
Abstract
Purpose
To explore the potential factors impacting the efficacy of venlafaxine extended release (ER) and treatment differences between 75 mg/day and 75–225 mg/day dose in patients with major depressive disorder (MDD).
Methods
We performed exploratory post hoc subgroup analyses of a randomized, double-blind, placebo-controlled study conducted in Japan. A total of 538 outpatients aged 20 years or older with a primary diagnosis of MDD who experienced single or recurrent episodes were randomized into three groups: fixed-dose, flexible-dose, or placebo. Venlafaxine ER was initiated at 37.5 mg/day and titrated to 75 mg/day for both fixed-dose and flexible-dose group, and to 225 mg/day for flexible-dose group (if well tolerated). Efficacy endpoints were changes from baseline at Week 8 using the Hamilton Rating Scale for Depression–17 items (HAM-D17) total score, Hamilton Rating Scale for Depression–6 items score, and Montgomery–Asberg Depression Rating Scale total score. The following factors were considered in the subgroup analyses: sex, age, HAM-D17 total score at baseline, duration of MDD, duration of current depressive episode, history of previous depressive episodes, history of previous medications for MDD, and CYP2D6 phenotype. For each subgroup, an analysis of covariance model was fitted and the adjusted mean of the treatment effect and corresponding 95% CI were computed. Due to the exploratory nature of the investigation, no statistical hypothesis testing was used.
Results
Venlafaxine ER improved symptoms of MDD compared with placebo in most subgroups. The subgroup with a long duration of MDD (>22 months) consistently showed greater treatment benefits in the flexible-dose group than in the fixed-dose group.
Conclusion
These results suggest that a greater treatment response to venlafaxine ER (up to 225 mg/day) can be seen in patients with a longer duration of MDD. Further investigations are needed to identify additional factors impacting the efficacy of venlafaxine ER.
Introduction
Antidepressant medications such as selective serotonin reuptake inhibitors and serotonin-norepinephrine reuptake inhibitors (SNRIs) are the first-line treatments for patients with moderate to severe major depressive disorder (MDD).Citation1–Citation3 In 1993, venlafaxine was approved by the US Food and Drug Administration as the first SNRI for the treatment of MDD in adults,Citation4 and is now marketed in more than 90 countries. In 2015, venlafaxine extended release (ER) became the third SNRI to receive regulatory approval for the treatment of MDD in Japan, thereby driving interest in data specifically addressing Japanese patients treated with venlafaxine ER.
Higuchi et alCitation5 reported the primary results of an 8-week, double-blind, placebo-controlled, randomized, Phase III study of 538 patients conducted in Japan using fixed-dose (75 mg/day) and flexible doses (75–225 mg/day) of venlafaxine ER. The study findings showed a statistically significant difference in the change from baseline in Hamilton Rating Scale for Depression–17 items (HAM-D17) total scoreCitation6 in the fixed-dose group (−10.76; P=0.031), but not in the flexible-dose group (−10.37; P=0.106), compared with the placebo group (−9.25). However, the flexible-dose group showed statistically significant treatment benefits compared with the placebo group (P<0.05) in several secondary endpoints, such as the Montgomery–Asberg Depression Rating Scale (MADRS)Citation7 and the Hamilton Rating Scale for Depression–6 items (HAM-D6).Citation8,Citation9 An examination of the HAM-D17 revealed poor improvement in sleep disturbance scores (items 4–6)Citation10 for the flexible-dose group after Week 4, possibly due to the norepinephrine effect of venlafaxine at high doses.
Given these results, we performed exploratory post hoc subgroup analyses in order to explore the potential factors that may impact the efficacy of venlafaxine ER and treatment differences between the fixed-dose (75 mg/day) and the flexible-dose (75–225 mg/day) in patients with MDD.
Materials and methods
Study design
The original study was a multicenter, randomized, double-blind, placebo-controlled, parallel-group, Phase III study to evaluate the efficacy and safety of venlafaxine ER 75 mg/day (fixed-dose) and venlafaxine ER 75–225 mg/day (flexible-dose), compared with placebo (ClinicalTrials.gov: NCT01441440).Citation5 After a 2-week screening period, eligible patients were randomized in a 1:1:1 ratio to each treatment group for 8 weeks, followed by a 2-week tapering period.
Subjects
Eligible patients included outpatients aged 20 years or older who had a primary diagnosis of MDD based on criteria of the Diagnostic and Statistical Manual of Mental Disorders, fourth edition, and had experienced single (≥90 days) or recurrent episodes (≥28 days) of depression without psychotic features. At both screening and baseline, patients were required to have scored at least 26 on the MADRS questionnaire and the change in MADRS total score from screening to baseline was required not to have exceeded 25%. Finally, at both screening and baseline, patients were required to have a 16-item Quick Inventory of Depressive Symptomatology self-report version (QIDS16-SR-J)Citation11 total score and a Clinical Global Impressions–Severity scale (CGI-S) score of at least 16 and 4, respectively.
Settings
The original study was conducted at 62 investigational sites from November 2011 to March 2014 in Japan. All applicable documentation including the study protocol was approved by the Institutional Review Board and Independent Ethics Committee at each site (Box S1). The study was conducted in agreement with all legal and regulatory requirements and the International Ethical Guidelines for Biomedical Research Involving Human Subjects (Council for International Organizations of Medical Sciences 2002), Guidelines for Good Clinical Practice, and the Declaration of Helsinki. Written informed consent was provided by all patients before study participation.
Treatment
The details of drug administration and dose titration have been reported elsewhere.Citation5 Initial dose of venlafaxine was 37.5 mg/day. In Week 1, the dose could be increased to 75 mg/day, and in Week 2, based on tolerability, it could be increased to 150 mg/day in the flexible-dose group. Further, in Week 3, the dose was force titrated to 225 mg/day in the flexible-dose group, in spite of an acceptable response at a lower dose. Dose reduction was allowed in case of intolerance to higher doses. We simply compared the point estimates among the subgroups to explore the potential factors that may impact the efficacy of venlafaxine ER and treatment differences between the fixed-dose (75 mg/day) and the flexible-dose (75–225 mg/day) groups.
Assessments
The results of all efficacy endpoints in this study have been previously published.Citation5 In this report, HAM-D17, HAM-D6, and MADRS were used for subgroup analyses. The formula, Σ (items 1, 2, 7, 8, 10, and 13), was used to measure HAM-D6 score.
Statistical analysis
As the current investigation was exploratory in nature, no statistical hypothesis testing was used. The following efficacy endpoints were analyzed: change from baseline at Week 8 in the HAM-D17 total score, HAM-D6 score, and MADRS total score. The following factors were considered for the subgroup analyses: sex (male/female); age (≤37/>37 years [median]); HAM-D17 total score at baseline (total score ≤22/total score >22 [median]); duration of MDD, defined as the duration of MDD since the occurrence of the first episode (≤22 months/>22 months [median], <12 months/≥12 months, and <48 months/≥48 months); duration of the current depressive episode (≤6.6 months/>6.6 months [median]); history of previous depressive episodes (0 [single]/≥1 [recurrence]); history of previous medications for MDD (0 [no medication]/≥1 [medicated]); and CYP2D6 phenotypes (ultra-rapid/extensive and intermediate/poor metabolizers). For each subgroup, an ANCOVA model with the treatment group as a factor and the baseline value of the respective efficacy endpoint as a covariate was fitted. Based on the ANCOVA model, the adjusted mean and its corresponding 95% CI of the treatment effect (defined as a difference from placebo) was computed for each active treatment group.
The full analysis set (FAS) was used throughout the analyses. The FAS was defined as all patients who received at least one dose of the study drug and had baseline measurement and at least one post-baseline measurement of the primary efficacy endpoint was used for the analysis. Missing values in the endpoints at Week 8 were imputed using the last observation carried forward (LOCF) algorithm. Assessments prior to the first dose of the study medication were not eligible to be carried forward.
Results
Patient disposition
Of 538 randomized patients, 537 patients received the study drug (fixed-dose group, 174; flexible-dose group, 179; placebo, 184). Overall, 475 patients completed the study period (fixed-dose, 151; flexible-dose, 158; placebo, 166). Patients in all groups had comparable demographic and baseline MDD characteristics. The mean (SD) age in the three treatment groups ranged from 38.3 (10.2) to 38.6 (11.1) years, and the mean (SD) duration of MDD ranged from 40.3 (50.0) to 52.6 (62.9) months. The mean (SD) baseline HAM-D17 total score and MADRS total score ranged from 22.4 (4.1) to 22.6 (4.1) and from 32.6 (4.4) to 33.2 (5.1), respectively. The distribution of the last dose during the 8-week treatment period was 4.5%, 4.5%, 10.6%, and 80.4% for 37.5 mg/day, 75 mg/day, 150 mg/day, and 225 mg/day, respectively, in the flexible-dose group.
Efficacy
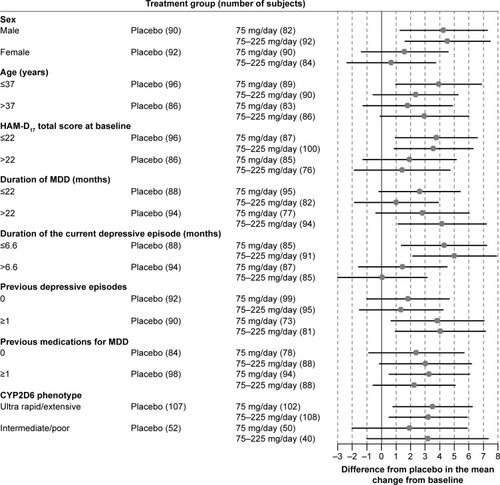
– show forest plots of the differences between each treatment group and the placebo group in the adjusted mean change from baseline at Week 8 (LOCF) in the HAM-D17 total score (), HAM-D6 score (), and MADRS total score (). Both venlafaxine ER groups showed greater treatment benefits compared with the placebo group for all efficacy measures in males than in females; in patients with a low HAM-D17 total score at baseline (≤22) than in those with a high HAM-D17 total score at baseline (>22); in patients with a long duration of MDD (>22 months) than a short duration (≤22 months); in patients with a short duration of current episode (≤6.6 months) than a long duration (>6.6 months); and in patients with one or more previous episodes than none (–). There were no consistent trends in the subgroup of patients with or without a history of previous medications for MDD, in the subgroup of patients in two age categories, and in the subgroup of patients with the two CYP2D6 phenotypes.
Figure 1 Forest plot of the HAM-D17 total score by subgroups: difference between venlafaxine ER treatment group and the placebo group in the adjusted mean change from baseline at Week 8 with 95% CIs (FAS, LOCF, ANCOVA model).
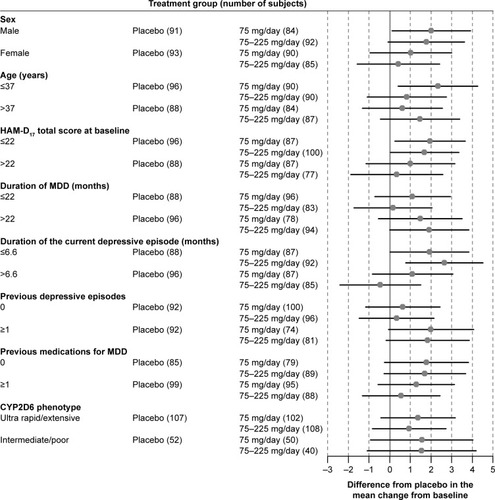
Figure 2 Forest plot of the HAM-D6 score by subgroups: difference between venlafaxine ER treatment group and the placebo group in the adjusted mean change from baseline at Week 8 with 95% CIs (FAS, LOCF, ANCOVA model).
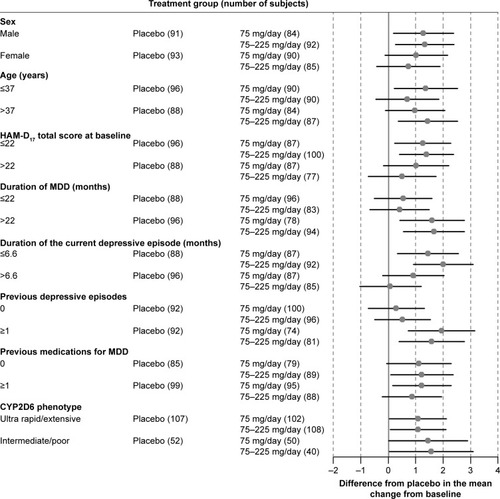
Figure 3 Forest plot of the MADRS total score by subgroups: difference between venlafaxine ER treatment group and the placebo group in the adjusted mean change from baseline at Week 8 with 95% CIs (FAS, LOCF, ANCOVA model).
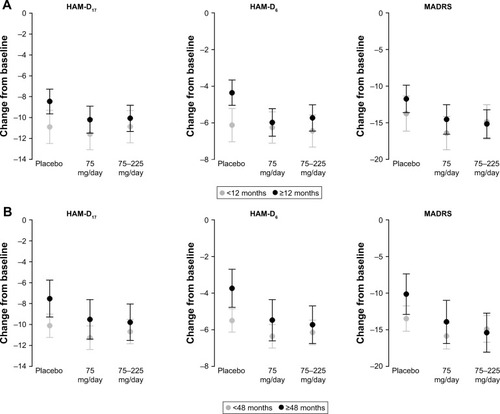
Although the flexible-dose group showed a favorable treatment effect compared with placebo in most subgroups, the flexible-dose group showed a relatively smaller treatment effect than the fixed-dose group in most subgroups. However, a greater treatment effect was seen in the flexible-dose group versus the fixed-dose group for all efficacy measures in subgroups of older patients (>37 years), and in patients with a long duration of MDD (>22 months), and a short duration of current depressive episode (≤6.6 months) (–). Similar trends were observed in duration of MDD in an analysis that divided the groups into durations of 12 months and 48 months ( and , respectively).
Figure 4 Adjusted mean change from baseline at Week 8 with 95% CIs by duration of MDD (≤22 months/>22 months) in each efficacy endpoint (FAS, LOCF, ANCOVA model).
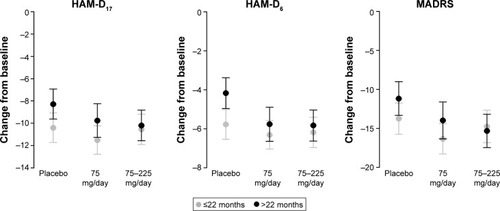
Figure 5 Adjusted mean change from baseline in each efficacy endpoint at Week 8 with 95% CIs by duration of MDD (A) <12 months/≥12 months, and (B) <48 months/≥48 months (FAS, LOCF, ANCOVA model).
Demographic and disease characteristics stratified by duration of MDD (≤22 months/>22 months) are presented in . Overall, demographic characteristics and baseline HAM-D17 and MADRS total scores were comparable between the subgroups in each treatment group. Patients with a long duration of MDD (>22 months) had more frequent previous depressive episodes and a longer duration of the current depressive episode than patients with a short duration of MDD (≤22 months).
Table 1 Demographic and disease characteristics by duration of MDD (≤22 months/>22 months) (FAS)
Discussion
Although these were exploratory, post hoc subgroup analyses of a placebo-controlled clinical study, our results highlight several potential factors that may impact the efficacy of venlafaxine ER in Japanese populations.
As in comparison between subgroups regardless of the treatment groups, there was no meaningful difference in the effect of venlafaxine ER compared with placebo for different degrees of severity of depression at baseline. As shown in , patients with more severe depression (HAM-D17 total score at baseline >22) showed a greater decrease in the mean change from baseline in the HAM-D17 total score among all groups, including the placebo group. While some studies have shown no relationship between severity of depression and treatment response to antidepressants in MDD,Citation12,Citation13 others have shown greater antidepressant–placebo differences in patients with more severe depression.Citation14–Citation17 This discrepancy is thought to be due to the extent of baseline score inflation.Citation18,Citation19 In our study, patients were first screened with MADRS, QIDS16-SR-J, and CGI-S to mitigate baseline score inflation, and a different score (HAM-D17) was used as the primary efficacy measure, although previous studies have used the same score both as an inclusion criterion and the primary efficacy measure. Patients with low baseline HAM-D17 scores (≤22) showed greater treatment benefits than patients with high scores (>22) in both treatment groups compared with the placebo group, because placebo response was much higher in patients with a high baseline HAM-D17 score (>22), particularly in changes from baseline in HAM-D17 and MADRS total scores, which contributed to smaller differences between each treatment group and the placebo group in those patients.
Figure 6 Adjusted mean change from baseline at Week 8 with 95% CIs by HAM-D17 total score at baseline (total score ≤22/total score >22) in each efficacy endpoint (FAS, LOCF, ANCOVA model).
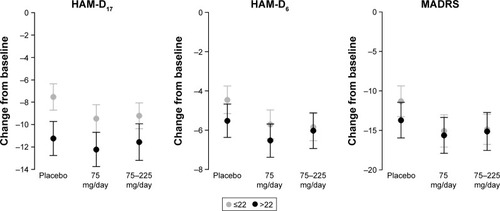
Patients with a long duration of MDD (>22 months) showed greater treatment benefits than those with a short duration of MDD (≤22 months) in both venlafaxine ER treatment groups compared with the placebo group. Placebo response was much smaller in patients with a long duration of MDD (); these results were consistent with a meta-analysis of ten clinical trialsCitation13 as well as other prior studies.Citation20,Citation21 A small placebo response in patients with a long duration of MDD may have contributed to the larger differences observed between each treatment group and the placebo group. Similar trends were seen in an analysis that divided the groups at 12 months and 48 months ( and , respectively).
Comparing the effect between the treatment groups in each subgroup, greater treatment effect was seen in the flexible-dose group versus the fixed dose group in the subgroup with a long duration of MDD. These results may prove the hypothesis that a greater treatment response to venlafaxine ER (up to 225 mg/day) can be seen in patients with a longer duration of MDD. A similar observation was seen in patients in age subgroups. In the older patient (>37 years) subgroup, the effect in the flexible-dose group was greater than that in the fixed-dose group. This result may be considered to be associated with the fact that the mean duration of MDD in the >37 years subgroup was longer than that in the ≤37 years subgroup (data not shown).
Furthermore, in both venlafaxine ER treatment groups, patients with recurrent depressive episodes showed greater treatment benefits than those with a single depressive episode compared with the placebo group. The placebo response was much smaller in patients with recurrent episodes (), which corresponds with the results of a meta-analysis of seven clinical trials.Citation22 A small placebo response may have contributed to the larger differences between the venlafaxine ER groups and the placebo group in patients with recurrent depressive episodes. These results were similar to those for duration of MDD reported previously (), as patients with a long duration of MDD (>22 months) experienced more depressive episodes ().
Figure 7 Adjusted mean change from baseline at Week 8 with 95% CIs by history of previous depressive episodes (0 [single episode]/≥1 [recurrent episodes]) in each efficacy endpoint (FAS, LOCF, ANCOVA model).
![Figure 7 Adjusted mean change from baseline at Week 8 with 95% CIs by history of previous depressive episodes (0 [single episode]/≥1 [recurrent episodes]) in each efficacy endpoint (FAS, LOCF, ANCOVA model).](/cms/asset/2468e920-b6cd-4a7b-9685-d9acef9cab7c/dndt_a_146428_f0007_b.jpg)
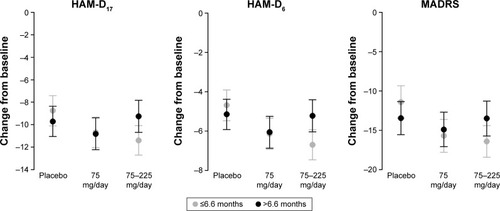
Interestingly, patients with a long duration of the current depressive episode (>6.6 months) versus a short duration (≤6.6 months) showed smaller treatment benefits in both venlafaxine ER treatment groups compared with the placebo group. Treatment benefit of venlafaxine 75–225 mg/day was nearly absent in patients with a long duration of the current depressive episode (). Since the inclusion criteria for the original study required a current depressive episode (≥90 days, single episode; ≥28 days, recurrent episode) before the screening visit, patients with more severe or treatment-resistant depression with a single episode may have been included in the subgroup. However, patients with a short duration of the current depressive episode consistently showed greater treatment benefits in the flexible-dose group than the fixed-dose group compared with the placebo group, which was also consistent with the findings observed in patients with a long duration of MDD (>22 months) ().
Figure 8 Adjusted mean change from baseline at Week 8 with 95% CIs by duration of current depressive episode (≤6.6 months/>6.6 months) in each efficacy endpoint (FAS, LOCF, ANCOVA model).
Finally, in recent years, the response to placebo observed in studies of antidepressants for MDD has increased.Citation23 Placebo response also increases as the number of active medication arms,Citation24 investigational sites,Citation25 and study visitsCitation26 increase, and as the number of academic sitesCitation27 decreases. The number of study visits influences dropout rate rather than treatment response;Citation28 that is, an increasing number of study visits increases the dropout rate. Additionally, site ratings, not centralized ratings, increase placebo response.Citation29 The present study had two active medication arms, seven visits during the 8-week treatment phase, and was conducted with the site rating method at 62 investigational sites. These factors might have contributed considerably to the high placebo response in this study. In addition, it is important to remember that drug adherence is often low among MDD outpatients. In this study, drug adherence was determined through capsule-counting procedures and patient–physician interviews at follow-up visits.
In conclusion, despite a high placebo response, venlafaxine ER improved symptoms of MDD compared with placebo among most subgroups. It is hypothesized that patients with a longer duration of MDD may have a greater treatment response at a higher dose of venlafaxine ER (up to 225 mg/day). Further investigation in real-world settings in Japan is needed to evaluate patient groups that require higher doses of venlafaxine ER.
Data sharing statement
Anonymized patient-level data will be available through the Pfizer Inc. data access request site: http://www.pfizer.com/research/clinical_trials/trial_data_and_results/data_request.
Acknowledgments
This study was sponsored by Pfizer Inc. Editorial support was provided by Pearl Gomes of Cactus Communications and was funded by Pfizer Inc. We are grateful for the contributions of trial participants, principal investigators, and all other medical personnel to this study. Full control of the manuscript content was retained by all authors.
Supplementary material
Disclosure
YA, YH, RI, and TI are employees of Pfizer Japan Inc. KK was an employee of Pfizer Japan Inc. at the time of the study. YW has received speaker’s honoraria from Pfizer Japan Inc., GlaxoSmithKline K.K., Otsuka Pharmaceutical Co., Ltd., Janssen Pharmaceutical K.K., Meiji Seika Pharma Co., Ltd, Eli Lilly Japan K.K., MSD K.K. a subsidiary of Merck & Co., Inc., Takeda Pharmaceutical Co., Ltd., and Mochida Pharmaceutical Co., Ltd., Mitsubishi Tanabe Pharma Corp., and Sumitomo Dainippon Pharma Co., Ltd., within the past 5 years. The authors report no other conflicts of interest in this work.
References
- American Psychiatric AssociationPractice guideline for the treatment of patients with major depressive disorder 3 rd editionAmerican Psychiatric Association2010 Available from: http://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/mdd.pdfAccessed March 12, 2018
- NuttDJDavidsonJRGelenbergAJInternational consensus statement on major depressive disorderJ Clin Psychiatry201071Suppl E1e08
- Japanese Society of Mood DisordersGuideline for treatment of major depressive disorder by the Japanese Society of Mood DisordersJapanese Society of Mood Disorders2013 Available from: http://www.secretariat.ne.jp/jsmd/mood_disorder/img/130924.pdfAccessed March 12, 2018 Japanese
- PapakostasGISerotonin norepinephrine reuptake inhibitors: spectrum of efficacy in major depressive disorderPrim Psychiatry2009165 Suppl 41624
- HiguchiTKamijimaKNakagomeKA randomized, double-blinded, placebo-controlled study to evaluate the efficacy and safety of venlafaxine extended release and a long-term extension study for patients with major depressive disorder in JapanInt Clin Psychopharmacol201631181926513202
- HamiltonMA rating scale for depressionJ Neurol Neurosurg Psychiatry196023566214399272
- MontgomerySAAsbergMA new depression scale designed to be sensitive to changeBr J Psychiatry1979134382389444788
- BechPGramLFDeinEQuantitative rating of depressive statesActa Psychiatr Scand19755131611701136841
- BechPAllerupPGramLFThe Hamilton depression scale. Evaluation of objectivity using logistic modelsActa Psychiatr Scand19816332902997015793
- ClearyPGuyWFactor analysis of the Hamilton depression scaleDrugs under Experimental and Clinical Research19771115120
- RushAJTrivediMHIbrahimHMThe 16-item quick inventory of depressive symptomatology (QIDS), clinician rating (QIDS-C), and self-report (QIDS-SR): a psychometric evaluation in patients with chronic major depressionBiol Psychiatry200354557358312946886
- SheltonRCPrakashAMallinckrodtCHPatterns of depressive symptom response in duloxetine-treated outpatients with mild, moderate or more severe depressionInt J Clin Pract20076181337134817627710
- NelsonJCDelucchiKLSchneiderLSModerators of outcome in late-life depression: a patient-level meta-analysisAm J Psychiatry2013170665165923598969
- ElkinISheaMTWatkinsJTNational Institute of Mental Health Treatment of Depression Collaborative Research Program. General effectiveness of treatmentsArch Gen Psychiatry198946119719822684085
- KhanALeventhalRMKhanSRBrownWASeverity of depression and response to antidepressants and placebo: an analysis of the Food and Drug Administration databaseJ Clin Psychopharmacol2002221404511799341
- KhanABrodheadAEKoltsRLBrownWASeverity of depressive symptoms and response to antidepressants and placebo in antidepressant trialsJ Psychiatr Res200539214515015589562
- FournierJCDeRubeisRJHollonSDAntidepressant drug effects and depression severity: a patient-level meta-analysisJAMA20103031475320051569
- RutherfordBRRooseSPA model of placebo response in antidepressant clinical trialsAm J Psychiatry2013170772373323318413
- ManciniMWadeAGPerugiGLenox-SmithASchachtAImpact of patient selection and study characteristics on signal detection in placebo-controlled trials with antidepressantsJ Psychiatr Res201451212924462042
- PosternakMAZimmermanMKeitnerGIMillerIWA reevaluation of the exclusion criteria used in antidepressant efficacy trialsAm J Psychiatry2002592191200
- CohenDConsoliABodeauNPredictors of placebo response in randomized controlled trials of psychotropic drugs for children and adolescents with internalizing disordersJ Child Adolesc Psychopharmacol2010201394720166795
- BialikRJRavindranAVBakishDLapierreYDA comparison of placebo responders and nonresponders in subgroups of depressive disorderJ Psychiatry Neurosci19952042652707647079
- WalshBTSeidmanSNSyskoRGouldMPlacebo response in studies of major depression: variable, substantial, and growingJAMA2002287141840184711939870
- SinyorMLevittAJCheungAHDoes inclusion of a placebo arm influence response to active antidepressant treatment in randomized controlled trials? Results from pooled and meta-analysesJ Clin Psychiatry201071327027920122371
- BridgeJABirmaherBIyengarSBarbeRPBrentDAPlacebo response in randomized controlled trials of antidepressants for pediatric major depressive disorderAm J Psychiatry20091661424919047322
- PosternakMAZimmermanMTherapeutic effect of follow-up assessments on antidepressant and placebo response rates in antidepressant efficacy trials: meta-analysisBr J Psychiatry200719028729217401033
- DunlopBWThaseMEWunCCA meta-analysis of factors impacting detection of antidepressant efficacy in clinical trials: the importance of academic sitesNeuropsychopharmacology201237132830283622910458
- RutherfordBRCooperTMPersaudALess is more in antidepressant clinical trials: a meta-analysis of the effect of visit frequency on treatment response and dropoutJ Clin Psychiatry201374770371523945448
- KobakKALeuchterADeBrotaDSite versus centralized raters in a clinical depression trial: impact on patient selection and placebo responseJ Clin Psychopharmacol201030219319720520295