Abstract
Background
Risperidone long-acting injection (RLAI) has been shown to be efficacious, improve compliance, and increase long-term retention rate on therapy. The aim of this work was to determine the effect of RLAI on clinical outcome and hospitalization rate in patients with schizophrenia or schizoaffective disorder enrolled in the electronic Schizophrenia Treatment Adherence Registry in Latin America.
Methods
Data were collected at baseline, retrospectively for the 12 months prior to baseline, and prospectively every three months for 24 months. Hospitalization prior to therapy was assessed by a retrospective chart review. Efficacy and functioning were evaluated using Clinical Global Impression of Illness Severity (CGI-S), Personal and Social Performance (PSP), and Global Assessment of Functioning (GAF) scores. Relapse and treatment were also registered.
Results
Patients were recruited in Mexico (n = 53), Brazil (n = 11), and Colombia (n = 15). Sixty-five percent (n = 52) were male, and mean age was 32.9 years. Patients were classified as having schizophrenia (n = 73) or schizoaffective disorder (n = 6). The mean dose of RLAI at six months was 34.1 mg (standard deviation = 10.2 mg). The percentage of hospitalized patients before treatment was 28.2% and 5.1% at six months after initiating RLAI (P < 0.001). Significant changes were registered on CGI-S, GAF, and PSP scores.
Conclusions
RLAI was associated with an improvement in clinical symptoms and functioning, and a greater reduction in hospitalization.
Introduction
Pharmacological treatment with antipsychotics is the essential component of schizophrenia therapy. The development of atypical antipsychotics has proven to be an important advance in the control of this disease. These medications show high levels of efficacy in controlling positive and negative symptoms,Citation1,Citation2 a modest effect on cognitive function,Citation3,Citation4 and a positive effect on affective symptoms.Citation5,Citation6 In addition, the atypical antipsychotics have been associated with an improvement in quality of life and performance in social contexts.Citation7,Citation8 Furthermore, it is well established that the prescription of atypical antipsychotics is associated with a decrease in the incidence of extrapyramidal symptoms.Citation9
Despite the obvious benefits, it is well known that an significant proportion of schizophrenic patients do not take their medication.Citation10 Estimates suggest that one-third of schizophrenic patients follow their treatment, another one-third present partial adherence to treatment, and the final one-third fail to follow treatment regimens.Citation11,Citation12 More than 35% of patients who start treatment have problems following their treatment protocol during the first six weeks, and the nonadherence rate has been reported to increase up to 75% after two-year follow-up.Citation13,Citation14 A low adherence rate was found after 12 months of treatment for oral therapies, including those with atypical antipsychotics.Citation15
The problem of low adherence is shown in studies of the first psychotic episode, where symptom remission has been observed in 80% of patients treated with antipsychotics.Citation16,Citation17 However, 80% of patients diagnosed with their first schizophrenic or schizoaffective episode present approximately two relapses in the first five years of the disease,Citation18 with symptom remission being less likely after each relapse.Citation19 In addition, a larger number of relapses have been shown to be correlated with poor functioning and a reduction in response to treatment.Citation20,Citation21 In addition, these patients and their caregivers experience extremely high levels of stress associated with relapse and hospitalization. Multiple studies have shown that low adherence rates in the treatment of schizophrenia are associated with a poor prognosis and more substantial decline in physical health.Citation22,Citation23
Apart from its impact on prognosis, lack of adherence has an important effect on the economic impact of the disease and utilization of health resources. Patients with poor adherence have a higher rate of hospitalization and longer hospital stays.Citation24,Citation25 It has been calculated that improving treatment adherence in patients with schizophrenia could save US$100 million dollars in the cost of medical attention by reducing both the number and duration of hospitalizations.Citation26 Therefore, treatment adherence is the one important variable that can be controlled to diminish the cost of schizophrenia by reducing relapse rates.
The long-acting injectable antipsychotics have a prolonged duration of action and may be a solution to decrease the relapse rate because they have been shown to increase treatment adherence by 10%–40%.Citation27 Many randomized trials have been conducted comparing the relapse rates of oral versus long-acting injectable antipsychotics. The findings of these studies favored the latter form of antipsychotics.Citation28,Citation29 Despite these findings, and the recommendations for using long-acting injectable antipsychotics for patients showing poor adherence to oral antipsychotics (recommended in the guidelines of the American Psychiatric Association for the handling of schizophrenia, UK National Institute for Health and Clinical Excellence, Schizophrenia Patient Outcomes Research Teams, and the Texas Medication Algorithm Project), physicians are reluctant to change their prescribing habits. In general, most of the barriers to the prescription of long-acting injectable antipsychotics are related to the lack of knowledge among doctors on how to use these forms of drugs and the idea that they should only be used in a very specific group of people, ie, severely ill patients and those who have been shown to have poor adherence.
Currently, there is a form of risperidone long-acting injectable (RLAI) that has been shown to increase adherence to antipsychotic treatments and improve clinical and economic parameters in patients with schizophrenia.Citation30–Citation32 This is the first atypical antipsychotic with a prolonged action, and has been shown to induce fewer extrapyramidal symptoms when compared with long-acting injectable first-generation antipsychotics, and to improve adherence and reduce relapse rates.Citation33,Citation34
However, as is the case in some other geographic regions, prescribing of long-acting risperidone in Latin America is uncommon and predominantly used in severe cases and in patients with poor adherence to treatment. For this reason, the Electronic Schizophrenia Treatment Adherence (e-Star)Citation35 has been implemented in Latin America as well as in other regions. The objective of this project is to determine the outcomes and hospitalization rates before and after treatment with RLAI in a group of patients with schizophrenia or schizoaffective disorder in a naturalistic setting. We hypothesized that the switch to RLAI will improve the symptoms and functioning, thereby reducing hospitalization rates. In this report, we present a preliminary prespecified interim analysis of the results from this project after six months of follow-up.
Methods and materials
This study was conducted in accordance with the regulations on Good Clinical Practice and the Helsinki Declaration of the World Medical Association, Edinburgh, 2000. The experimental protocol was approved by the different ethics committees of each of the participating institutions. Written informed consent was obtained from all patients after the procedures were carefully explained to them.
Subjects
Subjects were recruited from hospitalization services, emergency rooms, and outpatient programs in private and public institutions from Mexico, Colombia, and Brazil. Eligible patients included males, females who were not pregnant or lactating, those aged over 18 years, with a diagnosis of schizophrenia or schizoaffective disorder according to Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV) criteria. In addition, all subjects experienced either acute or chronic episodes that could benefit from treatment with RLAI, according to the clinical criteria of the researcher. Finally, all subjects had to submit written consent. Patients with bipolar disorder, a previous history of intolerance or poor response to risperidone that was not associated with poor adherence, women who were pregnant or planning to get pregnant during the two years of follow-up, or women who did not have a reliable contraception method available to them were excluded from this study.
Design and procedures
The Electronic Schizophrenia Treatment Adherence Registry is an independent international registry that records the usage of RLAI. The registry had a one-year retrospective analysis in which the usage of medications and the hospitalization history of each patient were recorded. At baseline, the demographic characteristics of the diseases and the reasons for the change in antipsychotic drugs were registered. The severity of the disease was assessed using the Clinical Global Impression-Schizophrenia scale (CGI-SCH).Citation36 Social functioning was registered using the Personal and Social Performance (PSP) scale, and the Global Assessment of Functioning (GAF) scale.Citation37 After baseline registration, a two-year, prospective follow-up was conducted with evaluations every three months using the CGI-SCH severity scale (CGI-SCH SI) as the estimator of efficacy and the PSP and GAF scales to assess functionality. The PSP scale is a tool that indicates how well a patient functions. The scale ranges from 1–100, where 1–10 represents lack of autonomy and 91–100 represents excellent functioning. The classifications are based on the evaluation of four objective indicators, ie, activities that contribute to society (including work and study), social and personal relationships, taking care of oneself, and disturbing and aggressive behaviors.Citation38 In each evaluation, adherence and satisfaction with treatment, other medications being taken, side effects, and hospitalizations were recorded. The initial doses of RLAI were prescribed according to the clinical criteria of the investigator and the condition of the patients. The doses were adjusted during follow-up, according to efficacy and tolerability. Concomitant therapy with anticholinergic agents, antidepressants, mood stabilizers, benzodiazepines, antipsychotics, and other medications were prescribed at the researcher’s discretion according to the patient’s condition.
Statistical analysis
Demographic and clinical characteristics were analyzed with frequencies and percentages for the categorical variables and means and standard deviations (SD) for the continuous variables. McNemar’s test was used to compare the percentage of patients hospitalized during the retrospective evaluation with those hospitalized during the prospective phase. This test was also utilized to determine the usage of concomitant therapy in each of these stages. Paired t-tests were used for the efficacy analyses of CGI and the functionality with GAF and PSP.
The sample size for a two-year follow-up was based on the minimum numbers required to demonstrate a reduction in the mean number of days of hospitalization. It is expected that patients in this study will have an average baseline of 21.6 days, and would show an average of 8.8 (SD = 37.1) days at the end of the study. These numbers reflect the results observed in previous studies with RLAI. The inclusion of 189 patients will permit us to demonstrate statistical differences with a 90% power.
Results
Patients
Seventy-nine patients were recruited in Mexico (n = 53), Colombia (n = 15), and Brazil (n = 11). These patients successfully completed the six-month follow-up. There was a predominance of men (n = 52, 65.8%), with the mean sample age being 32.9 years (SD = 8.8). Most of the sample was unemployed (n = 59, 74.7%) at the onset of the study, and only four patients had a full-time job (5.1%). Seventy-three patients were classified as schizophrenic (92.4%), and six were classified as having schizoaffective disorder (7.6%). The mean length of illness was 8.5 years (SD = 7.0). At baseline evaluation, 10 patients were hospitalized. Only one patient stopped treatment with RLAI because he was lost during follow-up (1.3%).
The most important clinical reasons to start treatment with RLAI were a low adherence rate (n = 29, 36.7%) and a lack of efficacy (n = 28, 35.4%). A recommendation of a maintenance treatment was the third reason to start RLAI treatment (n = 12, 15.2%). In addition, five patients decided to start RLAI therapy due to its convenience (6.3%).
Hospitalization
There was a significant reduction in the need for hospitalization services after patients switched to treatment with RLAI. The proportion of hospitalized patients significantly decreased from 28.2% to 5.1% (P < 0.001), and the duration of hospitalization also significantly decreased from 13 days to 2.1 days (P = 0.002) when comparing the six-month retrospective evaluation versus the six-month prospective evaluation of these variables ().
Table 1 Patients fully hospitalized at least once per period and length of stay by period (n = 78)
Clinical outcomes
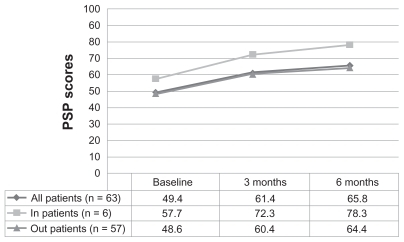
Compared with the initial phase, the mean CGI-SCH SI global score significantly improved after six months of treatment (4.19, SD = 1.01 versus 3.02, SD = 1.3, respectively, P < 0.001). At the endpoint, the severity of positive, negative, depressive, and cognitive symptoms were scored in a 1–3 range (mild symptoms). In addition, global functioning significantly improved after six months of RLAI treatment (55.7, SD = 16.9 versus 69.9, SD = 16.1, P < 0.001). Social functioning, which was evaluated using the PSP scale, also showed a significant improvement when compared with the baseline conditions for all the follow-up periods. Furthermore, a comparison of PSP scores in outpatients and hospitalized patients showed that the latter failed to present a significant change ().
Figure 1 Evolution of PSP scores over time.
Abbreviation: n-s, not significant.
Patients reported being satisfied (n = 22, 33.8%) or very satisfied (n = 39, 60%) with the RLAI treatment, and only one patient was unsatisfied with the treatment (1.5%). Sixty-five patients (82.2%) received a prescription of 25 mg of RLAI at treatment onset whereas two patients were prescribed an initial dose of 50 mg. The mean RLAI doses at onset, and at three and six months, were 27.5 mg (SD = 5.8), 31.8 mg (SD = 8.7), and 34.1 mg (SD = 10.2), respectively. At the last time point, 12 patients were on a 50 mg dose and one patient was receiving 75 mg. The proportion of patients receiving either 25 mg or 37.5 mg was similar (n = 25 [46.2%] and n = 29 [37%], respectively). Adherence to treatment at the six-month follow-up was excellent (81%–100%) in 65 patients (82.2%). The remaining patients were not included in the final evaluation.
Some patients received haloperidol 1–5 mg/day and risperidone 2–4 mg/day in addition to RLAI. The prescription patterns of antipsychotics prior to treatment and during treatment are shown in .
Table 2 Antipsychotics taken, by class, with each class counted only once (n = 79)
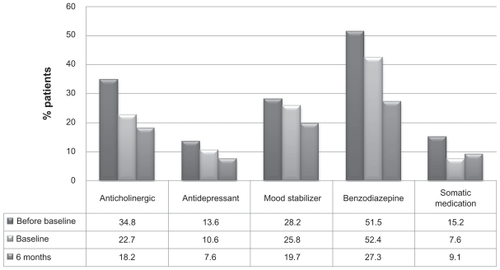
Concomitant therapy mainly included antidepressants (fluoxetine, sertraline 20–40 mg/day), mood stabilizers (valproate 200–400 mg/day, carbamazepine 200–400 mg/day, lamotrigine 25–100 mg/day), and benzodiazepines (clonazepam, lorazepam 2–4 mg/day). Patients were less likely to receive concomitant therapy during the study. As a result, there was a significant reduction in the prescription of benzodiazepines (n = 28, 42% at baseline versus n = 18, 27.3% at the six-month follow-up, P = 0.04). Although changes in the prescription of drugs other than benzodiazepines were not statistically significant, they were also reduced during the RLAI study ().
Figure 2 Concomitant therapy.
Treatment with RLAI was well tolerated during the study. Only 16 patients (20.2%) presented side effects, which were not serious. The most common side effect was akinesia (n = 4, 5%). In addition, three patients showed gastrointestinal disturbances (3.8%) and two patients showed changes in metabolism (2.5%). Additionally, two patients (2.5%) showed exacerbation of psychosis symptoms and required hospitalization.
Discussion
The preliminary results of this multicenter, naturalistic, retrospective, and prospective study in Latin America confirmed that RLAI improves symptoms and functionality in schizophrenic patients, while decreasing the number and length of hospitalizations. In addition, it shows excellent treatment adherence in patients with schizophrenia.
By improving treatment adherence with RLAI, relapses and hospitalizations were significantly reduced. Sixty-seven patients, representing 84% of our sample, showed no relapse or rehospitalization during the first six months of treatment.
This study’s favorable findings with respect to the efficacy of RLAI confirmed the results from previous short- and long-term studies that examined the efficacy of RLAI in patients with schizophrenia.Citation39–Citation41 The findings of this study suggested that there was an improvement in the patients’ outcomes when they were switched to the long-term treatment. This was similar to previous studies where treatments with other oral or long-acting injectable antipsychotics,Citation42–Citation45 including patients treated previously with oral risperidone,Citation46 were switched to RLAI. It is highly likely that this improvement was due to the improvement of partial adherence, as shown by the excellent rates of complete adherence found in the patients at the end of the study. One of the biggest advantages of long-acting injectable antipsychotics is that they allow for strict monitoring. Thus, when the patient does not inject the medicine, immediate decisions can be made to prevent this failure in adherence and to involve the family and primary caregivers.Citation47 This is particularly important in Latin American countries, where patients frequently have poor access to mental health services due to lack of available services in all the communities and long distances to mental health facilities.
Risk factors for lack of adherence can be conceptualized as being related to the patient, the treatment, or the environment. Citation48 Treatment-related factors are usually lack of efficacy and the occurrence of side effects that lead to the patient deciding to suspend their medication. Although the presence of side effects is not usually considered a factor directly associated with adherence,Citation49 it does influence the patient’s perception of the benefits of taking the medication.Citation50 This important factor is explained in the model of health beliefs, which proposes that patients will value and compare the perceived benefits and costs of the medication. If they believe that the benefits outweigh the costs, they will generally show a higher adherence to treatment.Citation51 Relatively few patients have withdrawn from RLAI studies due to side effects (1.2%–16%), and the drug is generally well tolerated.Citation52 The results of this study confirm that RLAI is a safe and well tolerated treatment option. In addition, these findings do not support the perception by some doctors and patients that long-acting injectable antipsychotics have more side effects than the oral formulations. Indeed, it is this inaccurate perception that has limited the prescribing of this presentation of antipsychotics.Citation53
The treatment benefits that have been perceived by patients include an improvement in general well being, mental health, and functionality.Citation54 These benefits for the patient are usually not analyzed in controlled clinical studies because these studies are designed to focus on establishing efficacy and tolerance. Studies focused on the real world, such as this one, allow for the assessment of these variables. In our study, we were able to show an improvement in patient functionality from the onset of the treatment with RLAI. This finding was consistent with results found from post hoc analyses of controlled studiesCitation55,Citation56 and studies done in real-world settings,Citation35 which have shown an improvement in functionality with RLAI.
The cost of schizophrenia increases four-fold in patients who present one relapse,Citation57 and 79% of the direct cost of schizophrenia is related to hospitalization or institutional care. Interestingly, the medications represent only a small fraction (1%–6%) of the overall cost of the disease.Citation58 In this study, the preliminary results showed an important reduction in the rate of hospitalizations and concomitant therapy, which resulted in a lower utilization of resources, which could lead to a reduction in the cost of schizophrenia. However, a pharmacoeconomic study is necessary to determine the possible relationship between these variables and a decrease in the cost of schizophrenia in Latin America.
It is important to highlight that the patients were prescribed RLAI according to the clinical discretion of the researcher. The two main reasons for switching treatments were poor adherence and lack of efficacy. Only a small number of patients decided to switch to RLAI due to convenience. This finding supports the existence of a strong misconception in Latin America that long-acting injectable antipsychotics should only be used in patients with severe symptoms and poor adherence. A recent study examining the criteria used for the prescription of long-acting injectable antipsychotics found that patients taking depot antipsychotics had higher rates of adherence problems and more extrapyramidal symptoms. It is notable that patients who received RLAI tended to have more severe disease than those treated with long-acting injectable first-generation antipsychotics.Citation59 The fact that RLAI tends to be prescribed for severe patients is likely associated with the perception of a higher efficacy, but it supports the hypothesis that there are specific criteria being used for its prescription. Studies have shown that RLAI was effective and well tolerated in patients in their first psychotic episode, reduced hospitalization rates, and improved prognosis by reducing relapse.Citation60–Citation62 However, the preconceived notions about its use still remain. Other factors that have limited the use of long-acting injectable antipsychotics are lack of reimbursement in some settings, and the lack of knowledge by doctors, as well as their belief that the patient or their family would refuse this form of treatment.Citation63 However, surveys of outpatients treated with long-acting injectable typical antipsychotics have shown that 87% chose to continue with this form of the drug.Citation64 The high satisfaction rates observed for RLAI in this study suggest that the first barrier to its prescription is simply a lack of knowledge.
The main limitations of our study were the lack of a control group and that it was not blinded, which allowed for possible observational bias. Despite these limitations, it is important to establish the relevance of the use of prospective data and that it is necessary to use studies focused on the real world to evaluate adherence because controlled studies, by design, will exclude patients that do not adhere to treatment. In addition, the use of the same patient as a control itself allowed us to avoid another selection bias.
In summary, our preliminary results highlight the efficacy and tolerability of RLAI in schizophrenic patients. This treatment reduces the burden on health resources and prevents relapses by increasing adherence to treatment. Further studies of RLAI in recently diagnosed patients are necessary. Given that doctors tend to prescribe long-acting injectable antipsychotics only to severe patients and those who have shown adherence problems, it is imperative that doctors gain a better understanding of long-acting injectable antipsychotics.
Acknowledgment
RA is supported by the National System of Investigators, CONACYT.
Disclosure
This study was supported by an unrestricted educational grant from the Janssen Cilag Medical Affairs Department in Mexico. RA has participated on speaker/advisory boards and received honoraria from Janssen and AstraZeneca, and has received research funding from Janssen, AstraZeneca, and UCLA. RC has participated in speaker/advisory boards and received honoraria from Janssen and AstraZeneca. ML has participated in speaker/advisory boards and received honoraria from Janssen Cilag, AstraZeneca, Eli Lilly, and Novartis.
References
- BeasleyCMJTollefsonGTranPSatterleeWSangerTHamiltonSOlanzapine versus placebo and haloperidol: Acute phase results of the North American double-blind olanzapine trialNeuropsychopharmacology19961421111238822534
- LindenmayerJPGrochowskiSMabugatLClozapine effects on positive and negative symptoms: A six-month trial in treatment-refractory schizophrenicsJ Clin Psychopharmacol19941432012048027417
- BarkicJFilakovicPRadanovic-GrguricLThe influence of risperidone on cognitive functions in schizophreniaColl Antropol200327Suppl 111111812955900
- KeefeRSBilderRMDavisSMNeurocognitive effects of antipsychotic medications in patients with chronic schizophrenia in the CATIE TrialArch Gen Psychiatry200764663364717548746
- BuckleyPFGoldsteinJMEmsleyRAEfficacy and tolerability of quetiapine in poorly responsive, chronic schizophreniaSchizophr Res20046623143150
- PeuskensJMollerHJPuechAAmisulpride improves depressive symptoms in acute exacerbations of schizophrenia: Comparison with haloperidol and risperidoneEur Neuropsychopharmacol200212430531012126869
- ColonnaLSaleemPDondey-NouvelLReinWLong-term safety and efficacy of amisulpride in subchronic or chronic schizophrenia. Amisulpride Study GroupInt Clin Psychopharmacol2000151132210836281
- SwartzMSPerkinsDOStroupTSEffects of antipsychotic medications on psychosocial functioning in patients with chronic schizophrenia: Findings from the NIMH CATIE studyAm J Psychiatry2007164342843617329467
- LeuchtSCorvesCArbterDEngelRRLiCDavisJMSecond-generation versus first-generation antipsychotic drugs for schizophrenia: A meta-analysisLancet20093739657314119058842
- MasandPSNarasimhanMImproving adherence to antipsychotic pharmacotherapyCurr Clin Pharmacol200611475618666377
- BlackwellBTreatment adherenceBr J Psychiatry1976129513531793670
- WrightECNon-compliance – or how many aunts has Matilda?Lancet199334288769099138105172
- WeidenPRapkinBZygmuntAMottTGoldmanDFrancesAPostdischarge medication compliance of inpatients converted from an oral to a depot neuroleptic regimenPsychiatr Serv19954610104910548829787
- WeidenPJDiscontinuing and switching antipsychotic medications: Understanding the CATIE schizophrenia trialJ Clin Psychiatry200768Suppl 1121917286523
- DolderCRLacroJPDunnLBJesteDVAntipsychotic medication adherence: Is there a difference between typical and atypical agents?Am J Psychiatry2002159110310811772697
- LiebermanJAAlvirJMWoernerMProspective study of psychobiology in first-episode schizophrenia at Hillside HospitalSchizophr Bull19921833513711411327
- RobinsonDGWoernerMGAlvirJMPredictors of treatment response from a first episode of schizophrenia or schizoaffective disorderAm J Psychiatry1999156454454910200732
- RobinsonDWoernerMGAlvirJMPredictors of relapse following response from a first episode of schizophrenia or schizoaffective disorderArch Gen Psychiatry199956324124710078501
- WiersmaDNienhuisFJSlooffCJGielRNatural course of schizophrenic disorders: A 15-year followup of a Dutch incidence cohortSchizophr Bull199824175859502547
- LiebermanJAKoreenARChakosMFactors influencing treatment response and outcome of first-episode schizophrenia: Implications for understanding the pathophysiology of schizophreniaJ Clin Psychiatry199657Suppl 9598823344
- ShepherdMWattDFalloonISmeetonNThe natural history of schizophrenia: A five-year follow-up study of outcome and prediction in a representative sample of schizophrenicsPsychol Med Monogr Suppl1989151462798648
- MarderSRFacilitating compliance with antipsychotic medicationJ Clin Psychiatry199859Suppl 321259541334
- MooreASellwoodWStirlingJCompliance and psychological reactance in schizophreniaBr J Clin Psychol200039Pt 328729511033750
- GilmerTPDolderCRLacroJPAdherence to treatment with antipsychotic medication and health care costs among Medicaid beneficiaries with schizophreniaAm J Psychiatry2004161469269915056516
- ValensteinMCopelandLABlowFCPharmacy data identify poorly adherent patients with schizophrenia at increased risk for admissionMed Care200240863063912187177
- MarcusSCOlfsonMOutpatient antipsychotic treatment and inpatient costs of schizophreniaSchizophr Bull200834117318017578893
- RemingtonGJAdamsMEDepot neuroleptic therapy: Clinical considerationsCan J Psychiatry1995403 Suppl 1S5117627927
- DavisJMMatalonLWatanabeMDBlakeLMetalonLDepot antipsychotic drugs. Place in therapyDrugs19944757417737520856
- LehmanAFSteinwachsDMPatterns of usual care for schizophrenia: Initial results from the Schizophrenia Patient Outcomes Research Team (PORT) Client SurveySchizophr Bull199824111209502543
- OlivaresJMRodriguez-MoralesADielsJLong-term outcomes in patients with schizophrenia treated with risperidone long-acting injection or oral antipsychotics in Spain: Results from the electronic Schizophrenia Treatment Adherence Registry (e-STAR)Eur Psychiatry200924528729619195847
- EdwardsNCLocklearJCRupnowMFDiamondRJCost effectiveness of long-acting risperidone injection versus alternative antipsychotic agents in patients with schizophrenia in the USAPharmacoeconomics200523Suppl 1758916416763
- AnnemansLCost effectiveness of long-acting risperidone: What can pharmacoeconomic models teach us?Pharmacoeconomics200523Suppl 11216416757
- TaylorDMFischettiCSparshattAThomasABisharaDCorneliusVRisperidone long-acting injection: A prospective 3-year analysis of its use in clinical practiceJ Clin Psychiatry200970219620019026261
- LindenmayerJPParakMGormanJMImproved long-term outcome with long-acting risperidone treatment of chronic schizophrenia with prior partial responseJ Psychiatr Pract2006121555716432447
- PeuskensJOlivaresJMPecenakJTreatment retention with risperidone long-acting injection: 24-month results from the Electronic Schizophrenia Treatment Adherence Registry (e-STAR) in six countriesCurr Med Res Opin201026350150920014981
- HaroJMKamathSAOchoaSThe Clinical Global Impression-Schizophrenia scale: A simple instrument to measure the diversity of symptoms present in schizophreniaActa Psychiatr Scand Suppl2003416162312755850
- EndicottJSpitzerRLFleissJLCohenJThe global assessment scale. A procedure for measuring overall severity of psychiatric disturbanceArch Gen Psychiatry1976336766771938196
- MorosiniPLMaglianoLBrambillaLUgoliniSPioliRDevelopment, reliability and acceptability of a new version of the DSM-IV Social and Occupational Functioning Assessment Scale (SOFAS) to assess routine social functioningActa Psychiatr Scand2000101432332910782554
- FleischhackerWWEerdekensMKarcherKTreatment of schizophrenia with long-acting injectable risperidone: A 12-month open-label trial of the first long-acting second-generation antipsychoticJ Clin Psychiatry200364101250125714658976
- KaneJMEerdekensMLindenmayerJPKeithSJLesemMKarcherKLong-acting injectable risperidone: Efficacy and safety of the first long-acting atypical antipsychoticAm J Psychiatry200316061125113212777271
- MartinSDLibrettoSEPrattDJBrewinJSHuqZUSalehBTClinical experience with the long-acting injectable formulation of the atypical antipsychotic, risperidoneCurr Med Res Opin200319429830512841922
- LindenmayerJPEerdekensEBerrySAEerdekensMSafety and efficacy of long-acting risperidone in schizophrenia: A 12-week, multicenter, open-label study in stable patients switched from typical and atypical oral antipsychoticsJ Clin Psychiatry20046581084108915323593
- MollerHJLlorcaPMSacchettiEMartinSDMedoriRParelladaEEfficacy and safety of direct transition to risperidone long-acting injectable in patients treated with various antipsychotic therapiesInt Clin Psychopharmacol200520312113015812261
- MarinisTDSaleemPTGluePSwitching to long-acting injectable risperidone is beneficial with regard to clinical outcomes, regardless of previous conventional medication in patients with schizophreniaPharmacopsychiatry200740625726318030649
- TurnerMEerdekensEJackoMEerdekensMLong-acting injectable risperidone: Safety and efficacy in stable patients switched from conventional depot antipsychoticsInt Clin Psychopharmacol200419424124915201572
- SchmaussMSacchettiEKahnJPMedoriREfficacy and safety of risperidone long-acting injectable in stable psychotic patients previously treated with oral risperidoneInt Clin Psychopharmacol2007222859217293708
- MasandPSRocaMTurnerMSKaneJMPartial adherence to antipsychotic medication impacts the course of illness in patients with schizophrenia: A reviewPrim Care Companion J Clin Psychiatry200911414715419750066
- FleischhackerWWOehlMAHummerMFactors influencing compliance in schizophrenia patientsJ Clin Psychiatry200364Suppl 16101314680413
- LacroJPDunnLBDolderCRLeckbandSGJesteDVPrevalence of and risk factors for medication nonadherence in patients with schizophrenia: A comprehensive review of recent literatureJ Clin Psychiatry2002631089290912416599
- RosaMAMarcolinMAElkisHEvaluation of the factors interfering with drug treatment compliance among Brazilian patients with schizophreniaRev Bras Psiquiatr200527317818416224604
- BebbingtonPEThe content and context of complianceInt Clin Psychopharmacol19959Suppl 541507622833
- ChuePLong-acting risperidone injection: Efficacy, safety, and cost-effectiveness of the first long-acting atypical antipsychoticNeuropsychiatr Dis Treat200731133919300536
- PatelMXde ZoysaNBernadtMDavidASA cross-sectional study of patients’ perspectives on adherence to antipsychotic medication: Depot versus oralJ Clin Psychiatry200869101548155619192437
- NasrallahHATargumSDTandonRMcCombsJSRossRDefining and measuring clinical effectiveness in the treatment of schizophreniaPsychiatr Serv200556327328215746501
- FleischhackerWWRabinowitzJKemmlerGEerdekensMMehnertAPerceived functioning, well-being and psychiatric symptoms in patients with stable schizophrenia treated with long-acting risperidone for 1 yearBr J Psychiatry200518713113616055823
- NasrallahHADuchesneIMehnertAJanagapCEerdekensMHealth-related quality of life in patients with schizophrenia during treatment with long-acting, injectable risperidoneJ Clin Psychiatry200465453153615119916
- AlmondSKnappMFrancoisCToumiMBrughaTRelapse in schizophrenia: Costs, clinical outcomes and quality of lifeBr J Psychiatry200418434635115056580
- GoereeRFarahatiFBurkeNThe economic burden of schizophrenia in Canada in 2004Curr Med Res Opin200521122017202816368053
- VehofJPostmaMJBruggemanRPredictors for starting depot administration of risperidone in chronic users of antipsychoticsJ Clin Psychopharmacol200828662563019011430
- EmsleyRMedoriRKoenLOosthuizenPPNiehausDJRabinowitzJLong-acting injectable risperidone in the treatment of subjects with recent-onset psychosis: A preliminary studyJ Clin Psychopharmacol200828221021318344732
- EmsleyROosthuizenPKoenLNiehausDJMedoriRRabinowitzJRemission in patients with first-episode schizophrenia receiving assured antipsychotic medication: A study with risperidone long-acting injectionInt Clin Psychopharmacol200823632533118854720
- ParelladaEAndrezinaRMilanovaVPatients in the early phases of schizophrenia and schizoaffective disorders effectively treated with risperidone long-acting injectableJ Psychopharmacol200519Suppl 551416144781
- LambertTBrennanACastleDKellyDLConleyRRPerception of depot antipsychotics by mental health professionalsJ Psychiatr Pract20039325226015985940
- PereiraSPintoRA survey of the attitudes of chronic psychiatric patients living in the community toward their medicationActa Psychiatr Scand19979564644689242840