
Abstract
Objective
The aim of this study was to explore the amplitude of spontaneous brain activity fluctuations in patients with relapsing–remitting multiple sclerosis (RRMS) using the amplitude of low-frequency fluctuation (ALFF) method.
Methods
ALFF and SPM8 were utilized to assess alterations in regional spontaneous brain activities in patients with RRMS in comparison with healthy controls (HCs). The beta values of altered brain regions between patients with RRMS and HCs were extracted, and a receiver operating characteristic (ROC) curve was generated to calculate the sensitivities and specificities of these different brain areas for distinguishing patients with RRMS from HCs. Pearson correlation analyses were applied to assess the relationships between the beta values of altered brain regions and disease duration and Expanded Disability Status Scale (EDSS) score.
Patients and participants
A total of 18 patients with RRMS (13 females; five males) and 18 sex-, age-, and education-matched HCs (14 females; four males) were recruited for this study.
Measurements and results
Compared with HCs, patients with RRMS showed higher ALFF responses in the right fusiform gyrus (Brodmann area [BA] 37) and lower ALFF responses in the bilateral anterior cingulate cortices (BA 24 and 32), bilateral heads of the caudate nuclei, and bilateral brainstem. The ROC analysis revealed that the beta values of these abnormal brain areas showed high degrees of sensitivity and specificity for distinguishing patients with RRMS from HCs. The EDSS score showed a significant negative Pearson correlation with the beta value of the caudate head (r=−0.474, P=0.047).
Conclusion
RRMS is associated with disturbances in spontaneous regional brain activity in specific areas, and these specific abnormalities may provide important information about the neural mechanisms underlying behavioral impairment in RRMS.
Introduction
Multiple sclerosis (MS) is a neurodegenerative disorder that is characterized by motor dysfunction and disseminated axonal degeneration as well as inflammatory demyelination in the central nervous system. MS is an autoimmune demyelinating disease of the central nervous system. While demyelination is the hallmark of relapsing–remitting subtype, neurodegeneration is believed to be the hallmark of progressive forms. In addition, there is a growing consensus on a partly independent occurrence of demyelination and neurodegeneration even at early stages of MS, the link between both processes being synaptotoxicity. Typically, the extent of motor dysfunction is relative to the extent of white matter (WM) and gray matter (GM) damage.Citation1,Citation2 The extensive involvement of disease-related cortical GM organization may delay and perturb syntonic intrinsic signals across cortico–cortical and cortico–subcortical circuits and underlie several nonmotor clinical manifestations of MS such as fatigue, sensorimotor deficits, and cognitive dysfunction.Citation2 However, the neurological basis of the role of WM and GM damage in these manifestations of MS remains unclear.
Brain imaging has facilitated the noninvasive exploration of MS-related pathology.Citation3–Citation5 However, previous functional magnetic resonance imaging (fMRI) studies have traditionally focused on task-evoked neuronal activity. Because different performance and task patterns make it difficult to interpret biological mechanisms of disease and hinder between-study comparisons, it has been difficult to achieve a consensus regarding the nature of MS-related abnormalities in brain regions, including the anterior cingulate cortex, inferior parietal lobule, basal ganglia, thalamus, and cerebellum.Citation6–Citation9
It has been reported that synchronous neuronal activity is conducive to information coordination and integration processing;Citation10 in one study, the interruption of synchronous activity was proposed to mediate cognitive dysfunction by inducing deterioration of the efficiency and speed of information processing.Citation11 Resting-state fMRI (RS-fMRI) is a useful tool for the mechanistic investigation of brain diseases; RS-fMRI can accurately localize neural activities, does not require the use of a radioactive tracer, and has been applied to detect alterations in regional brain activity.Citation12 In contrast to magnetoencephalography and conventional electrophysiological methods, RS-fMRI has the capacity to map neuronal activity with high spatial resolution. Beyond detecting regional changes in brain activity, RS-fMRI also provides important information on the architecture and interconnectivity of distributed brain networks, notably by measuring patterns of spontaneous fluctuations.
Previous applications of fMRI in MS have limited analyses to specific regions of interest and were not designed to detect activation changes across the entire brain.Citation13 Functional connectivity analyses using RS-fMRI permit the investigation of intrinsic brain activity across the whole brain and allow the identification of network connectivity between distant brain regions,Citation14 especially in the default mode network (DMN).Citation15 However, the results of abnormal functional connectivity between two remote areas do not allow for the determination of which brain area has abnormal spontaneous activity.Citation16
The amplitude of low-frequency fluctuation (ALFF), an important component of RS-fMRI, is integrated in a low-frequency range and has been used to identify brain areas showing disturbances in blood-oxygen-level-dependent (BOLD) signal.Citation17,Citation18 Previously, it was shown that ALFF index measurements were highly reproducible with scan intervals up to 1 year in chronic and stable schizophrenia patients as well as healthy controls (HCs).Citation19 Zuo et alCitation20 also indicated a high degree of test–retest reliability for spontaneous low-frequency fluctuations within a low-frequency range and within four defined sections of narrow low-frequency bands. Indications of high test–retest reliability for the ALFF method makes this method a convenient and reliable index for RS-fMRI data analysis, with utility for the exploration of regional spontaneous brain activity abnormalities in various brain diseases.Citation16 Recently, ALFF indices have been successfully employed for the study of sleep deprivation,Citation12,Citation21 primary insomnia,Citation16 and obstructive sleep apnea.Citation22 However, no study to date has evaluated disturbances in spontaneous regional brain activity in patients with relapsing–remitting MS (RRMS). In the current study, we used the ALFF method as an index to explore local functional alterations of regional brain activity in patients with RRMS relative to HCs. Moreover, we examined correlations between these findings and disability scores to evaluate the relevance of ALFF indices to the clinical manifestation of RRMS.
Patients and methods
Subjects
A total of 18 patients with RRMS (five males and 13 females; mean age, 35±10.68 years; mean education, 9.22±4.21 years) diagnosed according to the McDonald’s diagnostic criteria were recruited for this study. Prior to magnetic resonance imaging (MRI) examination, all subjects underwent a thorough physical examination using the Expanded Disability Status Scale (EDSS)Citation23 conducted by an experienced neurologist. EDSS scores ranged from 0 to 10, where 0 indicated normal status and higher scores indicated more severe degrees of disability.
All subjects were right handed as measured by the Edinburgh inventory. The inclusion criteria for patients with RRMS were as follows: 1) mild-to-moderate disability (EDSS ≤5) to prevent the inclusion of confounding factors; 2) the absence of corticosteroid therapy or clinical relapse for at least 1 month prior to the study and during the study; 3) the absence of any sleep disorders or other psychiatric disorders according to the DSM-IV; and 4) the absence of evidence for any brain tumor, brain injury, or intracerebral hemorrhage on conventional MRI. Disease duration was recorded as the number of months from initial symptom onset date until the study MRI scan date. The mean disease duration in this study was 28.52±38.83 months. Demographic and clinical characteristics of the included patients with RRMS are presented in .
Table 1 Demographics and clinical characteristics
A total of 18 age-, sex-, and education-matched HCs (four males and 14 females; mean age, 35.17±10.97 years; mean education, 10.72±3.95 years) were recruited for this study. HCs had no history of neurological or psychiatric disorders, alcohol or drug abuse, sleep disorders, systemic illness, brain tumor, brain injury, or intracerebral hemorrhage. The study was approved by the Human Research Ethics Committee of the Affiliated Hospital of Zunyi Medical University. The purpose, potential risks, and methods of this study were explained to all subjects, and all subjects voluntarily provided informed consent form prior to study participation.
Parameters
MRI examinations were conducted using a 3 T magnetic resonance scanner (GE, USA) with the subject in a supine position. Three-dimensional T1-weighted images were collected with a gradient-recalled echo (GRE) sequence in a sagittal position. The parameters were as follows: repetition time =3,000 ms, thickness =1.0 mm, echo time =7.8 ms, gap =0 mm, field of view =256×256 mm, acquisition matrix =256×256, and flip angle =15°. Finally, 210 functional images with 33 axial slices that covered the whole brain were collected for each subject using a GRE planar imaging pulse sequence. The parameters of the functional session were as follows: repetition time =2,000 ms, thickness =4.0 mm, echo time =30 ms, gap =0 mm, field of view =240×240 mm, and acquisition matrix =64×64, and flip angle =90°.
fMRI data analysis
To exclude defective data, all MRI data were checked using MRIcro software (www.MRIcro.com).Citation24 All MRI data were subjected to a Digital Imaging and Communications in Medicine (DICOM) form transformation. The first ten volumes of RS-fMRI images were discarded for each subject to allow for subject adaptation and account for the instability of initial MRI scanner signal. Using MATLAB2010a (Mathworks, Natick, MA, USA) and SPM8 (http://www.fil.ion.ucl.ac.uk/spm), the remaining 200 volumes were corrected for differences in slice times and were analyzed using Data Processing Assistant for RS-fMRI (DPARSFA; http://rfmri.org/DPARSF) toolbox. The time courses of head motion were collected by calculating the values of rotation (degrees) and translation (millimeter) for each volunteer. Subjects who showed >1.5 mm maximum translation in the x, y, or z planes or >1.5° of angular motion around the x, y, or z axes for any of the 200 volumes were excluded.
Three-dimensional T1-weighted images for each subject were co-registered to the mean of the realigned echo-planar imaging template and then segmented into GM, WM, and cerebrospinal fluid (CSF) using the Diffeomorphic Anatomical Registration Through Exponentiated Lie Algebra (DARTEL) segmentation. All the images were automatically transformed from the individual space into the Montreal Neurological Institute (MNI) space. Because MRI data are sensitive to micro-head motions in rotation (degrees) and translation (millimeter) in any direction (x, y, or z), the Friston 24-Parameter Model was applied to regress out head motion effects from the realigned data.Citation25,Citation26 We further characterized mean frame-wise displacement (FD), which considers voxel-wise differences in motion in its derivation, as a measure of micro-head motion for each subject.
fMRI images were resampled at a resolution of 3×3×3 mm. A linear regression was performed to remove signal from the WM, GM, CSF, mean time series of all voxels across the whole brain, and head motion parameters to minimize confounding factors.Citation27 Of note, global signal was not regressed out as in previous studiesCitation16,Citation28–Citation30 due to the controversial nature of this omission.Citation27,Citation31 The time series for each voxel was temporally band-pass filtered (0.01–0.08 Hz) and linearly detrended to reduce low-frequency drift, cardiac noise, and physiological high-frequency respiratory artifacts. For each subject, we calculated ALFF values at each voxel. The details of the ALFF calculation are described in previous studies.Citation16,Citation22
Receiver operating characteristic (ROC) curve analyses
The ROC curve method has been widely used for identifying and comparing physiological biomarkers. Sensitivity is excellent when the area under the curve (AUC) value ranges from 0.9 to 1, while sensitivity is good when the AUC value is 0.8–0.9, fair when the AUC value is 0.7–0.8, poor if the value is 0.6–0.7, and failed when the value is 0.5–0.6.Citation32,Citation33 In previous studies, the ALFF index showed high degrees of sensitivity and specificity for distinguishing patients from HCs and may be useful for detecting early biological indicators of regional brain activity changes.Citation12,Citation16,Citation22
Since different brain areas may have different utility for distinguishing patients with RRMS from the HCs,Citation22 we extracted the beta values of brain areas of interest and used them to explore whether changes in these specific areas have the ability to distinguish patients with RRMS from HCs.
Brain–behavior correlations
Based on ALFF findings, the beta values of specific brain areas in patients with RRMS were extracted, and Pearson correlation analyses were applied to assess relationships between disease duration and EDSS score.
Statistical analysis
χ2 tests were used for categorical data, and two-sample t-tests were used for continuous data. The P-value <0.05 was considered to indicate statistically significant differences with two-tailed tests. All statistical analyses of demographic and clinical variables were conducted with IBM SPSS 21.0 software.
For ALFF results, two-sample t-tests were applied to analyze regional brain differences between patients with RRMS and HCs with sex, age, and education as nuisance covariates using SPM8. A corrected individual voxel P<0.01 with cluster size ≥40 was applied to assess statistical differences using an AlphaSim-corrected cluster threshold of P<0.05.
Results
ALFF differences
Compared with HCs, patients with RRMS showed higher ALFF responses in the right fusiform gyrus (Brodmann area [BA] 37) and lower ALFF responses in the bilateral anterior cingulate gyrus (BA 24 and 32), bilateral caudate head, and the cluster of the bilateral brainstem. The details of this analysis are shown in and .
Figure 1 Different regional brain areas between patients with RRMS and HCs.
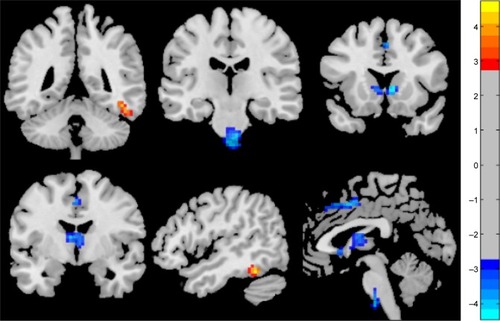
Table 2 Regional ALFF differences in patients with RRMS versus HCs
ROC findings
The mean beta values of specific clusters of interest were extracted and used for ROC curve analyses (). ROC analyses revealed that, among ALFF areas of interest, one showed an excellent AUC value, two showed good AUC values, and one showed a fair AUC value. Further diagnostic analyses demonstrated that the mean beta values of these areas demonstrated high degrees of sensitivity and specificity. These findings indicate that regional ALFF indices could serve as good-to-excellent markers for distinguishing patients with RRMS from HCs. The details of these analyses are presented in and .
Figure 2 Beta values of different ALFF brain areas.
Abbreviations: ALFF, amplitude of low-frequency fluctuation; HCs, healthy controls; MS, multiple sclerosis; RRMS, relapsing–remitting MS.
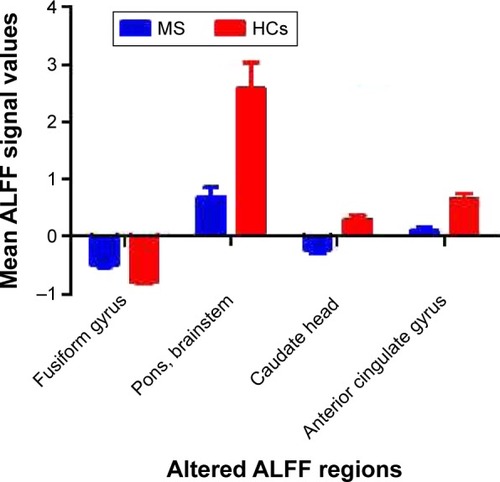
Figure 3 Sensitivity and specificity of mean beta values of different brain areas.
Abbreviation: ROC, receiver operating characteristic.
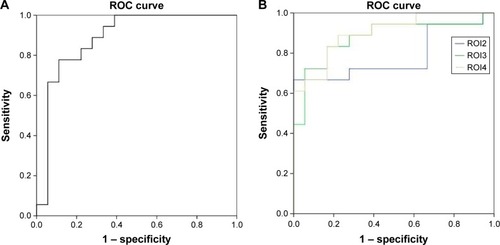
Table 3 ROC curve analysis for different ALFF areas between RRMS and HCs
Pearson correlation analysis
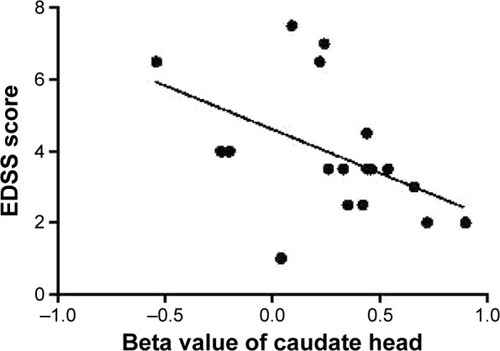
In this study, EDSS score showed a significant negative Pearson correlation with the beta value of the caudate head (r=−0.474, P=0.047) as shown in . There were no significant correlations between the beta values of different ALFF clusters and disease duration (P>0.05) or between EDSS score and any other ALFF cluster beta value (P>0.05).
Figure 4 Pearson correlation between EDSS score and beta value of caudate head.
Discussion
In the current study, we used the RS ALFF method to investigate regional brain differences between patients with RRMS and HCs. We found that patients with RRMS showed higher ALFF responses in the right fusiform gyrus of temporal lobe and lower ALFF responses in the bilateral anterior cingulate gyrus, bilateral caudate head, and the cluster of the bilateral pons and brainstem; moreover, these observations preceded evidence of visible brain lesions on conventional MRI. Further, an ROC analysis indicated that ALFF areas of interest could effectively discriminate patients with RRMS from HCs with high degrees of sensitivity and specificity. Overall, these findings indicate that the ALFF method is useful for characterizing the neural mechanisms underlying RRMS and may be capable of detecting early biological indicators of RRMS, ie, alterations in the brain activity of relevant regions.
Previous studies have identified abnormal baseline brain activity prior to the appearance of brain lesions on T2-weighted imaging in RRMS.Citation34 Other studies comparing patients with MS to HCs have shown, in addition to abnormal regional brain activity, alterations in fractional anisotropy values, mean diffusivity values, and functional connectivity in several brain areas, including the thalamus, visual system, motor system, and areas related to advanced cognitive function.Citation35–Citation42 In support of these findings, the current study identified the abovementioned differences in ALFF responses between patients with RRMS and HCs. Another previous study found smaller GM volumes in the left frontotemporal cortex, bilateral caudate nuclei, and bilateral anterior cingulate gyrus in patients with RRMS versus HCs and furthermore identified selective correlations between these brain areas and the lesion load of caudate atrophy.Citation43 In the current study, we found that EDSS score was negatively correlated with the beta value of the caudate head (r=−0.474, P=0.047). These findings provide a novel insight into the pathogenic mechanism of RRMS which, in particular, highlights the role of the caudate nucleus.
The basal ganglia play a role in both motor and advanced cognitive function. Some evidence suggests that cardiorespiratory fitness is associated with the GM volume of the basal ganglia.Citation44,Citation45 In line with this hypothesis, patients with MS with higher levels of cardiorespiratory fitness were shown to have larger basal ganglia volumes, including in the caudate, putamen, and pallidum.Citation46 The progressive decline of anterograde memory function has been increasingly recognized as a frequent symptom in chronic MS. Previous studies have demonstrated an association between MS and poor cognitive performances,Citation42,Citation47 and pediatric patients with MS were shown to have early maladaptive plasticity contributing to cognitive impairments.Citation48 Accordingly, increasing evidence exists for the beneficial effects of aerobic exercise training on motor and cognitive outcomes in MS and on the volumes of basal ganglia components.Citation49,Citation50 In support of this concept, our study identified low ALFF responses in the bilateral caudate head in patients with RRMS, which is consistent with the previous finding that the normalized bicaudate volume was 19% lower in patients with RRMS relative to HCs.Citation51 Overall, these findings suggest that caudate pathology underlies impairments in cognitive performance in RRMS and that cardiorespiratory fitness should be an important therapeutic goal to address these deficits.
Purely intracortical lesions represent up to 24% of the total lesion load in MS,Citation52 with lesions also occurring in the cingulate gyrusCitation53 associated with axonal transection, demyelination, apoptotic loss of neurons, and dendritic transection.Citation54 Brainin et alCitation55 showed extensive lesions in the WM of the anterior cingulate gyrus in patients with MS, whereas Terroni et alCitation56 found that cingulate cortex dysfunction was an important factor related to working memory impairments in patients with stroke. Abnormal functional connectivity between the hippocampus and the thalamus, anterior cingulate gyrus, and prefrontal cortex has already been identified and related to impaired spatial memory function in patients with MS.Citation57 Accordingly, dysfunction of the bilateral anterior cingulate gyrus may underlie the impairments in working memory in patients with MS.
Conclusion
Our study demonstrated that ALFF indices in key brain regions may serve as early biological indicators of abnormal regional spontaneous brain activity in RRMS, which is observed prior to visible brain lesions on conventional MRI. The current study provided important information in order to understand the underlying neural mechanisms of RRMS pathology, and also provided insights into the relationship between RRMS and abnormal baseline brain activity and can serve as a reference for task-related fMRI studies to enable a more comprehensive understanding of the pathophysiology of RRMS. However, we did not use fatigue or other measures in the assessment; future studies should perform more measures to assess the clinical characteristics of the RRMS.
Acknowledgments
This work was supported by grants from the Science and Technology Department of Guizhou Province (qiankehe J zi LKZ [2012] No 22).
Disclosure
The authors report no conflicts of interest in this work.
References
- VercellinoMMaseraSLorenzattiMDemyelination, inflammation, and neurodegeneration in multiple sclerosis deep gray matterJ Neuropathol Exp Neurol200968548950219525897
- MinagarABarnettMHBenedictRHThe thalamus and multiple sclerosis modern views on pathologic, imaging, and clinical aspectsNeurology2913802210219
- NelsonFAkhtarMAZúñigaENovel fMRI working memory paradigm accurately detects cognitive impairment in multiple sclerosisMult Scler Epub201699
- KhavariRKarmonikCShyMFletcherSBooneTFunctional magnetic resonance imaging with concurrent urodynamic testing identifies brain structures involved in micturition cycle in patients with multiple sclerosisJ Urol Epub2016921
- FilippiMRovarisMRoccaMAImaging primary progressive multiple sclerosis: the contribution of structural, metabolic, and functional MRI techniquesMult Scler201410Suppl 1S36S44
- TintoreMRoviraAMRI criteria distinguishing seropositive NMO spectrum disorder from MSNeurology20138014133623486884
- BakshiRThompsonAJRoccaMAMRI in multiple sclerosis: current status and future prospectsLancet Neurol20087761562518565455
- FilippiMRoccaMAFunctional MR imaging in multiple sclerosisNeuroimaging Clin N Am2009191597019064200
- FilippiMRiccitelliGMattioliFMultiple sclerosis: effects of cognitive rehabilitation on structural and functional MR imaging measures-an explorative studyRadiology2012262393294022357892
- BuzsakiGDraguhnANeuronal oscillations in cortical networksScience200430456791926192915218136
- ZhangZLiuYJiangTAltered spontaneous activity in Alzheimer’s disease and mild cognitive impairment revealed by regional homogeneityNeuroimage20125921429144021907292
- DaiXJLiuCLGongHHLong-term sleep deprivation decreases the default spontaneous activity and connectivity pattern in healthy male subjects: a resting-state fMRI studyNeuropsychiatr Dis Treat20151176177225834451
- WegnerCFilippiMKortewegTRelating functional changes during hand movement to clinical parameters in patients with multiple sclerosis in a multi-centre fMRI studyEur J Neurol200815211312218217881
- GreiciusMDSupekarKMenonVDoughertyRFResting state functional connectivity reflects structural connectivity in the default mode networkCereb Cortex2009191727818403396
- BucknerRAndrews-HannaJSchacterDThe brain’s default network: anatomy, function, and relevance to diseaseAnn N Y Acad Sci2008112413818400922
- DaiXJNieXLiuXGender differences in regional brain activity in patients with chronic primary insomnia: evidence from a resting-state fMRI studyJ Clin Sleep Med201612336337426715399
- ZangYFHeYZhuCZAltered baseline brain activity in children with ADHD revealed by resting-state functional MRIBrain Dev2007292839116919409
- LuHZuoYGuHSynchronized delta oscillations correlate with the resting-state functional MRI signalProc Natl Acad Sci U S A200710446182651826917991778
- TurnerJAChenHMathalonDHReliability of the amplitude of low-frequency fluctuations in resting state fMRI in chronic schizophreniaPsychiatry Res2012201325325522541511
- ZuoXNDi MartinoAKellyCThe oscillating brain: complex and reliableNeuroimage20104921432144519782143
- DaiXJMinYJGongHHEvaluation of the post-effect of acupuncture at Sanyinjiao (SP 6) under sleep deprivation by resting-state amplitude of low-frequency fluctuation: a fMRI studyZhongguo Zhen Jiu2012321475222295826
- LiHJDaiXJGongHHNieXZhangWPengDCAberrant spontaneous low-frequency brain activity in male patients with severe obstructive sleep apnea revealed by resting-state functional MRINeuropsychiatr Dis Treat20151120721425653530
- KurtzkeJFRating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS)Neurology19833311144414526685237
- DaiXJGongHHWangYXGender differences in brain regional homogeneity of healthy subjects after normal sleep and after sleep deprivation: a resting-state fMRI studySleep Med201213672072722503940
- SatterthwaiteTDElliottMAGerratyRTAn improved framework for confound regression and filtering for control of motion artifact in the preprocessing of resting-state functional connectivity dataNeuroimage20136424025622926292
- YanCGCheungBKellyCA comprehensive assessment of regional variation in the impact of head micromovements on functional connectomicsNeuroimage20137618320123499792
- FoxMDSnyderAZVincentJLCorbettaMVan EssenDCRaichleMEThe human brain is intrinsically organized into dynamic, anticorrelated functional networksProc Natl Acad Sci U S A2005102279673967815976020
- NieXShaoYLiuSYFunctional connectivity of paired default mode network subregions in primary insomniaNeuropsychiatr Dis Treat2015113085309326719693
- DaiXJPengDCGongHHAltered intrinsic regional brain spontaneous activity and subjective sleep quality in patients with chronic primary insomnia: a resting-state fMRI studyNeuropsychiatr Dis Treat2014102163217525484585
- PengDCDaiXJGongHHLiHJNieXZhangWAltered intrinsic regional brain activity in male patients with severe obstructive sleep apnoea: a resting-state functional magnetic resonance imaging studyNeuropsychiatr Dis Treat2014101819182625278755
- SaadZSGottsSJMurphyKTrouble at rest: how correlation patterns and group differences become distorted after global signal regressionBrain Connect201221253222432927
- HuangXZhongYLZengXJDisturbed spontaneous brain activity pattern in patients with primary angle-closure glaucoma using amplitude of low-frequency fluctuation: a fMRI studyNeuropsychiatr Dis Treat2015111877188326251603
- El KhouliRHMacuraKJBarkerPBHabbaMRJacobsMABluemkeDARelationship of temporal resolution to diagnostic performance for dynamic contrast enhanced MRI of the breastJ Magn Reson Imaging2009305999100419856413
- LiuYMengBZengCAbnormal baseline brain activity in patients with multiple sclerosis with simple spinal cord involvement detected by resting-state functional magnetic resonance imagingJ Comput Assist Tomogr201539686687526466112
- ZhouFZhuangYWuLIncreased thalamic intrinsic oscillation amplitude in relapsing-remittingClin Imaging201438560561024973078
- LiuYDuanYHuangJMultimodal quantitative MR imaging of the thalamus in multiple sclerosis and neuromyelitis opticaRadiology2015277378479226043265
- DogonowskiAMAndersenKWMadsenKHMultiple sclerosis impairs regional functional connectivity in the cerebellumNeuroimage Clin2013413013824371795
- DogonowskiAMSiebnerHRSoelbergPExpanded functional coupling of subcortical nuclei with the motor resting-state network in multiple sclerosisMult Scler201219555956623012251
- LoweMJPhillipsMDLuritoJTMattsonDDzemidzicMMatthewsVPMultiple sclerosis: low-frequency temporal blood oxygen level-dependent fluctuations indicate reduced functional connectivity initial resultsRadiology2002224118419212091681
- RoosendaalSDSchoonheimMMHulstHEResting state networks change in clinically isolated syndromeBrain2010133Pt 61612162120356855
- RoccaMAValsasinaPAbsintaMDefault-mode network dysfunction and cognitive impairment in progressive MSNeurology201074161252125920404306
- HawellekDJHippJFLewisCMCorbettaMEngelAKIncreased functional connectivity indicates the severity of cognitive impairment in multiple sclerosisProc Natl Acad Sci U S A201110847190661907122065778
- PrinsterAQuarantelliMOreficeGGrey matter loss in relapsing-remitting multiple sclerosis: a voxel-based morphometry studyNeuroimage200629385986716203159
- ChaddockLEricksonKIPrakashRSBasal ganglia volume is associated with aerobic fitness in preadolescent childrenDev Neurosci201032324925620693803
- VerstynenTDLynchBMillerDLCaudate nucleus volume mediates the link between cardiorespiratory fitness and cognitive flexibility in older adultsJ Aging Res2012201293928522900181
- MotlRWPiluttiLAHubbardEAWetterNCSosnoffJJSuttonBPCardiorespiratory fitness and its association with thalamic, hippocampal, and basal ganglia volumes in multiple sclerosisNeuroimage Clin2015766166625844320
- SchoonheimMMGeurtsJJLandiDFunctional connectivity changes in multiple sclerosis patients: a graph analytical study of MEG resting state dataHum Brain Mapp2013341526121954106
- CirilloSRoccaMAGhezziAAbnormal cerebellar functional MRI connectivity in patients with paediatric multiple sclerosisMult Scler201622329230126163069
- BatistaSZivadinovRHoogsMBasal ganglia, thalamus and neocortical atrophy predicting slowed cognitive processing in multiple sclerosisJ Neurol2012259113914621720932
- SchoonheimMMPopescuVRueda LopesFCSubcortical atrophy and cognition: sex effects in multiple sclerosisNeurology201279171754176123019265
- BermelRAInnusMDTjoaCWBakshiRSelective caudate atrophy in multiple sclerosis: a 3D MRI parcellation studyNeuroreport200314333533912634479
- KiddDBarkhofFMcConnellRAlgraPRAllenIVReveszTCortical lesions in multiple sclerosisBrain1999122Pt 1172610050891
- BoLVedelerCANylandHITrappBDMorkSJSubpial demyelination in the cerebral cortex of multiple sclerosis patientsJ Neuropathol Exp Neurol200362772373212901699
- PetersonJWBoLMorkSChangATrappBDTransected neurites, apoptotic neurons, and reduced inflammation in cortical multiple sclerosis lesionsAnn Neurol200150338940011558796
- BraininMGoldenbergGAhlersCReisnerTNeuholdADeeckeLStructural brain correlates of anterograde memory deficits in multiple sclerosisJ Neurol198823563623653171618
- TerroniLAmaroEIosifescuDVStroke lesion in cortical neural circuits and post-stroke incidence of major depressive episode: a 4-month prospective studyWorld J Biol Psychiatry201112753954821486107
- RoosendaalSDHulstHEVrenkenHStructural and functional hippocampal changes in multiple sclerosis patients with intact memory functionRadiology2010255259560420413769