c) significant medical (eg, cancer) or neurological (eg, dementia) disorder; d) severe untreated psychopathology (eg, schizophrenia, substance abuse); e) cognitive impairment based on a Mini-Mental State Examination score lower than 24 (ninth grade education or higher) or lower than 18 (less than ninth grade education).Citation20 The University of Florida Institutional Review Board approved all study procedures. All participants provided written informed consent prior to any study procedures.
Neuroimaging acquisition
T1-weighted structural MRI scans were acquired from two in-house 3 Tesla (3T) scanners. For FM participants, a Philips Achieva 3.0T 2-Series scanner (Philips Electronics, Amsterdam, The Netherlands) with a Philips eight-channel head coil was used to obtain the structural images. The parameters for each T1-weighted structural scan were set as follows: 180 slices were acquired in the sagittal plane. Fast field echo (FFE) imaging sequence (flip angle [FA] =8°; field of view [FOV] =240 mm ×240 mm ×180 mm; matrix =240 mm ×240 mm; voxel size =1 mm ×1 mm ×1 mm; slice gap =0 mm; actual TR/TE =8.1/3.7 ms) was used. Scans lasted ∼6 minutes (377 seconds). For HC participants, a Siemens MAGNETOM Allegra™ 3.0T scanner (Siemens AG, Munich, Germany) with an eight-channel head coil was used to obtain the structural images. A T1-weighted magnetization-prepared rapid gradient-echo (MP-RAGE) protocol (128 1 mm axial slices; FA =8°; FOV =240 mm; matrix =512 mm ×512 mm; TR =2,000 ms; TE =4.13 ms) was used. The two scanners used for data collection did not differ significantly in anatomic signal-to-noise ratio (SNR) or white matter signal intensity, which are two important factors for quality image segmentation.
Neuroimaging processing
To measure hippocampal volume, the automated subcortical segmentation stream in FreeSurfer V.5.1.0 was used. The software uses Bayesian inference methods relying on prior anatomical probabilities in a labeled data set, along with a priori known T1 intensity characteristics of subcortical regions, as well as T1 intensity information from the scan being processed, in order to label discrete regions.Citation21 Previous research has shown this automated procedure produces accurate and reliable results, while taking a fraction of the time of the gold standard of manual segmentation.Citation21,Citation22 This makes automated segmentation well suited for large samples.
Statistical analyses
Several factors of noninterest to this study, such as participant age, total brain size, and signal quality of MRI, have been shown to be associated with differences in estimated hippocampal volume. Although there were no significant differences in the three aforementioned variables between the FM and healthy controls in our sample, we decided to conservatively control them in our analysis, to minimize variance explained by factors other than differences in clinical condition. Differences in gray matter between FM and healthy individuals have previously been linked to the presence of affective disorders, such as major depression;Citation23 in order to control for these effects, Beck Depression Inventory-II (BDI) scores were included as a covariate in the analysis.Citation24 Missing BDI data for six HC participants were imputed with a random score from the range of HC scores; this method of missing data replacement results in less underestimation of standard errors than mean replacement (“hot deck imputation”).Citation25 In addition to controlling for BDI, the main effect of BDI scores on hippocampal volume was explored to examine the possible differential effects of depression and FM.
Two analyses of covariance (ANCOVAs) were run using SPSS v20, with dependent measures of left and right hippocampal volume respectively, a fixed factor of diagnosis, and covariates of BDI, age, whole brain gray matter volume, and anatomic SNR. Whole brain gray matter volume was used as a proxy for brain size, instead of intracranial volume, because whole brain gray matter volume had a stronger relationship to hippocampal volume in our sample (r=0.636 for whole brain gray matter and hippocampal volume relationship compared with r=0.12 for total intracranial volume and hippocampal volume relationship).
In order to examine the relationship between FM symptomology severity and hippocampal volume, measures of self-reported sleep quality (ratio of total sleep time to total time in bed, as reported in daily sleep diaries) and Pain Disability Index questionnaireCitation26 scores were correlated with hippocampal volume. Measures of sleep quality and pain disability were not collected in the HC sample due to the data being sourced from separate studies. To examine the relationship between FM chronicity and hippocampal volume, normalized symptom duration (years since symptom onset/participant’s age) was correlated with hippocampal volume. Symptom duration was not compared in HC participants, as it is not applicable. All correlation tests were conducted using semipartial correlations that controlled for the effects of age, total gray matter volume, SNR, and BDI on hippocampal volume, while leaving dependent variables unadjusted.Citation27
Results
Demographics
Participants’ demographic information is presented in .
Table 1 Demographic information
Main effect of group
ANCOVA indicated FM participants had significantly smaller hippocampi in both left (F[1,56]=4.55, P=0.037) and right hemispheres (F[1,56]=5.89, P=0.019). Larger volume differences were observed in the right hippocampus (η2p=0.095) compared with the left hippocampus (η2p=0.075) ().
Figure 1 Estimated left (A) and right (B) hippocampal volume for fibromyalgia and healthy control groups.
Depressive symptomatology
As anticipated, significant differences in depression level were observed between FM and HC groups, with FM participants having higher BDI scores (t[60]=6.58, P<0.001, Cohen’s d=1.52). However, no significant effect of BDI on hippocampal volume was observed in either hemisphere (left hemisphere: F[1,56]=0.06, P=0.813; right hemisphere: F[1,56]=0.06, P=0.811).
Sleep efficiency and hippocampal volume
No significant relationships were observed between sleep efficiency and hippocampal volume, in either hemisphere in FM participants, using Pearson correlations (left hemisphere: r=0.05, P=0.796; right hemisphere r=0.17, P=0.337).
Pain disability and hippocampal volume
No significant relationships were observed between Pain Disability Index scores and hippocampal volume, in either hemisphere in FM participants, using Pearson correlations (left hemisphere: r=−0.17, P=0.351; right hemisphere r=−0.05, P=0.788).
FM chronicity and hippocampal volume
No significant relationships were observed between FM chronicity and hippocampal volume, using Pearson correlations (left hemisphere: r=0.23, P=0.187; right hemisphere r=0.22, P=0.209).
Discussion
While controlling for potentially confounding factors, participants with FM showed reduced hippocampal volume bilaterally. These findings are in line with previous research showing reduced hippocampal volumes in FM.Citation18 However, to the authors’ knowledge, this is the first report describing reduced hippocampal volumes in FM while explicitly controlling for comorbid depression. Although patients with FM have increased incidence of depression and patients with major depressive disorder have been shown to have smaller hippocampi,Citation28 we did not find a significant main effect of depression in our study.
No relationships between FM chronicity, sleep efficiency, or Pain Disability Index and hippocampal volume were observed in our sample. Kuchinad et alCitation7 have described a significant relationship between duration of FM and gray matter deficits. However, other authors have reported no such relationship.Citation10,Citation29 Heterogeneity among modestly sized samples, discrepancy in how chronicity is defined (ie, years since symptom onset or years since diagnosis of FM), and inaccurate recall of events that are sometimes decades in the past may explain some of the inconsistency in the literature. Furthermore, we hypothesized participants with more severe symptoms (ie, lower quality and quantity of sleep and greater disability from pain) would show greater reductions in hippocampal volume. However, no such relationship was apparent. It is possible that symptom severity along other dimensions (ie, memory and cognitive function) may be more associated with hippocampal volume, due to the extensive role of the hippocampus in memory and cognition.
Potential mechanisms for hippocampal atrophy
Mechanisms of hippocampal atrophy in FM patients need to be explored further. One potential mechanism includes a dysfunctional balance between excitatory glutamate and inhibitory gamma-aminobutyric acid (GABA) neurotransmission. FM patients have been shown to have elevated levels of excitatory amino acids, such as glutamate.Citation30 Clauw et alCitation30 posited that abnormally high glutamate neurotransmission is associated with hyperalgesia and allodynia. Drugs that attempt to restore the balance between excitatory and inhibitory neurotransmission, via combinations of N-methyl-D-aspartate (NMDA) glutamate antagonism and GABA agonism, have been tested for efficacy in FM (for eg, sodium oxybate and ketamine).Citation31,Citation32 Restoring the balance in inhibitory/excitatory neurotransmission appears crucial in limiting hippocampal atrophy, as NMDA excitotoxicity is a prominent factor in animal models of hippocampal neuronal death.Citation33
Prolonged or traumatic stress represents another potential mechanism for hippocampal volume deficits in FM. Clinically FM often presents after a biological stressor, such as infection, or a psychosocial stressor, such as a major life event, or combinations of both.Citation34 FM patients have been found to have abnormalities in endogenous glucocorticoid and hypothalamic-pituitary-adrenal axis function, two important mediators of the biological stress response.Citation35,Citation36 Prolonged stress has been associated with hippocampal atrophy in animal models as well as human neuroimaging studies of posttraumatic stress disorder patients.Citation37,Citation38 Some authors have suggested hippocampal volume deficits are a predisposing factor to maladaptive stress response,Citation39 while others posit hippocampal atrophy is a consequence of prolonged or traumatic stress.Citation40
Limitations and future directions
Longitudinal studies are needed to clarify the time course of hippocampal atrophy; due to the cross-sectional nature of this study it is unknown whether hippocampal abnormalities precede FM, are a consequence of the disorder, or both. Furthermore, potential neuroplasticity of the hippocampus resulting from treatment is an unknown and exciting area for future research. Experimental designs that manipulate potential mechanisms of hippocampal atrophy (such as behavioral interventions promoting healthy stress responses or pharmacologic interventions targeting potentially excessive glutamatergic neurotransmission) in a FM sample would provide the evidence needed for causal inference. Additionally, technological advances in the acquisition and processing of neuroimaging data may provide new insights (for example, the subdivision of hippocampal structures into functionally distinct subfields, using high resolution structural MRI).Citation41
Conclusion
FM participants show reduced hippocampal volumes when compared with sex-matched healthy controls. These volumetric deficits were not explained by differences in age, duration of illness, total brain size, or depressive symptomology. Further research on hippocampal structure and function in fibromyalgia is justified.
Acknowledgments
The project described was supported by award numbers R01AR055160 and R01AR055160-S1 American Recovery and Reinvestment Act Supplement from the National Institute of Arthritis and Musculoskeletal and Skin Diseases.
Disclosure
The authors report no conflicts of interest in this work.
References
- McBethJMulveyMRFibromyalgia: mechanisms and potential impact of the ACR 2010 classification criteriaNat Rev Rheumatol20128210811622270077
- LawrenceRCFelsonDTHelmickCGNational Arthritis Data WorkgroupEstimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part IIArthritis Rheum2008581263518163497
- WolfeFAndersonJHarknessDA prospective, longitudinal, multicenter study of service utilization and costs in fibromyalgiaArthritis Rheum1997409156015709324009
- GormsenLRosenbergRBachFWJensenTSDepression, anxiety, health-related quality of life and pain in patients with chronic fibromyalgia and neuropathic painEur J Pain2010142127. e1127. e819473857
- SchweinhardtPSauroKMBushnellMCFibromyalgia: a disorder of the brain?Neuroscientist200814541542118270311
- BurgmerMGaubitzMKonradCDecreased gray matter volumes in the cingulo-frontal cortex and the amygdala in patients with fibromyalgiaPsychosom Med200971556657319414621
- KuchinadASchweinhardtPSeminowiczDAWoodPBChizhBABushnellMCAccelerated brain gray matter loss in fibromyalgia patients: premature aging of the brain?J Neurosci200727154004400717428976
- RobinsonMECraggsJGPriceDDPerlsteinWMStaudRGray matter volumes of pain-related brain areas are decreased in fibromyalgia syndromeJ Pain201112443644321146463
- JensenKBSrinivasanPSpaethROverlapping structural and functional brain changes in patients with long-term exposure to fibromyalgia painArthritis Rheum201365123293330323982850
- WoodPBGlabusMFSimpsonRPattersonJCChanges in gray matter density in fibromyalgia: correlation with dopamine metabolismJ Pain200910660961819398377
- WoodPBFibromyalgia syndrome: a central role for the hippocampus–A theoretical constructJ Musculoskeletal Pain20041211926
- WoodPBLedbetterCRGlabusMFBroadwellLKPattersonJCHippocampal metabolite abnormalities in fibromyalgia: correlation with clinical featuresJ Pain2009101475218771960
- AmbroseKRGracelyRHGlassJMFibromyalgia dyscognition: concepts and issuesReumatismo201264420621523024965
- PloghausANarainCBeckmannCFExacerbation of pain by anxiety is associated with activity in a hippocampal networkJ Neurosci200121249896990311739597
- MutsoAARadzickiDBalikiMNAbnormalities in hippocampal functioning with persistent painJ Neurosci201232175747575622539837
- MalekiNBecerraLBrawnJMcEwenBBursteinRBorsookDCommon hippocampal structural and functional changes in migraineBrain Struct Funct2013218490391222760159
- ZimmermanMEPanJWHetheringtonHPLiptonMLBaigiKLiptonRBHippocampal correlates of pain in healthy elderly adults: a pilot studyNeurology200973191567157019901248
- LutzJJägerLde QuervainDWhite and gray matter abnormalities in the brain of patients with fibromyalgia: a diffusion-tensor and volumetric imaging studyArthritis Rheum200858123960396919035484
- WolfeFSmytheHAYunusMBThe American College of Rheumatology 1990 criteria for the classification of fibromyalgia. Report of the Multicenter Criteria CommitteeArthritis Rheum19903321601722306288
- MurdenRAMcRaeTDKanerSBucknamMEMini-Mental State Exam scores vary with education in blacks and whitesJ Am Geriatr Soc19913921491551991947
- FischlBSalatDHBusaEWhole brain segmentation: automated labeling of neuroanatomical structures in the human brainNeuron200233334135511832223
- JovicichJCzannerSHanXMRI-derived measurements of human subcortical, ventricular and intracranial brain volumes: Reliability effects of scan sessions, acquisition sequences, data analyses, scanner upgrade, scanner vendors and field strengthsNeuroimage200946117719219233293
- HsuMCHarrisRESundgrenPCNo consistent difference in gray matter volume between individuals with fibromyalgia and age-matched healthy subjects when controlling for affective disorderPain2009143326226719375224
- BeckATSteerRABallRRanieriWComparison of Beck Depression Inventories-IA and -II in psychiatric outpatientsJ Pers Assess19966735885978991972
- AndridgeRRLittleRJA review of hot deck imputation for survey non-responseInt Stat Rev2010781406421743766
- TaitRCPollardCAMargolisRBDuckroPNKrauseSJThe Pain Disability Index – psychometric and validity dataArch Phys Med Rehab1987687438441
- FieldADiscovering Statistics Using SPSS3rd edLondonSage Publications2009
- MacQueenGMCampbellSMcEwenBSCourse of illness, hippocampal function, and hippocampal volume in major depressionProc Natl Acad Sci U S A200310031387139212552118
- Schmidt-WilckeTLuerdingRWeigandTStriatal grey matter increase in patients suffering from fibromyalgia – a voxel-based morphometry studyPain2007132Suppl 1S109S11617587497
- ClauwDJArnoldLMMcCarbergBHFibroCollaborativeThe science of fibromyalgiaMayo Clin Proc201186990791121878603
- RussellIJHolmanAJSwickTJAlvarez-HorineSWangYGGuintaDSodium Oxybate 06-008 FM Study GroupSodium oxybate reduces pain, fatigue, and sleep disturbance and improves functionality in fibromyalgia: results from a 14-week, randomized, double-blind, placebo-controlled studyPain201115251007101721397402
- Graven-NielsenTAspegren KendallSHenrikssonKGKetamine reduces muscle pain, temporal summation, and referred pain in fibromyalgia patientsPain200085348349110781923
- McEwenBSPossible mechanisms for atrophy of the human hippocampusMol Psychiatr199723255262
- Van HoudenhoveBEgleUTFibromyalgia: a stress disorder? Piecing the biopsychosocial puzzle togetherPsychother Psychosom200473526727515292624
- GriepENBoersmaJWde KloetERAltered reactivity of the hypothalamic-pituitary-adrenal axis in the primary fibromyalgia syndromeJ Rheumatol19932034694748386766
- AdlerGKKinsleyBTHurwitzSMosseyCJGoldenbergDLReduced hypothalamic-pituitary and sympathoadrenal responses to hypoglycemia in women with fibromyalgia syndromeAm J Med1999106553454310335725
- McEwenBSStress and hippocampal plasticityAnnu Rev Neurosci19992210512210202533
- BremnerJDRandallPScottTMMRI-based measurement of hippocampal volume in patients with combat-related posttraumatic stress disorderAm J Psychiatry199515279739817793467
- GilbertsonMWShentonMECiszewskiASmaller hippocampal volume predicts pathologic vulnerability to psychological traumaNat Neurosci20025111242124712379862
- LeeTJaromeTLiSJKimJJHelmstetterFJChronic stress selectively reduces hippocampal volume in rats: a longitudinal magnetic resonance imaging studyNeuroreport200920171554155819858767
- Van LeemputKBakkourABennerTAutomated segmentation of hippocampal subfields from ultra-high resolution in vivo MRIHippocampus200919654955719405131