
Abstract
First-generation drug-eluting stents have raised concerns regarding the risk of late and very late stent thrombosis compared with bare metal stents and require prolonged dual antiplatelet therapy. Despite extensive investigations, the physiopathology of these late events remains incompletely understood. Aside from patient- and lesion-related risk factors, stent polymer has been cited as one of the potential causes. In fact, the persistence of durable polymer after complete drug release has been shown to be responsible for local hypersensitivity and inflammatory reactions. Third-generation drug-eluting stents with more biocompatible or biodegradable polymers have subsequently been developed to address this problem. In this article, we evaluate and discuss the concept and clinical results (safety and efficacy) of a third-generation drug-eluting stent with biodegradable polymer: the Nobori® stent.
Introduction
Percutaneous transluminal coronary angioplasty was introduced by Gruntzig in the late 1970s as an alternative to coronary artery bypass graft surgery for coronary revascularization.Citation1 Since then, percutaneous coronary intervention (PCI) has been accepted as a safe, reliable, and effective treatment for coronary artery disease, and its use has spread worldwide. Nevertheless, in-stent restenosis (ISR), a complex phenomenon resulting in renewed symptoms, need for re-intervention, and poor patient outcome remained for many years the Achilles’ heel of PCI.Citation2 The introduction, a decade ago, of first-generation drug-eluting stents (DESs) transformed the practice of PCI by drastically reducing the rate of this complication.Citation3 The efficacy of DESs has largely been demonstrated in large randomized trials, leading to their current widespread use in clinical practice. Even in high-risk populations, ISR incidence does not currently go above 5%–10%.Citation4–Citation6 However, major concerns regarding the long-term safety of these first-generation DESs have progressively arisen, especially the increased risk of late/very late stent thrombosis (ST)Citation7–Citation14 and the need for prolonged dual antiplatelet therapy (DAPT) with an inherent increase of bleeding complications. Aside from patient- and lesion-related factors, delayed re-endothelialization and recovery of endothelial function after stenting as well as inhibition of vascular repair after DES implantation, all of which promote inflammation and thrombotic pathways, have been implicated in the pathophysiology of late/very late ST. Of note, stent polymer has also been cited as one of the main causes of these late events. In fact, the persistence of a durable polymer after complete release of the anti-proliferative drug has been shown to be responsible for local hypersensitivity and inflammatory reactions.Citation15
These safety concerns prompted additional research, new trial design, and development of new-generation DESs to reduce the rate of this rare but critical event.
Apart from the progress in stent platforms (thinner struts and stent designs), recent research in this field has subsequently been focused on the development of new more biocompatible durable polymers or completely biodegradable polymers. Third-generation DESs using biodegradable polymers, like the Biolimus-eluting stent (BES) (Nobori®; Terumo Corporation, Tokyo, Japan), have been developed to overcome the long-term adverse vascular reactions related to the durable polymer.
In this article, we present information on the concept and rationale behind this new stent generation. We then discuss the results of recent publications investigating the safety and effectiveness of the use of the third-generation BES (Nobori®) for the treatment of coronary artery lesions.
Rationale for new stent development
The two major complications of PCI, ISR and ST, have always been the trigger for new stent development.Citation16 Indeed, despite the fact that these events are multifactorial, stent “structure” has been suggested to be one of the leading causes of ISR and/or ST.Citation17–Citation21
ISR physiopathology has not yet been fully understood. Barotrauma induced by PCI is responsible for endothelial denudation and sub-intimal hemorrhages, leading to a local inflammatory response. This inflammatory process induced by vascular damage is thought to be one of the main contributors to the development of restenosis, by promoting vascular smooth muscular cell proliferation and extracellular matrix formation, resulting in neointimal hyperplasia. Beside these mechanical factors, other factors have been identified as predictors for ISR, including patient-related (eg, diabetes mellitus, smoking, and renal failure) and lesion-related (eg, minimal lumen diameter after PCI, severe calcifications, chronic total occlusions, tortuous vessel, and long lesion length) factors.Citation22 As mentioned above, ISR remained the Achilles’ heel of PCI until the large use of DESs, which were specifically developed to overcome this complication. Before the introduction of bare-metal stents (BMSs), up to 50% of the patients treated by PCI experienced restenosis. Even in the BMS era, ISR remained one of the major limitations of this technique, with an average incidence of 20%, but that could increase up to 35% in complex lesions and diabetic patients.Citation4,Citation5 The introduction, 10 years ago, of first- and then second-generation DESs transformed the practice of PCI by drastically reducing the incidence of this complication to less than 10%.Citation3
DESs prevent restenosis by inhibiting vascular smooth muscle proliferation.Citation23–Citation31 Unfortunately, they also delay re-endothelialization of stent struts, leading to the potential risk of late/very late ST and thereby the need for prolonged DAPT. Since the appearance of DESs, ST has become the major safety concern in contemporary PCI practice. ST is a rare adverse event (1% at 1 year and then 0.5% per year) but remains associated with high morbidity and mortality rates.Citation32 The overall prognosis is poor: most patients in whom ST occurs present with STEMI (ST-segment elevation myocardial infarction) or out-of-hospital death, and up to 30% of those who arrive alive at hospital die within the first month. Numerous factors have been implicated in ST physiopathology, but studies have also shown that these predictors vary over time. These data highlight the complex physiopathology of ST, depending on the timing of event occurrence. Acute (within 24 hours) and early ST (within 30 days) are likely related to mechanical issues concerning the stent (eg, minimum stent area and suboptimal stent expansion), inadequate platelet inhibition, or patient prothrombotic factors.Citation33 Late (up to 1 year) and very late ST (after 1 year) have been attributed to incomplete vascular healing and/or inadequate neointimal coverage, which in turn, promote inflammation and activation of thrombotic pathwaysCitation15 and late or acquired stent malapposition. DAPT associating aspirin with an oral P2Y12 inhibitor has been shown to be the standard therapy following coronary stenting in order to significantly reduce cardiac events, especially ST after PCI.Citation34 Current guidelines support the use of DAPT for 6–12 months after DES implantation.Citation35–Citation39 In 2006, the potential risk of late/very late ST after DES implantation raised the question of prolonging DAPT even beyond the first year.Citation40–Citation41 However, prolonged DAPT has also clearly been associated with an increased risk of bleeding.Citation42–Citation47 Availability of new biodegradable polymers and/or stents may shorten the duration of necessary DAPT and therefore minimize the risk of major bleeding to which it is associated.
Stent “structure” and concept for new development
First- and second-generation DESs have three major components: the stent platform, the antiproliferative drug, and the polymer. All of these factors have been subject to modification and have become a target for research and development. Improvement of each component could indeed lead to better patient outcomes.
The stent platform is the scaffold of the stent. It provides the radial force to prevent vessel occlusion provoked by vessel injury following PCI. First-generation DESs used stainless steel platforms. Cobalt-chromium and later platinum-chromium platforms used in second-generation DESs permitted similar stents’ radial strength all the while enabling a thinner strut design and subsequently significantly improved deliverability and a reduced rate of ISR.Citation48–Citation49 Unfortunately, the presence of a permanent scaffold in the vessel constitutes a stimulus for platelet aggregation and may lead to ST in patients with nonoptimal antiplatelet therapy and/or incomplete stent endothelialization. Recently, bioabsorbable platforms that biodegrade over a period of months have been developed, with the purpose of allowing the restoration of a normal vascular physiology and function over time. Ultimately, no foreign material is left exposed in the bloodstream. These stents may also potentially preserve reactive vasomotion and permit expansive remodeling.Citation50
There are several antiproliferative drugs with different modes of action. The goal of these drugs is to inhibit vascular smooth cell proliferation and migration, without affecting endothelial regeneration, and have anti-inflammatory/anti-thrombotic properties. Inhibitors of the mammalian target of rapamycin (mTOR) are the dominant class of anti-proliferative drugs used for DESs. The first mTOR inhibitor used in clinical practice was sirolimus. Later derivatives include zotarolimus and everolimus. The mTOR inhibitors are cytostatic drugs resulting in arrest of the cell cycle at the G1 phase. Aside from mTOR inhibitors, tacrolimus, which acts as a calcineurin inhibitor, has also been used in DESs and is a cytostatic agent with both antiproliferative and anti-inflammatory activities. Finally, paclitaxel is a taxan drug, which acts as a cytotoxic drug through the stabilization of microtubules. However, all these antiproliferative agents have shown detrimental local effects on the vascular wall and on endothelial function recovery after stenting.Citation11 New drugs (biolimus, novolimus, and myolimus) have been developed and have shown promising results.Citation51–Citation52 Compared with other mTOR inhibitors, biolimus shows better lipophilicity. Agents other than drugs are under investigation to limit restenosis, such as antibody-coated stents (CD34 antibody-coated stents) and nucleotide- or peptide-coated stents. The ultimate goal remains the inhibition of maladaptive neointimal proliferation, all the while promoting vascular healing.
Stent polymers control elution of the antiproliferative drug over a variable period of time. Once drug elution has been completed, most polymers exert limited functions and act as a potential trigger for local inflammation and hypersensitivity and subsequently late/very late ST. They promote an inflammatory response and eosinophilic infiltration in the arterial wall, causing hypersensitivity reactions and endothelial dysfunction responsible for delayed healing and lead to ST.Citation11,Citation12,Citation22,Citation53 The biocompatibility, composition, formulation, degradation delay of the polymer, pharmacokinetics of the antiproliferative agent released by the polymer, and the management of variation in polymer degradation delay have become new difficult challenges for the development of stent polymers. An optimal polymer should mimic the endothelial lining in order to prevent late thrombotic complications, thus improving stent safety. Given the issue of polymer-induced inflammation and thrombosis, more biocompatible durable polymers have been developed. Second-generation DESs are composed of these polymers, thereby improving arterial healing and potentially reducing the rate of late ischemic events. The limited function of stent polymers once the drug is eluted has also fuelled research in biodegradable polymers. Third-generation DESs use polylactic acids (poly-L-lactic acid and poly D,L-lactide-co-glycolide) as bioabsorbable polymers. The BES with biodegradable polymer (Nobori®) is one of these third-generation DESs. Finally, another field of research is the development of stents that elute antiproliferative drugs without the need for polymers. These polymer-free stents could prevent the potential adverse physical effects of the polymer, leading to sustained intima inhibition, improved healing, and a lessened activation of the inflammatory/thrombotic pathways. Preclinical studies support their use, but robust data are still lacking.
The BES with biodegradable polymer (Nobori®) stent: design and clinical results
Safety, efficacy, and deliverability are the main sought-out properties for the development of new DESs. An optimal combination of these components, which are in part interdependent, is necessary for enhancing stent performance.
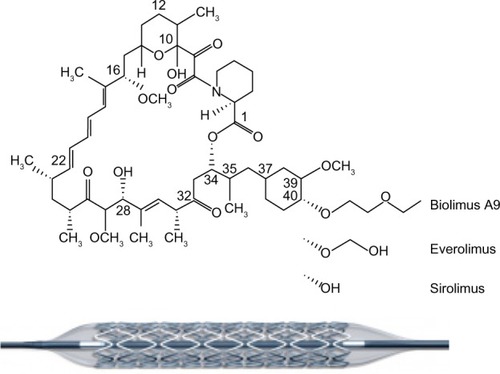
The BES stent with biodegradable polymer (Nobori®) is one of the third-generation DESs (). The platform is composed of stainless steel, and the strut thickness is 112 μm. It is coated with a polylactic acid polymer on its abluminal surface, which is metabolized within 6–9 months to lactic acid, water, and carbon dioxide through interaction with the Krebs cycle. The stent elutes an antiproliferative drug, biolimus (15.6 μg/mm), for up to 30 days. The coating design of the stent combined with the lipophilicity of the drug is thought to optimize local drug distribution and to reduce its release into the general circulation. At the end, the Nobori® stent will leave only a BMS in place.
Figure 1 The Biolimus-eluting stent (Nobori®; Terumo Corporation, Tokyo, Japan): chemical structure of Biolimus A9 and stent design. Replacement of hydrogen by alkoxy-alkyl group at 40-O position increases its lipophilicity.
The Nobori® stent has already been compared with first- and second-generation DESs with promising results. The NOBORI CORE trialCitation54 reported late-loss with the Nobori® stent at 9 months, similar to that found using the sirolimus-eluting stent (SES, Cypher®; Cordis Corporation, Bridgewater, NJ, USA): 0.10 and 0.12 mm, respectively (P=0.66). However, the use of the Nobori® stent results in better endothelial recovery, with normal coronary vasodilatation in the adjacent stent segments after implantation, contrasting with the paradoxical vasoconstriction seen with first-generation DESs.Citation55,Citation56 The NOBORI I trial showed non-inferiority to and subsequent superiority of the Nobori® stent over the paclitaxel-eluting stent (Taxus®, Boston Scientific, Maple Grove, MN, USA): late-loss 0.11 versus 0.32 mm, P<0.001. Moreover, this trial demonstrated a lower rate of ST with the Nobori® stent after a 9-month follow-up.Citation57
Three recent large randomized trials have compared safety and efficacy of this third-generation DES with that of first- and second-generation DESs with durable polymer ().Citation58
Table 1 Characteristics and principal results of recent trials with the Nobori® (Terumo Corporation, Tokyo, Japan) stent as compared with first- and second-generation DESs
The SORT OUT V trialCitation59 enrolled 2,468 patients who underwent PCI in Denmark and randomized them 1:1 using the Nobori® and Cypher® stents. This trial was a multicenter, prospective, non-inferiority trial (non-inferiority margin chosen at 2%) comparing the BES using biodegradable polymer with the SES using permanent polymer. A total of 1,229 patients were assigned to the BES group (1,532 lesions) and 1,239 to the SES group (1,555 lesions). DAPT was pursued at least 12 months after the procedure. The primary endpoint was a composite of safety (cardiac death, myocardial infarction [MI], and ST) and efficacy (target lesion revascularization [TLR]) within 9 months of stent implantation (intention-to-treat analysis). There were 75% male, and only 15% of the patients had a history of diabetes. Altogether, 17% had undergone a previous coronary intervention. PCI was performed in an acute setting in 49% of cases in both groups. The main target vessel location was the left anterior descending (LAD) artery (40.8%). Procedure characteristics were similar between the two groups, except for maximum stent pressure, which was significantly higher in the SES group (18 versus 16 atm, P<0.0001). Composite primary endpoint occurred in 4.1% of cases in the BES group and 3.1% of cases in the SES group (one-sided Pnon-inferiority=0.06, and P=0.22 for superiority). Cardiac death and TLR were not significantly different between the BES and SES groups (0.7% versus 1%, P=0.38; 3.3% versus 2.1%, P=0.07). Of note, ST occurred more frequently in the BES group (especially within the first month), with no clear explanation, and the rate of ST was particularly low in the SES group: 0.7% versus 0.2%, P=0.03. The authors concluded that the BES did not show non-inferiority when compared with the first-generation SES at 9 months.
The COMPARE II trialCitation60 was a multicenter, open-label, randomized, controlled, non-inferiority trial (non-inferiority margin chosen at 4%) and aimed to compare the safety and efficacy of the BES using biodegradable polymer with a second-generation everolimus-eluting stent (EES) using durable biocompatible polymer (Xience V® [Abbott Vascular, Santa Clara, CA, USA] or Prime® [Boston Scientific Corporation, Natick, MA, USA]). Altogether, 2,707 patients were enrolled and assigned 2:1. A total of 1,795 patients (2,638 lesions) received a BES, and 912 patients (1,387 lesions) an EES. DAPT was continued for a minimum of 12 months. The primary endpoint was a composite of safety (cardiac death and non-fatal MI) and efficacy (TLR) at 12 months. There were 74% male, 21.7% diabetics, and 20% had a previous history of MI. PCI was performed in an acute setting in 57.9% of cases. The LAD artery was the main target vessel (40.3%). Only 6.5% of the lesions were bifurcation lesions. Procedure characteristics were not significantly different between the groups but the rate of non-allocated stent implantation was higher in the BES group. Primary endpoint occurred in 5.2% of cases in the BES group and 4.8% in the EES group (one-sided Pnon-inferiority<0.0001, and P=0.69 for superiority). There was no difference in the rates of cardiac death (0.8% in each group, P=0.97) and MI (2.8% in the BES group versus 2.5% in the EES group; P=0.63). The rate of definite ST (0.7% versus 0.4%, P=0.38) and definite/probable ST (0.8% versus 1%, P=0.58) were very low and comparable between the two groups. Target vessel revascularization did not differ between the BES group (2.9%) and the EES group (2.6%, P=0.69). The authors concluded that the BES was shown to be non-inferior to the EES in terms of safety and efficacy at 1-year follow-up after PCI. The 5-year follow-up of the study should answer the question of long-term safety and efficacy of the BES compared with second-generation DESs.
The NEXT trialCitation61 was a prospective, multicenter, randomized, open-label, non-inferiority trial (non-inferiority margin chosen at 3.4%) comparing the BES (Nobori®) with the EES (Xience V® or Prime®) in terms of TLR at 1 year. DAPT was continued at least 3 months after the procedure. From May to October, 2011, in 98 Japanese centers, 3,235 patients were randomized 1:1 without any exclusion criteria to undergo PCI with either the BES or the EES. Altogether, 30% of included patients were over 75 years old, and 46% of the population in each group were diabetic. PCI was performed in a stable clinical setting for 83% of patients. The target vessel location was the LAD artery in 48% of cases. Efficacy endpoint was any TLR at 1 year, whereas the primary safety endpoint was a composite of death and MI. Primary efficacy endpoint occurred in 4.2% in both the BES group and the EES group (one-sided Pnon-inferiority<0.0001, and P=0.93 for superiority). The rate of any MI and stroke was similar between the two groups (3.3% versus 3.1 [P=0.77] and 1.4% versus 1.5% [P=0.89]). No difference was observed in terms of mortality, 2.6% and 2.5% in the BES and EES groups, respectively, P=0.9. With regard to the rate of ST, the incidence was extremely low, and there was no difference between the BES group and the EES group (0.25% and 0.06%, P=0.18). The angiographic sub-study shows that the difference in in-segment late loss between the two groups was −0.03 mm, demonstrating non-inferiority of the BES, with a margin of 0.195 mm. Of note, the rate of stent fracture was significantly higher in the BES group (3.1% versus 0%; P=0.004). The authors concluded in the non-inferiority of the BES over the EES in the setting of stable coronary artery disease. Clinical outcomes were excellent, with a low rate of TLR and extremely low rate of ST in each group.
Discussion
Third-generation DESs using biodegradable polymer such as the Nobori® stent have been developed to overcome long-term adverse effects observed with first-generation DESs related to the use of durable polymers, and to thereby shorten the duration of DAPT and the ensuing risk of hemorrhagic complications. Biodegradable BESs should nonetheless possess similar efficacy to actual DESs in preventing ISR (lower rate of TLR as compared with BMSs).
First studies evaluating BES efficacy and safety have shown promising results, with significantly lower in-stent late loss than with paclitaxel-eluting stents, and similar in-stent late loss as SESs.Citation54,Citation57 However, the recent COMPARE-II, SORT OUT V, and NEXT trials, all three of which were sufficiently powered to compare clinical outcomes, showed contrasting results. To date, only the COMPARE-II and the NEXT trials have evaluated a new third-generation DES versus a second-generation DES (Xience V® or Prime®). The COMPARE-II trial demonstrated non-inferiority of the BES relative to second-generation EESs, but procedural failure was significantly higher in the BES group.Citation60 By contrast, non-inferiority of the BES relative to the first-generation SES was not shown in the SORT OUT V trial due to a higher risk of early ST without a clear explanation for this phenomenon.Citation59 In fact, the rate of ST was particularly low in the SES group in this study. The NEXT trial is the largest trial, to date, evaluating the efficacy and safety of the BES as compared with the EES.Citation61 In this trial, clinical and angiographic outcomes of the BES group were non-inferior to the EES group, and the device implantation success rate was comparable in both groups. Of note, a higher rate of stent fracture was seen in the BES group in the angiographic sub-study of the NEXT trial, but its imputability in very late ST or TLR is uncertain and needs further exploration.
Of major importance, all these trials have enrolled low risk patients, and notably a low incidence of diabetics, with relatively simple angiographic lesions (eg, large vessels, low rate of bifurcations, and lesion length <20 mm). PCI was also performed in the majority of cases in a stable clinical setting. These facts are critical regarding the interpretation of the results and the low rate of adverse events observed in these three trials: the primary efficacy endpoint was lower than 5% in all studies, and any conclusion must be interpreted with caution, especially in non-inferiority trials. In addition, a safety comparison of modern DESs is challenging. Indeed, ST, especially very late ST, is a rare complication, and although 12-month results of standard trials usually enable safety or efficacy to be assessed, longer follow-up (5 years or more) and large trials are mandatory in the present case in regard of late-event exploration. The rate of ST in the present studies is particularity low (around 0.5% at 1 year), and these trials are not powered enough to evaluate such a low frequency event. Finally, if present, the expected benefit of third-generation DESs like the Nobori® stent over older DESs would logically appear only after 1 year. To date, no very late ST with the Nobori® stent has been reported in the literature, with the limitation that long-term follow-up is currently only available for very few patients.
The LEADERS trial was the first randomized study to evaluate BESs against durable polymer first-generation DESs. This trial included higher risk patients, and the rate of events was on average twice as high as compared with the COMPARE II, SORT OUT V, and NEXT trials. The LEADERS study compared another third-generation BES (Biomatrix Flex®, Biosensors, Newport Beach, CA, USA) with SESs. The only difference between the Biomatrix Flex® and the Nobori® stent is the presence of an ultra-thin non-degradable parylene coating between the stent and the polymer on the Nobori® stent to assure polymer attachment to the stent struts, which do not exist on the Biomatrix Flex®. The final 5-year report has just been publishedCitation62 and demonstrates that the BES is non-inferior to the SES with regard to the primary endpoint (cardiovascular death, MI, and clinically driven target vessel revascularization) (22.3% in the BES group versus 26.1% in the SES group; P=0.071). In addition, even though no significant difference was observed between the BES and the SES in total definite ST at 5 years, the BES was associated with a significantly lower rate of very late ST and secondary composite endpoint (all cause death, any MI, any revascularization) (0.6% in the BES group versus 2.2% in the SES group for very late ST [P=0.003], and 35.1% versus 40.4% for secondary composite endpoint [P=0.02]).Citation62
A recently pooled analysis based on patient individual data from the ISAR-TEST 3, the ISAR-TEST 4, and the LEADERS trialCitation63 has demonstrated that biodegradable polymer DESs (including: biodegradable polymer BES [Biomatrix Flex®], n=857; and biodegradable polymer SES, n=1,501) improve safety and efficacy over first-generation SESs during long-term follow-up. The three trials separately showed no differences between BESs and DESs in the past, highlighting the lack of statistical power of these studies (taken alone) to detect relevant differences in very low frequency events such as ST. In this meta-analysis, the benefit of BESs was seen in the rate of ST (0.2% versus 1.3%, P=0.004), MI (1.5% versus 3%, P=0.03), and cardiac death (3.9% versus 4.9%, P=0.05). Of note, BESs also showed a significant reduction in TLR in this meta-analysis (12% versus 13.7%, P=0.029). These trials were performed with sirolimus first-generation DESs as control, and results cannot be extended to other second-generation DESs. Further studies using second-generation DESs as control are required to make any conclusions. Interestingly, such a meta-analysis of trials that have evaluated the Nobori® stent may carry interesting conclusions in the next future.
Conclusion
BMSs and DESs have changed the landscape of current PCI by significantly reducing the rate of ISR. However, first-generation DESs have been associated with a higher rate of late or very late ST. The physiopathology of this rare but serious event is multifactorial, but inflammation and delayed arterial healing, of which the durable polymer may be a putative mechanism, has an important role. The concept of biodegradable polymer and totally bioresorbable scaffolds looks, in consequence, very interesting. Data currently available have shown promising but contrasting results. Long-term follow-up is mandatory to see if the implantation of these third-generation DESs will improve clinical outcomes with a lower rate of ST and MI. Further studies and results of their long-term follow-up would definitely shed light on patient outcomes with the use of such devices.
Disclosure
The authors report no conflicts of interest in this work.
References
- GruntzigARSenningASiegenthalerWENonoperative dilatation of coronary-artery stenosis: percutaneous transluminal coronary angioplastyN Engl J Med19793016168449946
- AgemaWRJukemaJWPimstoneSNKasteleinJJGenetic aspects of restenosis after percutaneous coronary interventions: towards more tailored therapyEur Heart J2001222058207411686664
- MoriceMCSerruysPWSousaJEA randomized comparison of a sirolimus-eluting stent with a standard stent for coronary revascularizationN Engl J Med20023461773178012050336
- SigwartUPuelJMirkovitchVJoffreFKappenbergerLIntravascular stents to prevent occlusion and restenosis after transluminal angioplastyN Engl J Med19873167017062950322
- FischmanDLLeonMBBaimDSA randomized comparison of coronary-stent placement and balloon angioplasty in the treatment of coronary artery disease. Stent Restenosis Study InvestigatorsN Engl J Med19943314965018041414
- FattoriRPivaTDrug-eluting stents in vascular interventionLancet200336124724912547552
- LemesleGMaluendaGCollinsSDWaksmanRDrug-eluting stents: issues of late stent thrombosisCardiol Clin2010289710519962052
- LemesleGPinto SlottowTLWaksmanRVery late stent thrombosis after bare-metal stent implantation: case reports and review of the literatureJ Invasive Cardiol200921273219126924
- DaemenJWenaweserPTsuchidaKEarly and late coronary stent thrombosis of sirolimus-eluting and paclitaxel-eluting stents in routine clinical practice: data from a large two-institutional cohort studyLancet200736966767817321312
- JensenLOTilstedHHThayssenPPaclitaxel and sirolimus eluting stents versus bare metal stents: long-term risk of stent thrombosis and other outcomes. From the Western Denmark Heart RegistryEuroIntervention2010589890520542774
- JonerMFinnAVFarbAPathology of drug-eluting stents in humans: delayed healing and late thrombotic riskJ Am Coll Cardiol2006419320216814667
- CookSLadichENakazawaGCorrelation of intravascular ultrasound findings with histopathological analysis of thrombus aspirates in patients with very late drug-eluting stent thrombosisCirculation200912039139919620501
- GargPMauriLThe conundrum of late and very late stent thrombosis following drug-eluting stent implantationCurr Opin Cardiol20072256557117921745
- McFaddenEPStabileERegarELate thrombosis in drug-eluting coronary stents after discontinuation of antiplatelet therapyLancet20043641519152115500897
- InoueTCroceKMorookaTSakumaMNodeKSimonDIVascular inflammation and repair, implications for re-endothelialization, restenosis and stent thrombosisJACC Cardiovasc Interv201141057106622017929
- GargSSerruysPWNew concepts in the design of drug-eluting coronary stentsNat Rev Cardiol20131024826023419901
- OtsukaFVorpahlMNakanoMPathology of second-generation everolimus-eluting stents versus first-generation sirolimus- and paclitaxel-eluting stents in humansCirculation201412921122324163064
- BriguoriCSaraisCPagnottaPIn-stent restenosis in small coronary arteries: impact of strut thicknessJ Am Coll Cardiol20024040340912142103
- OrmistonJAWebsterMWRuygrokPNStent strut thickness and restenosisCirculation20021052E1211790719
- TanigawaJBarlisPDimopoulosKDalbyMMoorePDi MarioCThe influence of strut thickness and cell design on immediate apposition of drug-eluting stents assessed by optical coherence tomographyInt J Cardiol200913418018818775576
- HaraHNakamuraMPalmazJCSchwartzRSRole of stent design and coatings on restenosis and thrombosisAdv Drug Deliv Rev20065837738616650911
- JukemaJWVerschurenJJAhmedTAQuaxPHRestenosis after PCI. Part 1: pathophysiology and risk factorsNat Rev Cardiol20119536221912414
- SerruysPWOngATMoriceMCArterial Revascularisation Therapies Study Part II – Sirolimus-eluting stents for the treatment of patients with multivessel de novo coronary artery lesionsEuroIntervention2005114715619758896
- GrubeESilberSHauptmannKETAXUS I: six- and twelve-month results from a randomized, double-blind trial on a slow-release paclitaxel-eluting stent for de novo coronary lesionsCirculation2003107384212515740
- SerruysPWMoriceMCKappeteinAPSYNTAX InvestigatorsPercutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery diseaseN Engl J Med200936096197219228612
- SabatéMJiménez-QuevedoPAngiolilloDJDIABETES InvestigatorsRandomized comparison of sirolimus-eluting stent versus standard stent for percutaneous coronary revascularization in diabetic patients: the diabetes and sirolimus-eluting stent (DIABETES) trialCirculation20051122175218316203930
- KirtaneAJEllisSGDawkinsKDPaclitaxel-eluting coronary stents in patients with diabetes mellitus: pooled analysis from 5 randomized trialsJ Am Coll Cardiol20085170871518279734
- SpauldingCHenryPTeigerETYPHOON InvestigatorsSirolimus-eluting versus uncoated stents in acute myocardial infarctionN Engl J Med20063551093110416971716
- LaarmanGJSuttorpMJDirksenMTPaclitaxel-eluting versus uncoated stents in primary percutaneous coronary interventionN Engl J Med20063551105111316971717
- MeredithITOrmistonJWhitbournRKayIPMullerDCutlipDEENDEAVOR I InvestigatorsFive-year clinical follow-up after implantation of the Endeavor zotarolimus-eluting stent: ENDEAVOR I, first-in-human studyCatheter Cardiovasc Interv20097498999519859958
- WiemerMSerruysPWMiquel-HebertKFive-year long-term clinical follow-up of the XIENCE V everolimus eluting coronary stent system in the treatment of patients with de novo coronary artery lesions: the SPIRIT FIRST trialCatheter Cardiovasc Interv201075997100320517959
- SerruysPWDaemenJAre drug-eluting stents associated with a higher rate of late thrombosis than bare metal stents? Late stent thrombosis: a nuisance in both bare metal and drug-eluting stentsCirculation200711514331439 discussion 143917344323
- JaffeRStraussBHLate and very late thrombosis of drug-eluting stents: evolving concepts and perspectivesJ Am Coll Cardiol20075011912717616295
- BrilakisESPatelVGBanerjeeSMedical management after coronary stent implantation: a reviewJAMA20131018919823839753
- StegPGJamesSKAtarDTask Force on the management of ST-segment elevation acute myocardial infarction of the European Society of Cardiology (ESC)ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevationEur Heart J2012332569261922922416
- MehtaSRYusufSPetersRJClopidogrel in Unstable Angina to Prevent Recurrent Events Trial (CURE) InvestigatorsEffects of pretreatment with clopidogrel and aspirin followed by long-term therapy in patients undergoing percutaneous coronary intervention: the PCI-CURE studyLancet200135852753311520521
- SteinhublSRBergerPBMannJT3rdCREDO InvestigatorsClopidogrel for the Reduction of Events During Observation. Early and sustained dual oral antiplatelet therapy following percutaneous coronary intervention: a randomized controlled trialJAMA20022882411242012435254
- WiviottSDBraunwaldEMcCabeCHTRITON-TIMI 38 InvestigatorsPrasugrel versus clopidogrel in patients with acute coronary syndromesN Engl J Med20073572001201517982182
- WallentinLBeckerRCBudajAPLATO InvestigatorsTicagrelor versus clopidogrel in patients with acute coronary syndromesN Engl J Med20093611045105719717846
- IakovouISchmidtTBonizzoniEIncidence, predictors, and outcome of thrombosis after successful implantation of drug-eluting stentsJAMA200522932126213015870416
- EisensteinELAnstromKJKongDFClopidogrel use and long-term clinical outcomes after drug-eluting stent implantationJAMA200729715916817148711
- ValgimigliMCampoGMontiMProlonging Dual Antiplatelet Treatment After Grading Stent-Induced Intimal Hyperplasia Study (PRODIGY) InvestigatorsShort- versus long-term duration of dual-antiplatelet therapy after coronary stenting: a randomized multicentre trialCirculation20121252015202622438530
- ParkSJParkDWKimYHDuration of dual antiplatelet therapy after implantation of drug-eluting stentsN Engl J Med20103621374138220231231
- GwonHCHahnJYParkKWSix-month versus 12-month dual antiplatelet therapy after implantation of drug-eluting stents: the Efficacy of Xience/Promus Versus Cypher to Reduce Late Loss After Stenting (EXCELLENT) randomized, multicenter studyCirculation201212550551322179532
- KimBKHongMKShinDHRESET InvestigatorsA new strategy for discontinuation of dual antiplatelet therapy: the RESET Trial (Real Safety and Efficacy of 3-Month Dual Antiplatelet Therapy following Endeavor zotarolimus-eluting stent implantation)J Am Coll Cardiol2012601340134822999717
- CasseseSByrneRATadaTKingLAKastratiAClinical impact of extended dual antiplatelet therapy after percutaneous coronary interventions in the drug-eluting stent era: a meta-analysis of randomized trialsEur Heart J2012333078308723091199
- HawnMTGrahamLARichmanJSItaniKMHendersonWGMaddoxTMRisk of major adverse cardiac events following noncardiac surgery in patients with coronary stentsJAMA20133101462147224101118
- KastratiAMehilliJDirschingerJIntracoronary stenting and angiographic results: strut thickness effect on restenosis outcome (ISAR-STEREO) trialCirculation20011032816282111401938
- PacheJKastratiAMehilliJIntracoronary stenting and angiographic results: strut thickness effect on restenosis outcome (ISAR-STEREO-2) trialJ Am Coll Cardiol2003411283128812706922
- SerruysPWOrmistonJAOnumaYA bioabsorbable everolimus-eluting coronary stent system (ABSORB): 2-year outcomes and results from multiple imaging methodsLancet200937389791019286089
- CostaJRJrAbizaidAFeresFEXCELLA First-in-Man (FIM) study: safety and efficacy of novolimus-eluting stent in de novo coronary lesionsEuroIntervention20084535819112779
- OrmistonJAMulticenter FIM study with a low dose elixir myolimus-eluting coronary stent system with a bioabsorable polymer: 6-month angiographic and IvUS resultsPresented at Transcatheter Cardiovascular Therapeutics (TCT)October 12–17, 2008Washington, DC
- JonerMNakazawaGFinnAVEndothelial cell recovery between comparator polymer-based drug-eluting stentsJ Am Coll Cardiol20085233334218652940
- OstojicMSagicDBeleslinBFirst clinical comparison of Nobori Biolimus A9 eluting stents with Cypher sirolimus eluting stents: Nobori Core nine months angiographic and one year clinical outcomesEuroIntervention2008357457919608483
- HamilosMOstojicMBeleslinBDifferential effects of drug-eluting stents on local endothelium-dependent coronary vasomotionJ Am Coll Cardiol20082512123212918510958
- HamilosMSarmaJOstojicMInterference of drug-eluting stents with endothelium-dependent coronary vasomotion: evidence for device-specific responsesCirc Cardiovasc Interv2008119320020031678
- ChevalierBSilberSParkS-JRandomized comparison of the Nobori Biolimus A9-eluting coronary stent with the Taxus Liberte paclitaxel-eluting coronary stent in patients with stenosis in native coronary arteries: the NOBORI 1 trial – phase 2Circ Cardiovasc Interv2009218819520031715
- LemesleGSchurtzGDelhayeCBiolimus eluting stent with biodegradable polymer (Nobori®): an overview of recent clinical results, SORT OUT V and COMPARE II trialsExpert Rev Cardiovasc Ther2013111293129624090440
- ChristiansenEHJensenLOThayssenPScandinavian Organization for Randomized Trials with Clinical Outcome (SORT OUT) V investigatorsBiolimus-eluting biodegradable polymer-coated stent versus durable polymer-coated sirolimus-eluting stent in unselected patients receiving percutaneous coronary intervention (SORT-OUT V): a randomized non-inferiority trialLancet201338166166923374649
- SmitsPCHofmaSTogniMAbluminal biodegradable polymer biolimus-eluting stent versus durable polymer everolimus-eluting stent (COMPARE II): a randomized, controlled, non-inferiority trialLancet201338165166023374650
- NatsuakiMKozumaKMorimotoTNEXT InvestigatorsBiodegradable polymer biolimus-eluting stent versus durable polymer everolimus-eluting stent: a randomized, controlled, noninferiority trialJ Am Coll Cardiol20136218119023684673
- SerruysPWFarooqVKalesanBImproved safety and reduction in stent thrombosis associated with biodegradable polymer-based biolimus-eluting stents versus durable polymer-based sirolimus-eluting stents in patients with coronary artery disease. Final 5-year report of the LEADERS trialJ Am Coll Cardiol Interv20136777789
- StefaniniGGByrneRASerruysPWBiodegradable polymer drug-eluting stents reduce the risk of stent thrombosis at 4 years in patient undergoing percutaneous coronary intervention: a pooled analysis of individual patient data from the ISAR-TEST 3, ISAR-TEST 4, and LEADERS randomized trialsEur Heart J2012331214122222447805