
Abstract
Introduction:
Parkinson’s disease (PD) is associated with slowness of movement and balance disturbance. Anxiety and social isolation are common and quality of life (QoL) can be compromised. Dancing enables people with PD to participate in an enjoyable form of exercise within a group. This review provides an updated synthesis of the literature comparing dance to other interventions in people with PD.
Methods:
Six databases were electronically searched. Relevant articles were identified using inclusion criteria. Data on participants, the dance intervention, and outcomes were extracted from suitable articles.
Results:
Methodological limitations were evident in 13 included articles. The evidence reviewed suggests that dancing is enjoyable and can improve balance, motor function, and QoL. Further research is needed to determine the effect of dancing on cognition and depression in this population. Longer term dance interventions may be needed to achieve more meaningful benefits in mobility.
Conclusion:
Dancing can be a feasible and beneficial physical activity and improve the wellness of individuals with PD.
Keywords::
Introduction
Parkinson’s disease (PD) is common, affecting at least 7 million people worldwide.Citation1 With disease progression, people can experience movement difficultiesCitation2 and problems participating in socialCitation3 and family lifeCitation4 and physical activities.Citation5 Movement disorders associated with PD together with insufficient exercise can compromise balance and gait, contributing to further inactivity,Citation6 falls,Citation7 isolation, and loss of independence.Citation8 Although the benefits of exercise are well-recognized for people with PD,Citation9,Citation10 sedentary lifestyles remain common and can be debilitating.Citation11
Therapeutic dancing has become popular for people with Parkinson’s.Citation12,Citation13 It is purported to offer an enjoyable and social setting for physical activity in addition to boosting exercise motivation,Citation14,Citation15 social interaction, and emotional well-being. Previous reviews have shown that some forms of dance can improve balance,Citation16 motor function,Citation17 and quality of life (QoL)Citation12 in people with mild to moderately severe PD. More recently, a resurgence of new studies has been published and offers new insight into the benefits of dance for people with PD. There is a need to provide an updated synthesis of the multidimensional benefits of dance for people with PD compared to other interventions or a control. This may enable evidence based practice and help clinicians and/or dance therapists to justify their treatment decisions and offer the most beneficial therapies to patients.
The aim of this systematic review is to provide an updated 1) synthesis and critique of the literature on dance for people with PD and 2) review of the physical and non-motor benefits of dance for people with PD compared to other interventions and/or control groups.
Methods
The methods of this review conform with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.Citation18
Inclusion criteria
Peer-reviewed published articles were included if they evaluated the benefit of a dance program for people with PD. There was no restriction on the stage of PD, described using the Hoehn and Yahr or modified Hoehn and Yahr scale. Studies must have been written in English, included more than one participant, and reported at least one of the outcomes of interest using a quantitative approach. Only study designs involving two or more arms were eligible for inclusion. Review articles and qualitative studies were not included in this review.
Literature search
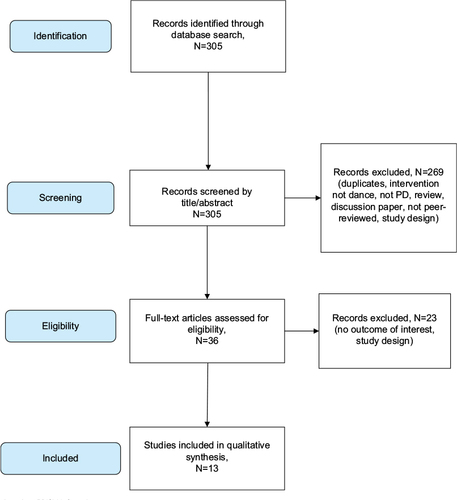
EBSCO was used to electronically search Academic Search Complete, AMED, MEDLINE, and CINAHL Plus, in 2017. ScienceDirect and Pubmed Central were also searched. Databases were searched by title/abstract. The search terms used were “Parkinson OR Parkinson’s” AND “dance OR dancing OR dancers”. One reviewer (JS) screened the retrieved articles by title/abstract and those unrelated were excluded. The remaining full-text articles were read and two reviewers determined their suitability for inclusion (JS and AMC). Any discrepancies between the reviewers were resolved through discussion. An overview of the search process is shown in .
Figure 1 Search strategy based on PRISMA flow diagram.
Data extraction
The following data were extracted from eligible articles:
Characteristics of participants (number of participants, age, stage of disease).
Characteristics of the intervention (dosage, therapy offered, attendance, satisfaction, adverse events, dropouts).
Outcomes of interest.
Results: the results of both intragroup (the difference between pre- and post-assessment results within each study group) and intergroup comparisons (the difference between the study groups after the intervention) were extracted. In line with the aim of this review, data on both types of comparisons were included in order to 1) identify the aspects of health improved by dance participation and 2) ascertain if dancing may be equally or more beneficial than other therapies or a control.
Methodological features.
Outcomes of interest
The lives of people with PD are often negatively affected by physical and non-motor symptoms associated with the condition. Therefore, the outcomes of interest and measurement tools listed in were chosen for this review.
Table 1 Outcomes and measurement tools of interest
Only data from one measurement tool were extracted per outcome. If an outcome was assessed using two or more tools, data from the measurement tool of interest () were prioritized. Outcomes of interest assessed using tools not mentioned in were considered for review. If an outcome was assessed with two or more tools not detailed in , data regarding the first tool listed in the study were extracted.
Quality assessment
The design of each study was defined using the Cochrane Handbook of Systematic Reviews of Interventions.Citation28 The quality of randomized controlled trials (RCTs), quasi-RCTs, stratified RCTs, and non-RCTs was appraised using the PEDro scale.Citation29,Citation30 This scale has been used in previous systematic reviews.Citation9,Citation12 The quality of controlled before and after studies and case-controlled studies was critiqued using a checklist developed by Lötzke et al.Citation13 This tool provides a list of criteria for evaluating the quality of various study designs and has been used in previous reviews of dance interventions for people with PD.Citation13
Data synthesis
The information extracted from the included articles was synthesized qualitatively. Due to the high level of clinical heterogeneity in the studies, quantitative analysis was not recommended.
Results
The search strategy retrieved 305 articles and 13 were eligible for inclusion (). The included articles consisted of one quasi-RCT,Citation31 one case-controlled study,Citation32 one controlled before and after study,Citation33 two non-RCTs,Citation34,Citation35 one stratified RCT,Citation36 and seven RCTs.Citation37–Citation43
displays the characteristics of the included studies. The collective sample size across the studies was 533 participants and the average age of participants ranged from 57.90 to 72.6 years.Citation35,Citation40 There were 138 dropouts across all studies. Some of the reasons for dropping out of dance classes included fatigue,Citation39 changes in health status,Citation39,Citation41–Citation43 fractures,Citation31 knee pain,Citation37,Citation38 leg injury outside of class,Citation32 family reasons,Citation32,Citation38,Citation42 desire not to continue,Citation39,Citation41 and travel or schedule difficulties.Citation38,Citation39,Citation41,Citation42 Two studies did not state the reasons for dropout and the number of dropouts per group.Citation34,Citation35 Over 50% of studies failed to state if they monitored for adverse events.
Table 2 Characteristics of included studies
The benefit of seven dance genres was investigated. Two studies compared dance with traditional therapy approaches,Citation34,Citation36 one compared dance to usual medical care,Citation42 another compared dance to Tai Chi,Citation37 three studies compared different forms of dance,Citation32,Citation38,Citation39 three other studies compared dance to exercise,Citation31,Citation40,Citation43 and six studies compared dance with no intervention. Participants in the traditional therapy and exercise interventions performed exercises to improve strength, flexibility, range of motion, mobility, balance, and motor coordination. Cueing was also used in two studies as part of the intervention.Citation34,Citation36 The dance interventions were well-described in 10 studies.Citation35,Citation40,Citation41 Seven studies stated that a warm-up was performed at the start of classCitation31–Citation34,Citation36,Citation39,Citation42 and nine studies used dance instructors with previous experience.Citation31,Citation33,Citation36–Citation40,Citation42,Citation43 Two studies included a home dance program as part of the dance intervention.Citation36,Citation42
The volume of dance activity in each study and the results of intragroup (the difference between pre- and post-assessment results within each study group) and intergroup comparisons (the difference between the study groups after the intervention) are summarized in and . Where possible, the results of intragroup comparisons were presented quantitatively. If the required raw data were not provided in the original article, the results were described qualitatively.
Table 3 Intervention design and results of intragroup comparisons
Table 4 Results of intergroup comparisons
The results of the quality appraisal for RCT and non-RCTs are presented in . No study fulfilled the criteria for blind therapists and subjects. Five studies scored 7/10 indicating good methodological quality. One study scored 2/10 indicating major methodological flaws. The case-controlled trial and controlled before and after study fulfilled the majority of criteria in the checklist as shown in .
Table 5 Methodological quality of included randomized and non-randomized trials
Table 6 Methodological quality of controlled before and after and case-controlled studies
Discussion
The results of this review inform clinicians and dance therapists about the potential benefits of dancing compared to other therapies and will help therapists to treat and advice patients considering dancing as an exercise hobby.
Promoting well-being and physical activity are key priorities for clinicians treating individuals with PD.Citation44 Nevertheless, physical inactivity remains commonCitation11,Citation45 and may negatively impact mood, balance, and gait.Citation6 The evidence in this review indicates that dancing is enjoyable and can motive regular participation. The group settingCitation46 of dance along with the various stylesCitation47 and musicCitation48 may create positive emotional responses and encourage weekly participation. Whether or not people with PD will continue dancing over prolonged periods of time requires further research.
Physical benefits
The results of this review suggest that dancing can improve balance and motor function. With respect to balance, all studies except oneCitation42 reported improvements following the intervention. In the majority of studies, gains >2.84 points were evident on the Berg balance scale. Previous research suggests that this magnitude of improvement could be functionally significant for people with PDCitation49 and make the completion of everyday tasks easier. Clinically meaningful changes seem more difficult to achieve on the mini-BESTest, particularly in the short term. This suggests that some dance programs may not effectively target all the aspects of postural control assessed in the mini-BESTest.Citation20 Future studies should carefully plan the content of the intervention and ensure that the material safely challenges all aspects of balance control.
The dosage of dance may influence balance performance. The longest duration interventions noted the largest improvements in balance.Citation36,Citation41 This is consistent with the American College of Sports Medicine exercise recommendations which advise long-term exercise participation to optimize health benefits.Citation50 An insufficient dosage of dance, due to low compliance with the home program, may explain the lack of balance improvement found by Shanahan et al.Citation42 From the evidence reviewed, it is obvious that ~20 hours of dancing within 10–13 weeks may be needed to improve balance.
There is preliminary evidence to suggest that dance can improve motor function. Dance participants achieved gains that surpassed the minimal clinically important difference for the unified PD rating scale motor sectionCitation51 and Movement Disorders Society unified PD rating scale motor sectionCitation52 in six studies (). Compared to nondance interventions, dancers achieved better motor performance following the intervention and the difference between groups was statistically significant in two studies.Citation36,Citation41 There is insufficient evidence to indicate that some dance forms are more effective than others for improving motor function; however, further research is warranted. This would identify dance genres that preferentially target certain symptoms and help individualize the referral process to classes.
Although evidence suggests that dance can improve mobility, the results reported in studies demonstrated lower than the minimal detectable change for the timed up and go test for people with PD.Citation19 Previous research on physiotherapy interventions in this population reported similar results.Citation53 In the current review, the duration of the interventions may explain the lack of substantial improvement in mobility. Many of the included studies involved short durations and the progressive nature of PD could make it harder to achieve mobility gains within this time frame. At present, there is a paucity of evidence examining the long-term benefit of dance on mobility in people with PD and future studies are needed. Notably, the dance interventions were sufficient to maintain mobility and this was significantly better than comparison therapies in some studies.Citation34,Citation36,Citation43 This could be very meaningful for patients function.Citation54 Qualitative research studies are warranted to ascertain the perceived benefits of dancing and determine if dancing positively impacts the everyday lives of people with PD.
Non-motor benefits
At present, there is insufficient evidence to suggest that dance can improve cognitive performance and depression in people with PD. Only one study reported significant cognitive and mood improvements following dance participation.Citation31 The improvements noted in other studies that assessed these outcomes were small and may be clinically insufficient. Notably, no study in this review reported negative mood or cognitive effects of dancing. In individuals without PD, research has found that participation in partnered dance styles is associated with perceived cognitive, social, and emotional health benefits.Citation55 The combination of motor skill learning, exercise, socialization, and music is hypothesized to improve mood and cognitionCitation14 and further research is recommended in people with PD.
Fatigue affects over 50% of people with PD and is perceived to be one of the most deliberating symptoms of this condition.Citation56 Music accompaniment in dance may help combat fatigue by activating brain areas such as the amygdala and cingulate cortex and stimulating dopamine.Citation48 Only one included study examined the impact of dance on fatigue.Citation43 While the results of this study were positive, more research is warranted to determine if dancing can help people with PD manage this deliberating symptom.
In comparison with nondance groups, QoL improved more in dance participants. Although one study reported contrary results, the clinical meaningfulness of this finding is unclear.Citation43 Further research will help ascertain the optimum styles of dance to improve QoL.
No relationship between the dosage of dance and the magnitude of improvement in QoL was evident from the literature reviewed. It is possible that other factors such as the environment created at the dance classes may have a greater influence. Previous research indicates that people with PD are most comfortable when dance classes foster a relaxed social and learning environment and are led by a patient teacher who has the skills necessary to adapt dances for each individual.Citation57,Citation58 Importantly, these factors may influence the joy experienced at dance classes and subsequently effect QoL. A sense of satisfaction and perceived benefit in QoL may be important to enhance continual participation,Citation59 create positive attitudes toward exercise, and improve well-being. The social context of dance may be particularly pertinent to build social networks, friendships, and social connectedness;Citation3 however, this needs to be assessed in future studies. In conclusion, it is important that studies consider the effect of environmental factors on health and participation outcomes and implement strategies to overcome any challenges encountered.
Limitations
The limitations of this review must be considered when interpreting the results. Many of the included studies were small. This limits the clinical transferability of the results. Four studies were non-randomized and therefore have an increased risk of bias.Citation32–Citation35 The majority of RCTs and non-randomized studies have an increased risk of selection bias.Citation34,Citation35,Citation37–Citation41,Citation43 Comparability between the groups at baseline was also lacking in four studies.Citation31,Citation35,Citation37,Citation43 Reporting and monitoring of adverse events were insufficient in the literature (). This presents a challenge when clinicians need to establish the suitability of dance interventions for people with PD. Future research should consider these limitations and design study protocols that limit their occurrence.
There were a number of dropouts in the included studies. Collectively, the dropout rate was nearly 26%. This is higher than that reported in some other interventionsCitation60 and makes it difficult for clinicians to determine the feasibility of dance therapy. The reason for the higher dropout rate reported in this review is unclear. However, many of the reasons for dropping out are modifiable and need to be considered in future studies. Additionally, many people have experiences of danceCitation47 and it is plausible that the dancing organized as part of research afforded different experiences and discouraged participation. Dance is not just an exercise. It is a form of artistic expression that captures social and emotional experiences.Citation58 Collaboration between people with PD and arts and health therapists may help identify the desired elements of dance classes and improve the retention rates in studies.
Conclusion
Dancing can be a valuable and enjoyable activity for people with PD. Dance may benefit balance, motor function, and QoL compared to some other forms of therapy. Further research is needed to examine if dancing can improve mobility and non-motor symptoms in people with PD.
Disclosure
This manuscript entitled “Dancing and Parkinson’s disease: updates on this creative approach to therapy” has not been published previously and is not under consideration by another journal. The authors report no conflicts of interest in this work.
References
- Morris ME, Martin C, McGinley JL, et al. Protocol for a home-based integrated physical therapy program to reduce falls and improve mobility in people with Parkinson’s disease. BMC Neurol. 2012;12:54.
- Shulman LM, Gruber-Baldini AL, Anderson KE, Vaughan CG, Reich SG, Fishman PS. The evolution of disability in Parkinson disease. Mov Disord. 2008;23(6):790–796.
- Soleimani MA, Negarandeh R, Bastani F, Greysen R. Disrupted social connectedness in people with Parkinson’s disease. Br J Community Nurs. 2014;19(3):136–141.
- Soundy A, Stubbs B, Roskell C. The experience of Parkinson’s disease: a systematic review and meta-ethnography. Scientific World J. 2014;2014:19.
- van Nimwegen M, Speelman AD, Hofman-van Rossum EJ, et al. Physical inactivity in Parkinson’s disease. J Neurol. 2011;258(12):2214–2221.
- Speelman AD, van de Warrenburg BP, van Nimwegen M, Petzinger GM, Munneke M, Bloem BR. How might physical activity benefit patients with Parkinson disease? Nat Rev Neurol. 2011;7(9):528–534.
- Morris ME, Taylor NF, Watts JJ, et al. A home program of strength training, movement strategy training and education did not prevent falls in people with Parkinson’s disease: a randomised trial. J Physiother. 2017;63(2):94–100.
- Tan DM, McGinley JL, Danoudis ME, Iansek R, Morris ME. Freezing of gait and activity limitations in people with Parkinson’s disease. Arch Phys Med Rehabil. 2011;92(7):1159–1165.
- Shu H-F, Yang T, Yu S-X, et al. Aerobic exercise for Parkinson’s disease: a systematic review and meta-analysis of randomized controlled trials. PLoS One. 2014;9(7):e100503.
- Wu P-L, Lee M, Huang T-T. Effectiveness of physical activity on patients with depression and Parkinson’s disease: a systematic review. PLoS One. 2017;12(7):e0181515.
- Benka Wallén M, Franzén E, Nero H, Hagströmer M. Levels and patterns of physical activity and sedentary behavior in elderly people with mild to moderate Parkinson disease. Phys Ther. 2015;95(8):1135–1141.
- Aguiar L, Morris ME. Therapeutic dancing for Parkinson’s disease. Int J Gerontol. 2016;10(2):64–70.
- Lötzke D, Ostermann T, Büssing A. Argentine tango in Parkinson disease – a systematic review and meta-analysis. BMC Neurol. 2015; 15:226.
- Dhami P, Moreno S, DeSouza JFX. New framework for rehabilitation – fusion of cognitive and physical rehabilitation: the hope for dancing. Front Psychol. 2015;5:1478.
- Earhart GM. Dance as therapy for individuals with Parkinson disease. Eur J Phys Rehabil Med. 2009;45(2):231–238.
- Rocha PA, McClelland J, Morris ME. Complementary physical therapies for movement disorders in Parkinson’s disease: a systematic review. Eur J Phys Rehabil Med. 2015;51(6):693–704.
- Shanahan J, Morris ME, Bhriain ON, Saunders J, Clifford AM. Dance for people with Parkinson disease: what is the evidence telling us? Arch Phys Med Rehabil. 2015;96(1):141–153.
- Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097.
- Steffen T, Seney M. Test-retest reliability and minimal detectable change on balance and ambulation tests, the 36-item short-form health survey, and the unified Parkinson disease rating scale in people with parkinsonism. Phys Ther. 2008;88(6):733–746.
- Leddy AL, Crowner BE, Earhart GM. Utility of the Mini-BESTest, BESTest, and BESTest sections for balance assessments in individuals with Parkinson disease. J Neurol Phy Ther. 2011;35(2):90–97.
- Fahn S, Elton RL, Members UP. Unified Parkinson’s disease rating scale. In: Fahn S, Marsden CD, Calne D, Goldstein M, editors. Recent Developments in Parkinson’s Disease. Volume 2. Florham Park, NJ: McMillan Healthcare Information; 1987.
- Goetz CG, Tilley BC, Shaftman SR, Stebbins GT, Fahn S, Martinez-Martin P. Movement Disorder Society-sponsored revision of the unified Parkinson’s disease rating scale (MDS-UPDRS): scale presentation and clinimetric testing results. Mov Disord. 2008;23(15):2129–2170.
- Morris S, Morris ME, Iansek R. Reliability of measurements obtained with the timed “up & go” test in people with Parkinson disease. Phys Ther. 2001;81(2):810–818.
- Schrag A, Barone P, Brown RG, et al. Depression rating scales in Parkinson’s disease: critique and recommendations. Mov Disord. 2007;22(8):1077–1092.
- Nazem S, Siderowf AD, Duda JE, et al. Montreal cognitive assessment performance in patients with Parkinson’s disease with “normal” global cognition according to mini-mental state examination score. J Am Geriatr Soc. 2009;57(2):304–308.
- Jenkinson C, Fitzpatrick R, Peto V, Greenhall R, Hyman N. The Parkinson’s disease questionnaire (PDQ-39): development and validation of a Parkinson’s disease summary index score. Age Ageing. 1997;26(5):353–357.
- Grace J, Mendelsohn A, Friedman JH. A comparison of fatigue measures in Parkinson’s disease. Parkinsonism Relat Disord. 2007;13(7):443–445.
- Reeves BC, Deeks JJ, Higgins JP, Wells GA. Including non-randomized studies. In: Higgins JP, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions. Volume 5.0.1 (updated March 2011). Cochrane Collaboration: John Wiley & Sons Ltd; 2011: 13.1–13.2. Available from: www.handbook.cochrane.org. Accessed April 1, 2017.
- Sherrington C, Herbert RD, Maher CG, Moseley AM. PEDro. A database of randomized trials and systematic reviews in physiotherapy. Man Ther. 2000;5(4):223–226.
- Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. 2003;83(8):713–721.
- Hashimoto H, Takabatake S, Miyaguchi H, Nakanishi H, Naitou Y. Effects of dance on motor functions, cognitive functions, and mental symptoms of Parkinson’s disease: a quasi-randomized pilot trial. Complement Ther Med. 2015;23(2):210–219.
- McNeely ME, Mai MM, Duncan RP, Earhart GM. Differential effects of tango versus dance for PD in Parkinson disease. Front Aging Neurosci. 2015;7:239.
- Ventura MI, Barnes DE, Ross JM, Lanni KE, Sigvardt KA, Disbrow EA. A pilot study to evaluate multi-dimensional effects of dance for people with Parkinson’s disease. Contemp Clin Trials. 2016;51:50–55.
- de Natale E, Paulus K, Aiello E, Sanna B. Dance therapy improves motor and cognitive functions in patients with Parkinson’s disease. NeuroRehabilitation. 2017;40(1):141–144.
- Lukšys D, Griškevičius G. Quantitative assessment of dance therapy influence on the Parkinson’s disease patients’ lower limb biomechanics. Mokslas – Lietuvos Ateitis. 2016;8(6):583–586.
- Volpe D, Signorini M, Marchetto A, Lynch T, Morris ME. A comparison of Irish set dancing and exercises for people with Parkinson’s disease: a phase II feasibility study. BMC Geriatr. 2013;13(54):1–6.
- Hackney ME, Earhart GM. Health-related quality of life and alternative forms of exercise in Parkinson disease. Parkinsonism Relat Disord. 2009;15(9):644–648.
- Hackney ME, Earhart GM. Effects of dance on movement control in Parkinson’s disease: a comparison of Argentine tango and American ballroom. J Rehabil Med. 2009;41(6):475–481.
- Hackney ME, Earhart GM. Effects of dance on gait and balance in Parkinson’s disease: a comparison of partnered and nonpartnered dance movement. Neurorehabil Neural Repair. 2010;24(4):384–392.
- Hackney ME, Kantorovich S, Levin R, Earhart GM. Effects of tango on functional mobility in Parkinson’s disease: a preliminary study. J Neurol Phys Ther. 2007;31(4):173–179.
- Duncan RP, Earhart GM. Randomized controlled trial of community-based dancing to modify disease progression in Parkinson disease. Neurorehabil Neural Repair. 2012;26(2):132–143.
- Shanahan J, Morris ME, Ni Bhriain O, Volpe D, Lynch T, Clifford AM. Dancing for Parkinson disease: a randomized trial of Irish set dancing compared to usual care. Arch Phys Med Rehabil. 2017; S0003-9993(17):30162–30164.
- Rios Romenets S, Anang J, Fereshtehnejad S-M, Pelletier A, Postuma R. Tango for treatment of motor and non-motor manifestations in Parkinson’s disease: a randomized control study. Complement Ther Med. 2015;23(2):175–184.
- Keus SHJ, Munneke M, Graziona M, et al. European Physiotherapy Guideline for Parkinson’s Disease. The Netherlands: KNGF/ParkinsonNet; 2014.
- Hirsch MA, Iyer SS, Englert D, Sanjak M. Promoting exercise in Parkinson’s disease through community-based participatory research. Neurodegener Dis Manag. 2011;1(5):365–377.
- Allen K, Morey M. . Physical activity and adherence. In: Bosworth H, editor. Improving Patient Treatment Adherence: A Clinicians Guide. New York: Springer Science and Business Media; 2010: 9–38.
- Keogh JWL, Kilding A, Pidgeon P, Ashley L, Gillis D. Physical benefits of dancing for healthy older adults: a review. J Aging Phys Act. 2009;17(4):479–500.
- de Dreu MJ, Kwakkel G, van Wegen EEH. Partnered dancing to improve mobility for people with Parkinson’s disease. Front Neurosci. 2015;9:444.
- Lim LIIK, van Wegen EEH, de Goede CJT, et al. Measuring gait and gait-related activities in Parkinson’s patients own home environment: a reliability, responsiveness and feasibility study. Parkinsonism Relat Disord. 2005;11(1):19–24.
- Schwingel A. . Understanding human aging. In: Chodzko-Zajko WJ, editor. ACSM’s Exercise for Older Adults. USA: Lippincott Williams & Wilkins; 2014: 1–14.
- Shulman LM, Gruber-Baldini AL, Anderson KE, Fishman PS, Reich SG, Weiner WJ. The clinically important difference on the unified Parkinson’s disease rating scale. Arch Neurol. 2010;67(1):64–70.
- Horváth K, Aschermann Z, Ács P, et al. Minimal clinically important difference on the motor examination part of MDS-UPDRS. Parkinsonism Relat Disord. 2015;21(12):1421–1426.
- Tomlinson CL, Patel S, Meek C, et al. Physiotherapy intervention in Parkinson’s disease: systematic review and meta-analysis. BMJ. 2012;345:e5004.
- Tan D, Danoudis M, McGinley J, Morris ME. Relationships between motor aspects of gait impairments and activity limitations in people with Parkinson’s disease: a systematic review. Parkinsonism Relat Disord. 2012;18(2):117–124.
- Lakes KD, Marvin S, Rowley J, et al. Dancer perceptions of the cognitive, social, emotional, and physical benefits of modern styles of partnered dancing. Complement Ther Med. 2016;26:117–122.
- Friedman JH, Beck JC, Chou KL, et al. Fatigue in Parkinson’s disease: report from a mutidisciplinary symposium. NPJ Parkinsons Dis. 2016;2:15025.
- Shanahan J, Ni Bhriain O, Morris ME, Volpe D, Clifford AM. Irish set dancing classes for people with Parkinson’s disease: the needs of participants and dance teachers. 2016;27:12–17.
- Rocha PA, Slade SC, McClelland J, Morris ME. Dance is more than therapy: qualitative analysis on therapeutic dancing classes for Parkinson’s. Complement Ther Med. 2017;34:1–9.
- Thomas DR. The critical link between health-related quality of life and age-related changes in physical activity and nutrition. J Gerontol A Biol Sci Med Sci. 2001;56(10):M599–M602.
- Allen NE, Sherrington C, Suriyarachchi GD, Paul SS, Song J, Canning CG. Exercise and motor training in people with Parkinson’s disease: a systematic review of participant characteristics, intervention delivery, retention rates, adherence, and adverse events in clinical trials. Parkinsons Dis. 2012;2012:854328.