
Abstract
Based on the principle of surgical edge-to-edge mitral valve repair (MVR), the MitraClip percutaneous MVR technique has emerged as a minimally invasive option for MVR. This catheter-based system has been widely demonstrated to be safe, although inferior to surgical MVR. Studies examining patients with ≥3+ mitral regurgitation (MR) show that, for all patients treated, freedom from death, surgery, or MR ≥3+ is in the 75%–80% range 1 year following MitraClip implantation. Despite its inferiority to surgical therapy, in high-risk surgical patients, data suggest that the MitraClip system can be employed safely and that it can result in symptomatic improvement in the majority of patients, while not precluding future surgical options. MitraClip therapy also appears to reduce heart failure readmissions in the high-risk cohort, which may lead to an economic benefit. Ongoing study is needed to clarify the impact of percutaneous mitral valve clipping on long-term survival in high-risk populations, as well as its role in other patient populations, such as those with functional MR.
Introduction
Mitral regurgitation (MR) continues to impose significant morbidity and mortality on patients. Since even asymptomatic MR typically progresses to left ventricular dilatation, left ventricular failure, worsening MR, and eventual symptom onset, surgical therapy has traditionally been advocated to break this cycle. However, though effective, even mitral valve repair (MVR), as opposed to replacement, has been associated with first-time operative mortality rates in the 2% range, and reoperative mortality rates as high as 8%.Citation1 Accordingly, the MitraClip system has emerged as a transcatheter method of treating MR while avoiding the adverse effects associated with cardiopulmonary bypass and open cardiac surgery.
History
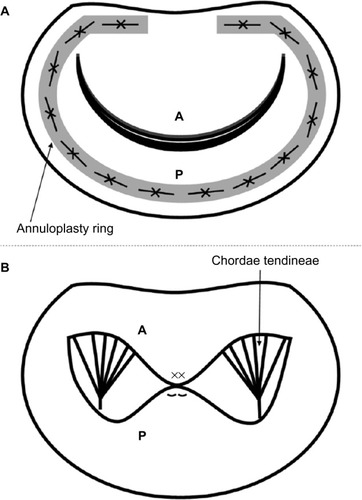
The history of the MitraClip begins with advances made in the surgical treatment of MR. For at least two decades, it has become clear that for most patients, mitral repair (rather than replacement) provides superior outcomes at lower risk.Citation2,Citation3 Traditionally, repair has been performed via ring annuloplasty based on the seminal work of Dr Carpentier and others,Citation4,Citation5 but other techniques have been proposed (). The MitraClip technology draws on experience with the edge-to-edge MVR, first described by Dr Alfieri in the 1990s.Citation6 This technique, first employed in patients with single or bileaflet prolapse, involves the placement of suture to anchor the free edge of the prolapsed leaflet to its corresponding opposite leaflet. Alfieri’s simple method results in the creation of two valve orifices if prolapse occurs in the middle portion of a leaflet, or a smaller valve orifice should the lesion be pericommissural.Citation7 This “double-orifice” technique omitted annuloplasty. In his original series, Alfieri documented rates of survival and freedom from reoperation to be above 90% over 5 years after MVR using his technique.Citation6
Figure 1 Schematic diagram of two methods of mitral valve repair.
Abbreviations: A, anterior mitral leaflet; P, posterior mitral leaflet.
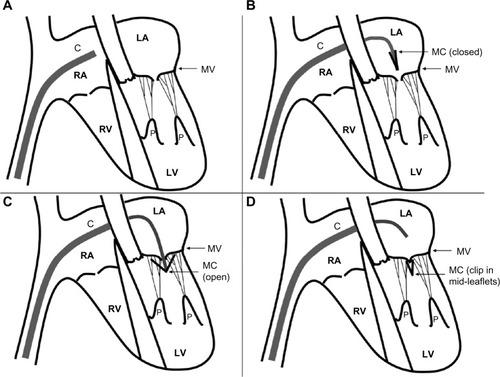
Based on these findings, investigators at major academic institutions in concert with private industry (Evalve, Redwood City, CA, USA; later Abbot Vascular, Santa Clara, CA, USA) developed a transcatheter method of accomplishing reapproximation of the anterior and posterior mitral leaflets as a therapy for MR. This method was first described in adult pigs in 2003.Citation8 The original device was inserted via the femoral vein and utilized a 24Fr guidewire to gain transseptal access to the left atrium (). The tip of this catheter was designed with a bidirectional steering mechanism so it can be positioned centrally above the mitral valve annulus. Once the delivery catheter is in position, a V-shaped clip is introduced while closed. The clip, which is polyester-covered and made of cobalt–chromium, spans about 4 mm when closed, and has a maximum arm excursion of about 20 mm when opened (). The clip is then opened and rotated in the left atrium so as to be perpendicular to the lines of leaflet coaptation, advanced into the left ventricle, and then retracted during systole to snare the anterior and posterior leaflets (). Importantly, the clip can be opened and closed repeatedly to ensure optimal positioning.
Figure 2 Schematic of MitraClip device insertion.
Abbreviations: C, MitraClip catheter; MC; MitraClip clip; LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle; MV, mitral valve; P, papillary muscles.
Early animal data using this technique were promising. In the first report of clip use in 14 adult pigs, a functional double-orifice valve was achieved in 12 animals.Citation8 The clip failed to grasp the anterior leaflet in the remaining two animals, which the authors determined was due to incomplete opening of the clip prior to positioning. Following sacrifice, none of the animals exhibited significant injury to other cardiac structures. A subsequent study by the same investigators using the same animal model (but with direct left atrial access via thoracotomy instead of femoral vein access) demonstrated successful clip placement in all 21 animals utilized.Citation9 After various survival points between 4 and 52 weeks, 20 of the 21 animals (96%) had a double-orifice valve on necropsy. Adequate histopathologic evidence of healing and endothelialization were also noted in all animals except for two that developed endocarditis and required early euthanization.
Current surgical techniques to address mitral regurgitation
Consideration should be given to the current state of the art in open surgical therapy for MR. As mentioned earlier, the placement of a synthetic ring around the mitral annulus to improve leaflet coaptation was first recommended by Dr Carpentier and has since been shown to provide durable long-term relief from MR, with up to 90% of degenerative mitral valves able to be repaired in this fashion.Citation4,Citation5,Citation10 Ring annuloplasty, though, represents only one technique to address MR, which Dr Carpentier and various others have advocated. Isolated prolapse of the posterior leaflet, which can occur due to chordal rupture, can be addressed by triangular or quadrangular resection of the leaflet’s central portion, with reapproximation to “tighten” it. However, care must be taken to not over-correct the defect, or systolic anterior motion of the anterior mitral valve leaflet into the outflow tract may result.Citation11 Another method to address a prolapsing leaflet is the placement of artificial polytetrafluoroethylene (PTFE) neochordae “loops” between the leaflet and papillary muscle in order to pull a prolapsing leaflet downward and improve coaptation, and/or to replace ruptured papillary muscles or chordae tendineae.Citation12,Citation13 This method, which requires careful measurement to ensure appropriate length of the PTFE neochordae, has been demonstrated to be safe and effective on long-term follow-up as well.Citation14,Citation15 At least one randomized trial has shown that leaflet resection and PTFE neochordae placement have similar early and mid-term outcomes,Citation16 a finding echoed by other investigators.Citation17,Citation18
Newer technologies have led to less invasive approaches to utilize the same principles while minimizing the morbidity of open cardiac surgery. All of the above approaches today are often performed through a right lateral mini-thoracotomy or a conventional median sternotomy. With the introduction of the robotic surgery and the Da Vinci robotic system (Intuitive Surgical, Sunnyvale, CA, USA), MVR can be accomplished through five trocar ports in the right chest and peripheral cardiopulmonary bypass cannulation. Recent large series of robotic MVR performed at experienced centers suggests that this approach is safe and effective at least through mid-term follow-up.Citation19–Citation21
Early results in man
Based on these findings in animal models, a US Food and Drug Administration Investigational Device Exemption-approved phase I safety and feasibility trial was conducted: EVEREST I (Endovascular Valve Edge to Edge Repair Study).Citation22 The trial enrolled 27 patients with at least moderate-to-severe MR (≥3+), of whom 22 were discharged with clips in place. Three patients underwent the percutaneous procedure but did not have a clip left in place due to inadequate reduction of MR (and subsequently underwent elective MVR), while two other patients underwent elective MVR following device malfunctions. Of the 22 patients discharged with clips in place, 14 patients had MR ≤2+ at 1 month; 13/14 patients maintained this improvement at 6 months. Freedom from MVR was 82% (18/22) at 6 months. Freedom from 30-day major adverse events (MAEs) was 85%, with one patient having a stroke and three patients experiencing clip detachment from one leaflet. It is worth noting that the study protocol was modified after the first ten patients to allow multiple clips to be implanted should MR only improve partially after implantation of a single clip; subsequent studies have shown that this technique is most useful in patient with a wide regurgitant jet (vena contracta >7.5 mm).Citation23
A follow-up study, EVEREST II, analyzed 107 patients (including the original EVEREST I patients) in whom the MitraClip procedure was attempted.Citation24,Citation25 These patients either had symptoms or evidence of left ventricular dysfunction with MR ≥3+. By the investigators’ definition of procedural success (MR ≤2+), 74% (79/107) patients underwent successful MitraClip placement. Substantial intraprocedural hemodynamic stability was observed for all patients. The composite primary endpoint of freedom from MR >2+, surgery, or death was 66%, with symptomatic improvement observed in 74% of patients. When examining only patients who underwent a successful procedure, 77% achieved MR ≤2+; 3-year survival was 90.1%, and freedom from surgery was 76.3%. Echocardiographically, at 12 months, annular diameter remained stable in patients with clips. Of note, however, 11 patients did not have a clip implanted due to MR >2+ intraprocedurally after the clip was placed (at which point the clip was removed intraprocedurally), while 17 patients had a clip implanted but still had MR >2+ postprocedure. Among the 32 patients who ended up having MVR following clip attempt, 25 had a planned repair, and 21 underwent successful repair – which the authors interpreted as indicating that clipping did not preclude surgical options. A subsequent analysis of the same 107 patients confirmed this finding.Citation26
Of note, investigators did find evidence for a learning curve as interventionalists accumulated experience with the MitraClip device. In the 2009 EVEREST mid-term study, a decrease in procedure time (transseptal access to guidewire removal) from 231 to 90 minutes was noted over the study period. A group of German investigators similarly noted that decreases in safety events and increases in successful clip placement (ie, with reduction in MR to ≤2+) over the course of the first 75 patients receiving MitraClips.Citation27
Accumulating evidence
In 2011, the first randomized trial comparing the MitraClip device to clipping versus standard MVR was published ().Citation28 Two hundred and seventy-nine patients with predominantly primary ≥3+ MR were randomized in a 2:1 ratio to undergo MitraClip implantation or conventional surgical MVR (either repair or replacement). The composite endpoint of freedom from death, surgery, or >2+ MR at 12 months was achieved in 55% of MitraClip patients versus 73% of surgery patients (P=0.007); the principal driver of this difference was a 20% surgery rate in the MitraClip cohort versus a 2% reoperative rate in the de novo surgery cohort. Surgery patients experienced superior decreases in MR grade, with 76% demonstrating MR ≤1+ compared to 43% of MitraClip patients. Notably, however, among percutaneous patients who experienced an improvement in MR grade immediately after the procedure, these improvements were durable through 24 months of follow-up. Both groups demonstrated similar symptomatic improvements, though surgery patients had a greater decrease in left ventricular end-diastolic volume than did MitraClip patients. MAEs were documented in only 15% of MitraClip patients versus 48% of surgery patients. However, the definition of MAEs in this trial included transfusion of ≥2 units of blood; excluding this criterion, MAE rates did not differ significantly between groups. The authors concluded that though surgery appeared more effective in treating MR, percutaneous treatment was also effective and safer in a large number of patients and was associated with lower rates of MAEs.
Table 1 Summary of selected studies of percutaneous mitral valve clipping
Given the finding that MitraClips were inferior to surgery but still beneficial to some patients, and safer, a key question was whether or not the use of a MitraClip procedure affected options for surgical correction of MR. Indeed, this was examined in a subsequent study of EVEREST II patients. Of the 107 examined, 32 patients underwent subsequent surgery (23 of whom had at least one clip implanted). This study found that the overall MVR (as opposed to replacement) rate was comparable for patients undergoing MitraClip implantation versus de novo MVR.Citation29 However, in 13.5% of patients studied, when a subsequent operation was required, replacement rather than repair had to be performed due to leaflet injury associated with the clip. Unfortunately, this study did not directly address whether the placement of two clips, as opposed to one, impacted the ability to repair the mitral valve during surgery. Small case reports suggest that repair is still possible even after the placement of more than one clip.Citation30,Citation31
Subsequent studies have tended to confirm the EVEREST I and II results. In particular, several studies of “real-world” experience with the MitraClip system have been published with reasonable results. A large European study, the Amsterdam Center for Contemporary European Studies - A Two-Phase Observational Study of the MitraClip System in Europe (ACCESS-EU) prospective nonrandomized trial, found 81.8% survival at 1 year and 78.9% freedom from MR ≥3+.Citation32 Data from the Getting Reduction of Mitral Insufficiency by Percutaneous Clip Implantation (GRASP) registry at 30 days and 1 year show promising results: freedom from the same composite endpoint of death, surgery, or MR ≥3+ in 75.8% of 117 treated patients at 1 year (with no operations occurring), and a 3.4% MAE rate at 30 days.Citation33 These data also failed to show any differences in safety or outcomes when comparing patients with degenerative versus functional MR. A recent meta-analysis reviewing 16 studies came to similar conclusions, documenting a low adverse event profile (with blood transfusions accounting for the majority of MAEs) and only 14.7% of patients demonstrating MR ≥3+ at 1 year.Citation34 Most recently, in the largest series of MitraClip-treated patients published to date (749 patients with 1-year follow-up), data from the German transcatheter mitral valve interventions registry demonstrated 79.7% 1-year survival among all patients (as opposed to EVEREST II, in which MR was predominantly primary in etiology), as well as a decreased rate of hospital readmission for heart failure.Citation35 Unfortunately, this excellent study did not include echocardiographic follow-up at 1-year.
MitraClip use in high-risk and other populations
Given the perceived attractiveness of a percutaneous approach over MVR in high-risk patients, the MitraClip investigators published a study examining 1-year results of EVEREST II patients deemed at high surgical risk.Citation36 This study was logical given the finding on subgroup analysis in EVEREST II that surgery and percutaneous clipping had equivalent outcomes for patients aged 70 and older.Citation28 Patients selected had MR ≥3+ as well as Society of Thoracic Surgeons predicted operative mortality rate of ≥12%. In this High Risk Study, 78 patients were enrolled; 75 had a clip implanted and 75% (56/75) achieved MR ≤2+. Eighty-nine percent of patients were New York Heart Association III/IV functional class preintervention; this improved to 74% being NYHA I/II postclipping. (Though not available in this EVEREST cohort, a study of similar high-risk patients also demonstrated that these individuals experience marked declines in pro-brain natriuretic peptide at 6 and 12 months.)Citation37 No patients received surgery over 12 months of follow-up, and 75.4% were alive at 1 year compared to 55.3% of patients in a retrospective comparator group with similar degrees of MR and predicted surgical risks managed medically. As with prior studies, favorable left ventricular remodeling was observed, and MAEs occurred in 26.9% of patients through 30 days (21/78; 14 of these were blood transfusions ≥2 units). A 45% reduction in hospitalization rates from congestive heart failure was also documented following successful Mitra-Clip implantation (reduction to MR ≤2+) among surviving EVEREST High Risk Registry patients compared to matched controls.Citation36,Citation38 Given the poor natural history of these patients’ disease, the authors concluded that MitraClip therapy was safe and effective in this high-risk population, particularly considering the absence of other viable therapeutic options. A similar analysis of very high-risk patients with euroSCORE >20 also found evidence for safety and feasibility in this patient population, with a majority of patients demonstrating clinical improvement.Citation37 More recently, a meta-analysis of 12 prospective observational studies confirmed that in high-risk surgical patients, MitraClip implantation is safe and associated with 1-year survival rates in the range of 75%–90%.Citation39
An important question is whether or not MitraClip therapy in high-risk patients simply alleviates symptoms or actually improves survival. Data in surgical patients suggest that the presence of ≥1+ MR is associated with decreased survival following MVR, and even elimination of MR in high-risk surgical patients undergoing MVR has not been conclusively associated with improved survival.Citation40,Citation41 Additionally, as with the surgical Alfieri edge-to-edge MVR, the lack of an annuloplasty when employing the MitraClip may be problematic and explain the progression of MR in some patients. Data on the long-term results of MitraClip therapy in high-risk patients has yet to emerge.
The MitraClip has also been tested and shown to be safe and at least modestly beneficial in several other patient sub-populations. In addition to several trials underway in patients with functional MR (see later), one recent study of 60 patients treated with MitraClip compared to 60 patients managed medically revealed survival of 98.3% in the percutaneous therapy group compared to 89.7% in the MitraClip group at 1 year; at 3 years, these figures were 61.4% versus 34.9% (P=0.007).Citation42 Seventy-two percent of patients achieved MR ≤2+ postprocedure and maintained it through 12 months of follow-up. Other patient populations studied include: patients with renal impairment (a strong predictor of early mortality)Citation43,Citation44 and patients with ≥3+ MR and left ventricular dyssynchrony nonresponsive to cardiac resynchronization therapy.Citation45
MitraClip use in functional versus degenerative MR
The role of MitraClip therapy in patients with functional, as opposed to degenerative, MR remains unclear. This is an important distinction, as patients with functional MR have worse outcomes following surgery compared to degene rative MR.Citation46 Interestingly, MVR and replacement appeared to have equivalent outcomes for functional MR patients in a recent randomized trial, despite earlier data suggesting superior outcomes for repair.Citation47 However, an excess incidence of recurrent MR was noted at 1-year among patients undergoing MVR, raising the possibility that outcomes following MitraClip therapy may vary based on MR etiology. These data compare with the generally suboptimal outcomes of the Alfieri double-orifice repair without annuloplasty (which is most analogous to MitraClip therapy).Citation40 Patients with functional MR undergoing surgery seem to fare better with an undersized annuloplasty added to Alfieri’s techinique.Citation48
To date, no randomized trial data have adequately addressed this issue. Initial studies lacked patients with this MR etiology. Only about one-quarter of patients in the EVEREST II randomized trial had functional MR; in contrast, 77.1% of patients in ACCESS-EU had functional MR. Though MitraClip therapy was inferior to surgery for patients overall in ACCESS-EU, a secondary intention-to-treat analysis showed that surgery was nonsuperior in patients with functional MR.Citation32 Similar to ACCESS-EU, about three-quarters of patients in the GRASP registry (Grasso et al)Citation33 data had functional MR, and no significant differences were noted in primary efficacy end points between the two disease etiologies. Even among patients with the highest predicted surgical risks, no significant differences in outcome were seen between functional versus degenerative MR patients.Citation36 At least one other small series has confirmed these findings.Citation49 Two ongoing randomized trials (discussed later) will help clarify this important issue.
Currently approved indications in the US
In the US, Abbot Vascular’s MitraClip system is currently approved by the Food and Drug Administration for patients with degenerative MR ≥3+ and symptoms (New York Heart Association functional class III or IV) who meet prohibitive risk criteria (30-day Society of Thoracic Surgeons predicted operative mortality risks of ≥8% for planned mitral valve replacement, or ≥6% for planned MVR; porcelain aorta; frailty; hostile chest; severe liver disease or cirrhosis; severe pulmonary hypertension with pressures two-thirds of systemic; as well as a list of unusual extenuating circumstances).Citation50 A patient’s comorbidities must not preclude the expected benefit of reducing MR to ≤2+.
Ongoing trials
Several ongoing trials will help clarify the role of MitraClip therapy in the treatment of functional MR. The COAPT trial (Clinical Outcomes Assessment of MitraClip Percutaneous Therapy), a prospective, randomized, parallel controlled study, is currently enrolling patients with ≥3+ functional MR and heart failure (LVEF 20%–50%). A similar study, the RESHAPE-HF trial (Randomized Study of the MitraClip Device in Heart Failure Patients With Clinically Significant Functional Mitral Regurgitation), is enrolling patients with ≥3+ functional MR and LVEF 15%–40% deemed nonsurgical candidates who will be randomized to MitraClip therapy versus medical management.
Limitations of the MitraClip system
The present MitraClip device does not address all of the aspect of mitral valve dysfunction resulting in MR. In particular, though it can improve leaflet coaptation, it cannot address the mitral annulus (as can be done surgically by suturing a ring in place to provide annular stabilization), nor can it address problems with the chordae tendinae (as can be done with PTFE neochordae). Though a number of technologies designed to improve annular geometry (eg, by placing a wire in the coronary sinus, which runs just posterior and lateral to the mitral annulus) or address chordal problems are under development, none have combined all the elements available to the surgeon in a single device.
Conclusion
As a logical extension of the Alfieri edge-to-edge MVR technique, the MitraClip percutaneous MVR technique has emerged as an option for mitral repair in high-risk surgical patients. Data from a variety of sources demonstrate that though the MitraClip system is less effective than surgical MVR intervention in most patients, it remains a safe alternative, which usually does not preclude future surgical options to address MR. In high-risk patients who are poor operative candidates, MitraClip has a favorable safety profile and can improve both the degree of MR and symptoms in the majority of patients in whom it is utilized. Ongoing trials will help to clarify the impact of MitraClip therapy on symptoms versus long-term survival among high-risk patients, as well as its role as a therapy in other patient populations, such as those with functional MR. The learning curve associated with MitraClip implantation suggests this therapy should be performed in centers of excellence with recognized surgical and structural expertise in mitral valve pathologies. In the future, effective percutaneous therapies for MR will have to incorporate features readily accomplished in open heart surgery, such as annular stabilization and repair of the subvalvular apparatus as needed. Reduction in MR to zero or trace will be requisite before percutaneous MVR can be considered a viable and equivalent alternative to surgery.
Acknowledgments
JTM is the Irene Piccinini Investigator in Cardiac Surgery Research at Johns Hopkins. TCC is the Hugh Sharp Fellow in Cardiac Surgery Research at Johns Hopkins.
Disclosure
The authors report no conflicts of interest in this work.
References
- BlockPCPercutaneous mitral valve repair for mitral regurgitationJ Interv Cardiol2003161939612664822
- Enriquez-SaranoMSchaffHVOrszulakTATajikAJBaileyKRFryeRLValve repair improves the outcome of surgery for mitral regurgitation. A multivariate analysisCirculation1995914102210287850937
- MossRRHumphriesKHGaoMOutcome of mitral valve repair or replacement: a comparison by propensity score analysisCirculation2003108Suppl 1II90II9712970215
- DelocheAJebaraVARellandJYValve repair with Carpentier techniques. The second decadeJ Thorac Cardiovasc Surg19909969901001 discussion 1001–10022359339
- CarpentierACardiac valve surgery–the “French correction”J Thorac Cardiovasc Surg19838633233376887954
- MaisanoFTorraccaLOppizziMThe edge-to-edge technique: a simplified method to correct mitral insufficiencyEur J Cardiothorac Surg1998133240245 discussion 245–2469628372
- MaisanoFSchreuderJJOppizziMFioraniBFinoCAlfieriOThe double-orifice technique as a standardized approach to treat mitral regurgitation due to severe myxomatous disease: surgical techniqueEur J Cardiothorac Surg200017320120510758376
- St GoarFGFannJIKomtebeddeJEndovascular edge-to-edge mitral valve repair: short-term results in a porcine modelCirculation2003108161990199314530193
- FannJISt GoarFGKomtebeddeJBeating heart catheter-based edge-to-edge mitral valve procedure in a porcine model: efficacy and healing responseCirculation2004110898899315302782
- GillinovAMCosgroveDMMitral valve repair for degenerative diseaseJ Heart Valve Dis200211Suppl 1S15S2011843514
- MihaileanuSMarinoJPChauvaudSLeft ventricular outflow obstruction after mitral valve repair (Carpentier’s technique). Proposed mechanisms of diseaseCirculation1988783 Pt 2I781843409521
- SeeburgerJKuntzeTMohrFWGore-tex chordoplasty in degenerative mitral valve repairSemin Thorac Cardiovasc Surg200719211111517870004
- DavidTEArtificial chordaeSemin Thorac Cardiovasc Surg200416216116815197692
- SalvadorLMironeSBianchiniRA 20-year experience with mitral valve repair with artificial chordae in 608 patientsJ Thorac Cardiovasc Surg200813561280128718544371
- KobayashiJSasakoYBandoKMinatoyaKNiwayaKKitamuraSTen-year experience of chordal replacement with expanded polytetra-fluoroethylene in mitral valve repairCirculation200010219 Suppl 3III30III3411082358
- FalkVSeeburgerJCzeslaMHow does the use of polytetrafluoroethylene neochordae for posterior mitral valve prolapse (loop technique) compare with leaflet resection? A prospective randomized trialJ Thorac Cardiovasc Surg200813651205 discussion 1205–120619026803
- SeeburgerJFalkVBorgerMAChordae replacement versus resection for repair of isolated posterior mitral leaflet prolapse: a egaliteAnn Thorac Surg20098761715172019463584
- SeeburgerJBorgerMADollNComparison of outcomes of minimally invasive mitral valve surgery for posterior, anterior and bileaflet prolapseEur J Cardiothorac Surg200936353253819464911
- YooJSKimJBJungSHMitral durability after robotic mitral valve repair: analysis of 200 consecutive mitral regurgitation repairsJ Thorac Cardiovasc Surg201414862773277925173122
- RamzyDTrentoAChengWThree hundred robotic-assisted mitral valve repairs: the Cedars-Sinai experienceJ Thorac Cardiovasc Surg2014147122823524199760
- MurphyDAMossEBinongoJThe expanding role of endoscopic robotics in mitral valve surgery: 1,257 consecutive proceduresAnn Thorac Surg2015100516751681 discussion 1681–168226296272
- FeldmanTWassermanHSHerrmannHCPercutaneous mitral valve repair using the edge-to-edge technique: six-month results of the EVEREST Phase I Clinical TrialJ Am Coll Cardiol200546112134214016325053
- Alegria-BarreroEChanPHFoinNConcept of the central clip: when to use one or two MitraClips(R)EuroIntervention20149101217122423764890
- FeldmanTKarSRinaldiMPercutaneous mitral repair with the MitraClip system: safety and midterm durability in the initial EVEREST (Endovascular Valve Edge-to-Edge REpair Study) cohortJ Am Coll Cardiol200954868669419679246
- MauriLGargPMassaroJMThe EVEREST II Trial: design and rationale for a randomized study of the evalve mitraclip system compared with mitral valve surgery for mitral regurgitationAm Heart J20101601232920598968
- ArgenzianoMSkipperEHeimansohnDSurgical revision after percutaneous mitral repair with the MitraClip deviceAnn Thorac Surg20108917280 discussion p. 8020103209
- SchillingerWAthanasiouTWeickenNImpact of the learning curve on outcomes after percutaneous mitral valve repair with MitraClip and lessons learned after the first 75 consecutive patientsEur J Heart Fail201113121331133922024027
- FeldmanTFosterEGlowerDDPercutaneous repair or surgery for mitral regurgitationN Engl J Med2011364151395140621463154
- GlowerDAilawadiGArgenzianoMEVEREST II randomized clinical trial: predictors of mitral valve replacement in de novo surgery or after the MitraClip procedureJ Thorac Cardiovasc Surg20121434 SupplS60S6322423604
- GeidelSOstermeyerJLassMSchmoeckelMComplex surgical valve repair after failed percutaneous mitral intervention using the MitraClip deviceAnn Thorac Surg201090127727920609795
- RogersJHYeoKKCarrollJDLate surgical mitral valve repair after percutaneous repair with the MitraClip systemJ Card Surg200924667768119682161
- MaisanoFFranzenOBaldusSPercutaneous mitral valve interventions in the real world: early and 1-year results from the ACCESS-EU, a prospective, multicenter, nonrandomized post-approval study of the MitraClip therapy in EuropeJ Am Coll Cardiol201362121052106123747789
- GrassoCCapodannoDScanduraSOne- and twelve-month safety and efficacy outcomes of patients undergoing edge-to-edge percutaneous mitral valve repair (from the GRASP Registry)Am J Cardiol2013111101482148723433761
- VakilKRoukozHSarrafMSafety and efficacy of the MitraClip(R) system for severe mitral regurgitation: a systematic reviewCatheter Cardiovasc Interv201484112913624323764
- PulsMLubosEBoekstegersPOne-year outcomes and predictors of mortality after MitraClip therapy in contemporary clinical practice: results from the German transcatheter mitral valve interventions registryEur Heart J201637870371226614824
- WhitlowPLFeldmanTPedersenWRAcute and 12-month results with catheter-based mitral valve leaflet repair: the EVEREST II (Endovascular Valve Edge-to-Edge Repair) High Risk StudyJ Am Coll Cardiol201259213013922222076
- NeussMSchauTSchoeppMPatient selection criteria and midterm clinical outcome for MitraClip therapy in patients with severe mitral regurgitation and severe congestive heart failureEur J Heart Fail201315778679523325017
- WhitlowPPercutaneous edge-to-edge evalve mitral evalve mitral valve repair in the US “High Risk” Registry, in Trancatheter Cardiovascular Therapeutics (TCT) meeting2009San Francisco, CA
- Munkholm-LarsenSWanBTianDHA systematic review on the safety and efficacy of percutaneous edge-to-edge mitral valve repair with the MitraClip system for high surgical risk candidatesHeart2014100647347823813844
- MaisanoFCaldarolaABlasioADe BonisMLa CannaGAlfieriOMidterm results of edge-to-edge mitral valve repair without annuloplastyJ Thorac Cardiovasc Surg200312661987199714688717
- WuAHAaronsonKDBollingSFPaganiFDWelchKKoellingTMImpact of mitral valve annuloplasty on mortality risk in patients with mitral regurgitation and left ventricular systolic dysfunctionJ Am Coll Cardiol200545338138715680716
- GianniniCFiorelliFDe CarloMComparison of percutaneous mitral valve repair versus conservative treatment in severe functional mitral regurgitationAm J Cardiol2015117227127726651454
- SchuelerRNickenigGMayAEPredictors for short-term outcomes of patients undergoing transcatheter mitral valve interventions: analysis of 778 prospective patients from the German TRAMI registry focusing on baseline renal function. EuroInterventionEpub20159811 (5).
- Estevez-LoureiroRSettergrenMPighiMEffect of advanced chronic kidney disease in clinical and echocardiographic outcomes of patients treated with MitraClip systemInt J Cardiol2015198758026156318
- SeifertMSchauTSchoeppMAryaANeussMButterCMitraClip in CRT non-responders with severe mitral regurgitationInt J Cardiol20141771798525499346
- JensenHJensenMONielsenSLSurgical treatment of functional ischemic mitral regurgitationJ Heart Valve Dis2015241304226182617
- AckerMAParidesMKPerraultLPMitral-valve repair versus replacement for severe ischemic mitral regurgitationN Engl J Med20143701233224245543
- De BonisMLapennaELa CannaGMitral valve repair for functional mitral regurgitation in end-stage dilated cardiomyopathy: role of the “edge-to-edge” techniqueCirculation20051129 SupplI40240816159854
- BraunDLesevicHOrbanMPercutaneous edge-to-edge repair of the mitral valve in patients with degenerative versus functional mitral regurgitationCatheter Cardiovasc Interv201484113714624323541
- GroupAMitraClip Transcatheter Mitral Valve Repair: Frequently Asked Questions201512192015 Available from: http://www.mitraclip.com/hcp/faqs