
Abstract
Objective
Recent controversial evidence suggests that maternal diabetes may increase the risk of attention deficit and hyperactivity disorder (ADHD) in offspring. To examine this potential association, a systematic literature search and meta-analysis was performed.
Methods
OR or risk ratio (RR) from each study was obtained and combined for evaluating the risk. Six cohort studies and three case-control studies were included in the present study.
Results
The meta-analysis of the highly heterogeneous case-control studies did not find significant association between maternal diabetes and ADHD risk (OR: 1.20, 95% CI: 0.96–1.49). The combining of the cohort studies demonstrated that offspring of diabetic mothers were at higher risk of ADHD (RR: 1.40, 95% CI: 1.27–1.54); however, publication bias was identified. When exposure was specified as gestational diabetes mellitus (GDM), GDM exposure increased the risk of ADHD for children by 164% (95% CI: 1.25–5.56) in a Caucasian population. Neither heterogeneity nor publication bias was detected.
Conclusion
Maternal diabetes, especially GDM, is probably a risk factor for ADHD in the Caucasian population. More studies based on large sample size and different ethnicities are needed to confirm this association.
Introduction
Attention deficit and hyperactivity disorder (ADHD) is an early-onset neurodevelopmental disorder combining overactivity and impulsivity with the inability to concentrate, resulting in functional impairment in academic, family, and social settings. A systematic review including 175 studies has demonstrated that ADHD affects up to 7.2% (95% CI: 6.7–7.8) of children worldwide.Citation1 A recent investigation in the UK has demonstrated a marked increase in ADHD prevalence, incidence, and medication.Citation2 Therefore, this disorder is of particular public health concern. The etiology of ADHD is complex since it is clear that ADHD has a strong genetic component,Citation3 while environmental risk factors are also implicated.Citation4 For psychiatric disorders in children, exposure to risk factors in utero plays an important role.Citation5 For example, a hyperglycemic intrauterine environment may exert a negative impact on the development of fetal brain.Citation6
Diabetes before pregnancy is known as pregestational diabetes mellitus (PGDM). Gestational diabetes mellitus (GDM) is defined as diabetes diagnosed in the second and third trimesters of pregnancy. Experiments in animal models of diabetic pregnancies have demonstrated that maternal hyperglycemia usually creates an inflammatory environment by promoting oxidative stress via production of reactive oxygen species within the embryo and fetus.Citation7 Intriguingly, it has been hypothesized that ADHD may be due to central nervous system inflammatory response in the fetus caused by maternal inflammation and immune response.Citation8 In addition, murine models have showed that maternal diabetes induces imbalance in the epigenetic mechanisms, alters transcriptional factors and signaling pathways, and thereby contributes to neurodevelopmental disorders.Citation9
In line with the experimental evidence mentioned earlier, population studies have suggested a possible association between maternal diabetes and the risk of ADHD for children. Several observational studies in the Caucasian and Chinese populations have revealed that maternal diabetes was related to higher risk of ADHD among children.Citation10–Citation13 However, some retrospective studies based on large sample size have reported statistically insignificant results,Citation8,Citation14 indicating that offspring from diabetic mothers may be vulnerable to ADHD. Because results from population investigations are currently controversial, we systematically searched the electronic databases, identified all the relevant studies, and performed meta-analyses to quantitatively synthesize all the available data. This is, to our knowledge, the first meta-analysis to study the association between maternal diabetes and risk of ADHD in offspring.
Materials and methods
Literature search
This meta-analysis followed the recommended PRISMA guidelines.Citation15 A comprehensive literature search was conducted on PubMed, Web of Science, Embase, PsycINFO, WanFang, and China National Knowledge Infrastructure (CNKI) database. The most recent search was conducted in November 2018. The detailed search syntax for PubMed was as follows: (((maternal OR pregestational OR gestational) AND (diabetes OR “diabetes mellitus” OR hyperglycemia))) AND (“ADHD” OR “attention deficit” OR “hyperactivity syndrome” OR “attention deficit hyperactivity disorder”). The corresponding Chinese characters were used in CNKI database searching.
After the primary records were retrieved from databases, duplicated studies were removed. Then, the remaining records were checked according to titles and abstracts. Irrelevant studies were excluded during this step. After that, the full texts of the rest of the studies were obtained and reviewed in detail for eligibility according to the inclusion criteria. Finally, the qualified studies were included for further analyses.
Inclusion criteria
The inclusion criteria were established as follows: 1) original observational studies investigating the association between maternal diabetes and risk of ADHD in offspring, and 2) effect size (usually OR or risk ratio [RR]) and its 95% CI were reported, or the distribution of subjects in each comparison group was given so that the effect size was able to be calculated. Only English and Chinese literature was included. No restriction on diabetes subtype and study design was imposed. Review, editorial, and conference articles were excluded.
Data extraction
The following items were extracted independently by two reviewers from each study: first author, publication year, study design, characteristics of the participants, diagnostic criteria of ADHD and maternal diabetes, effect size with its 95% CI (preferentially adjusted effect size), and adjusted confounders. If the effect size was not reported, it was manually calculated from the original data. Any disagreement was resolved by further discussion. Since Caucasian usually includes modern population of Europe and white people in the US, we roughly classified participants from Europe and the US into Caucasian population when performing subgroup analyses.
Statistical analyses
The heterogeneity across studies was evaluated with Q-statistic, and the significance level was defined as 0.1.Citation16 Heterogeneity was further measured by I2 value and classified into high, medium, or low when I2 ≥50%, 50%> I2 ≥25%, or 25%> I2, respectively.Citation17 If an I2 was smaller than 25%, Mantel–Hansel’s method in fixed-effect model was used to pool outcomes, otherwise data were pooled based on Dersimonian and Laird method in random-effect model.Citation18 The effect size and its lower and higher CIs were natural logarithm transformed before data combining, and the result was natural exponential transformed and displayed. The publication bias was evaluated by the Egger’s linear regression test statistically.Citation16 Sensitivity analysis was performed with omitting each study and observing whether the synthesized result altered significantly. All statistical analyses were conducted by Stata 9.0 (StataCorp LP, College station, TX, USA). All P-values were two-sided and identified as significant if <0.05, unless otherwise specified.
Results
Characteristics of the included studies
As illustrated in , a total of nine studiesCitation8,Citation10–Citation14,Citation19–Citation21 involving 7,218,903 participants were included in the present analysis. The majority of themCitation8,Citation12–Citation14,Citation19,Citation20 were published in the recent 2 years. For baseline information, six studiesCitation10–Citation13,Citation19,Citation20 were cohort design and used RR or HR to measure the effect size. The remaining three studiesCitation8,Citation14,Citation21 were case-control studies, using OR to describe the risk. Over half of the studies were conducted in Nordic Europe,Citation8,Citation12–Citation14,Citation19 benefiting from the excellent local nationwide registry system. The rest of the studies were from China,Citation11 Greece,Citation20 Germany,Citation21 and USA.Citation10 Maternal type 1 diabetes (T1D) was investigated in five studies,Citation8,Citation12–Citation14,Citation19 while four studies did not give the accurate type of diabetes.Citation10,Citation11,Citation20,Citation21 Only one study recruited mothers with type 2 diabetes (T2D).Citation8 Three of the studiesCitation10,Citation11,Citation19 did not use multivariate analysis in order to consider the potential bias induced by confounders (for details see ). The quality of each study was assessed in using Newcastle-Ottawa Scale for nonrandomized studies. The overall quality levels were evaluated using the GRADE approach in .
Figure 1 Flow diagram of the identification of the eligible studies.
Table 1 Basic information of the included studies
Table 2 Quality of the included studies
Table 3 Evaluation of overall quality levels using the GRADE approach
Data synthesis of the case-control studies
The pooling of data from case-control studiesCitation8,Citation14,Citation21 demonstrated that maternal diabetes was not associated with ADHD in offspring (OR: 1.20, 95% CI: 0.96–1.49). Since all the case-control studies were conducted among Caucasian population, the findings should be applied to this race exclusively. High heterogeneity was detected (I2=74.5%) (). Sensitivity analysis indicated that omission of a given study would not reverse the insignificant result (). Egger’s test showed that no publication bias existed (t=1.67, P=0.194) ().
Figure 2 Main results of the meta-analyses.
Abbreviations: ES, effect size; GDM, gestational diabetes mellitus; T1D, type 1 diabetes; T2D, type 2 diabetes.
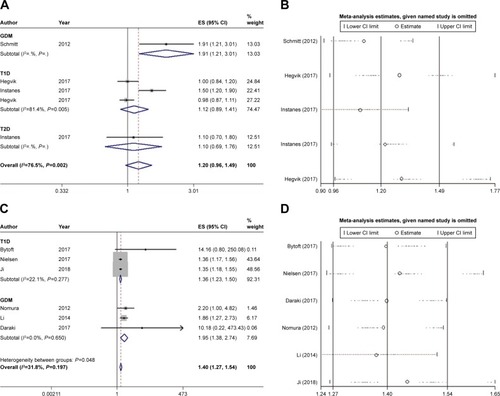
Table 4 Main results of the meta-analyses
Data synthesis of the cohort studies
In terms of cohort studies,Citation10–Citation13,Citation19,Citation20 the meta-analysis demonstrated that maternal diabetes increased the risk of ADHD in offspring by 40% (RR: 1.40, 95% CI: 1.27–1.54) (). Sensitivity analysis confirmed that the results were stable (). Unfortunately, publication bias was identified according to Egger’s test (t=6.56, P=0.003) (), indicating that the estimated effect was probably overstated due to publication of positive results. Since only the Li et al’sCitation11 study investigated the effect of maternal diabetes in Chinese, the remaining studies Citation10,Citation12,Citation13,Citation19,Citation20 that were conducted in Caucasian population demonstrated the risk in this race (RR: 1.37, 95% CI: 1.24–1.51). Subgroup analyses revealed that T1D increased the risk by 36% (RR: 1.36, 95% CI: 1.23–1.50).Citation12,Citation13,Citation19 No heterogeneity between studies were found in either overall or subgroup analyses.
Subgroup analysis of the cohort studies investigating mothers with GDM
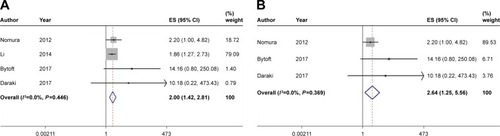
Since the participants in the cohort studies consisted of mothers with GDM and mothers with a history of diabetes (the onset of diabetes was not specified), we further narrowed the scope and investigated the effect of GDM on risk of ADHD for children. The combining of four studiesCitation10,Citation11,Citation19,Citation20 demonstrated that GDM heightened the risk of ADHD by onefold (RR: 2.00; 95% CI: 1.42–2.81), without detecting inconsistency between studies (I2=0%) (). Publication bias was also identified regarding this analysis. We next excluded Li et al’s studyCitation11 and ensured all the included studiesCitation10,Citation19,Citation20 were from Caucasian population. The risk of ADHD conferred by GDM in Caucasian was as much as 1.64-fold (95% CI: 1.25–5.56) higher compared with controls (). Besides, neither heterogeneity nor publication bias was detected ().
Figure 3 Meta-analyses of the subjects from (A) mothers with GDM or (B) Caucasian mothers with GDM.
Discussion
The present study is, to our knowledge, the first meta-analysis to evaluate the risk of ADHD for children induced by maternal diabetes. We systematically searched the databases and some of the included studies were nationwide investigations, and the number of subjects was large enough to obtain sufficient study power.Citation12,Citation13 The analyses generally consisted of two parts. On the one hand, combining of case-control studies demonstrated that the offspring of diabetic mothers were not at a heightened risk of ADHD (OR: 1.20, 95% CI: 0.96–1.49). All the case-control studies recruited Caucasian participants. Therefore, this finding should be restricted to this population. Of note, it has been suggested that some minority groups, such as obese or older Caucasian women, are at a greater risk for maternal diabetes than the overall Caucasian women.Citation22 This indicates that management of the high-risk subgroups by maternal DM intervention could be more beneficial for ADHD prevention. On the other hand, cohort studies altogether indicated that maternal diabetes was a risk factor for ADHD (RR: 1.40, 95% CI: 1.27–1.54). However, this result was not reliable considering publication bias was identified.
Since higher functions of brain develop during the second half of pregnancy, we hypothesized that GDM may exert adverse effects on offspring more profoundly in this period. When the participants were specified as offspring of mothers with GDM in Caucasian population from cohort studies, data pooling suggested that they were more vulnerable to ADHD and the risk was increased as much as by 1.64-fold (95% CI: 1.25–5.56). Although the sample size was relatively smaller (number of subjects in exposure group was 515, number of subjects in non-exposure group was 984,499) in this subgroup analysis, neither inconsistency nor publication bias was detected, indicating the reliability of this result. This result emphasizes the importance of good glycemic control in diabetic mothers throughout pregnancy and not only in the first trimester.
It has been hypothesized that ADHD may be due to inflammatory response to the central nervous system in the fetus caused by maternal inflammation and immune response. A nationwide study demonstrated that several immune system diseases, including maternal multiple sclerosis, rheumatoid arthritis, asthma and hypothyroidism, were more frequently observed among mothers of offspring with ADHD compared with mothers of controls.Citation8 Apart from the association regardless of gender, another large cross-sectional study reported that inflammatory bowel disease was associated with ADHD, particularly in females.Citation14 Considering that ADHD has an approximate sex ratio of 3:1 during childhood and displays sex-specific manifestations,Citation23 a sex-specific mechanism may underlie the relationship between ADHD and maternal immune disease, such as diabetes. Among the included studies, only one investigationCitation14 separately reported the association of maternal diabetes with ADHD in males and females. Although insignificant findings were shown in both males and females,Citation14 further studies exploring the difference between gender are encouraged for a better understanding of ADHD etiology.
Social factors have been suggested to play a crucial role on maternal diabetes and glycemic control, thus mediating the onset of ADHD. Most the included studiesCitation8,Citation13,Citation14,Citation20,Citation21 considered family socioeconomic status (SES), such as parental income, occupation, education, and single parent status, as a confounding variable and thereby adjusted the result. It is widely accepted that parental socioeconomic disadvantage is a risk factor for ADHD in children,Citation24 which is likely mediated by factors linked to low SES such as parental mental disorders. Diabetic mothers, especially for those with complications, are linked to low SES because those women might have limited ability to work and have lower disposable income, resulting in a relatively deprived environment for children. Apart from socioeconomic deprivation, lifestyle, access to health food, regular physical activity, public insurance, etc, are also linked to glycemic control.Citation25 Overall, it is recommended to record social factors and consider them as confounders when examining the true effect of maternal diabetes on ADHD in children. So the adjusted results were extracted and combined if available.
A new insight into the impact of in utero hyperglycemia on fetus brain development emphasizes that maternal diabetes may increase the vulnerability to psychiatric disorder later in life by interacting with other environmental insult during pregnancy. Animal model study has demonstrated that GDM and viral infection concurrently produce a novel transcriptional profile, and these novel transcriptional changes are associated with pathways implicated in psychiatric disorders.Citation26 This finding indicates that GDM may have the potential to prime the fetus for an exacerbating response to infection, which is a common environmental stress during pregnancy.
The mechanism of ADHD also has some endocrinological components. It has been shown that patients with T1D are more likely to receive ADHD diagnosis.Citation27 Interestingly, adolescents and young adults with ADHD are reportedly to be more likely than non-ADHD controls to develop T2D in later life.Citation28 There is an ongoing discussion whether thyroid hormone system is involved in the development of ADHD, and there is a link between thyroid hormones and diabetes risk.Citation29 In has been observed that thyroid-stimulating hormone levels are slightly increased among ADHD patients.Citation30 This finding is further validated by transgenic mouse that expresses a human mutant thyroid receptor β1, which manifests typical syndromes of ADHD such as impulsive and inattentive.Citation31
The National Institute for Health and Care Excellence accredited guidelines for ADHD management emphasized the importance of a holistic approach to managing ADHD.Citation32 A comprehensive shared treatment plan should address psychological, behavioral, and occupational or educational needs.Citation32 The guideline recommends an ADHD-focused group parent-training program to parents or carers as first-line treatment for children under 5 years with ADHD. Pharmacological medication is offered to children aged 5 years and over, young people, and adults, only if ADHD symptoms are still causing a significant impairment in interpersonal relationships, education and occupational attainment, or risk awareness.Citation32 However, a network meta-analysis of randomized trials indicated that the therapeutic effects of cognitive training, neurofeedback, antidepressants, antipsychotics, dietary therapy, fatty acids, and other complementary and alternative medicine were uncertain due to limited evidences.Citation33
The present studies consisted of cohort, cross-sectional, and case-control studies. Heterogeneity existed as a significant limitation for this review because of differences in ADHD definition, ethnicity, type of maternal diabetes, and methodology used. In order to reduce the heterogeneity between studies included in the review, the studies that were similar regarding design and measurement were combined. Another noteworthy fact was that we included the studies in which prescriptions were used as proxy for the diagnosis of ADHD,Citation8,Citation14,Citation19 and thus selection bias might occur. Due to various health care systems and policies in different countries, medications are accepted by different subgroups of children who may have been diagnosed with ADHD. However, medication for ADHD does not necessarily mean a clinical diagnosis has been given. Therefore, the identification of ADHD cases in further studies should be based on a standardized scale so that the selection bias could be diminished.
Conclusion
Maternal diabetes, especially for GDM, is probably a risk factor for ADHD in Caucasian race. This result emphasizes the importance of good glycemic control in diabetic mothers throughout pregnancy and not only in the first trimester. The attention on gender difference, the clear record of significant confounders, and the accurate diagnosis of ADHD cases are urgently needed in the further studies.
Disclosure
The authors report no conflicts of interest in this work.
References
- ThomasRSandersSDoustJBellerEGlasziouPPrevalence of attention-deficit/hyperactivity disorder: a systematic review and meta-analysisPediatrics20151354e994e100125733754
- Beau-LejdstromRDouglasIEvansSJWSmeethLLatest trends in ADHD drug prescribing patterns in children in the UK: prevalence, incidence and persistenceBMJ Open201666e010508
- GrimmOKittel-SchneiderSReifARecent developments in the genetics of ADHDPsychiatry clin Neurosci201872965467229722101
- PolańskaKJurewiczJHankeWExposure to environmental and lifestyle factors and attention-deficit/hyperactivity disorder in children – a review of epidemiological studiesInt J Occup Med Environ Health201225433035523086631
- SchroederSRMental retardation and developmental disabilities influenced by environmental neurotoxic insultsEnviron Health Perspect2000108Suppl 339539910852834
- BytoftBKnorrSVlachovaZLong-term cognitive implications of intrauterine hyperglycemia in adolescent offspring of women with type 1 diabetes (the EPICOM study)Diabetes Care20163981356136327271191
- OrnoyAReeceEAPavlinkovaGKappenCMillerRKEffect of maternal diabetes on the embryo, fetus, and children: congenital anomalies, genetic and epigenetic changes and developmental outcomesBirth Defects Res C Embryo Today20151051537225783684
- InstanesJTHalmøyAEngelandAHaavikJFuruKKlungsøyrKAttention-deficit/hyperactivity disorder in offspring of mothers with inflammatory and immune system diseasesBiol Psychiatry201781545245926809250
- BanikAKandilyaDRamyaSStünkelWChongYDheenSMaternal factors that induce epigenetic changes contribute to neurological disorders in offspringGenes (Basel)201786150
- NomuraYMarksDJGrossmanBExposure to gestational diabetes mellitus and low socioeconomic status: effects on neurocognitive development and risk of attention-deficit/hyperactivity disorder in offspringArch Pediatr Adolesc Med2012166433734322213602
- LiJZhongHLiangZCXyLStudy on correlation between gestational diabetes merged pregnancy-induced hypertension and hyperactivity syndrome in childrenJ Clin Exp Med2014131915831585
- NielsenPRBenrosMEDalsgaardSAssociations between autoimmune diseases and attention-deficit/hyperactivity disorder: a nationwide studyJ Am Acad Child Adolesc Psychiatry2017563234240.e128219489
- JiJChenTSundquistJSundquistKType 1 diabetes in parents and risk of attention deficit/hyperactivity disorder in offspring: a population-based study in SwedenDiabetes Care201841477077429374069
- HegvikTAInstanesJTHaavikJKlungsøyrKEngelandAAssociations between attention-deficit/hyperactivity disorder and autoimmune diseases are modified by sex: a population-based cross-sectional studyEur Child Adolesc Psychiatry201827566367528983730
- MoherDLiberatiATetzlaffJAltmanDGPRISMA GroupPreferred reporting items for systematic reviews and meta-analyses: the PRISMA statementPLoS Med200967e100009719621072
- EggerMSmithGDSchneiderMMinderCBias in meta-analysis detected by a simple, graphical testBMJ199731571096296349310563
- HigginsJPTThompsonSGQuantifying heterogeneity in a meta-analysisStat Med200221111539155812111919
- DersimonianRLairdNMeta-analysis in clinical trialsControl Clin Trials1986731771883802833
- BytoftBKnorrSVlachovaZAssessment of attention deficits in adolescent offspring exposed to maternal type 1 diabetesPLoS One2017121e016930828072839
- DarakiVRoumeliotakiTKoutraKEffect of parental obesity and gestational diabetes on child neuropsychological and behavioral development at 4 years of age: the Rhea mother–child cohort, Crete, GreeceEur Child Adolesc Psychiatry201726670371428050707
- SchmittJRomanosMPrenatal and perinatal risk factors for attention-deficit/hyperactivity disorderArch Pediatr Adolesc Med2012166111074107522965737
- HeddersonMEhrlichSSridharSDarbinianJMooreSFerraraARacial/ethnic disparities in the prevalence of gestational diabetes mellitus by BMIDiabetes Care20123571492149822619080
- FaraoneSVAshersonPBanaschewskiTAttention-deficit/hyperactivity disorderNat Rev Dis Primers20154915020
- RussellAEFordTWilliamsRRussellGThe association between socioeconomic disadvantage and attention deficit/hyperactivity disorder (ADHD): a systematic reviewChild Psychiatry Hum Dev201647344045826266467
- ColicchiaLCParviainenKChangJCSocial contributors to glycemic control in gestational diabetes mellitusObstet Gynecol201612861333133927824747
- MoneyKMBarkeTLSerezaniAGestational diabetes exacerbates maternal immune activation effects in the developing brainMol Psychiatry201823919
- KapellenTMReimannRKiessWKostevKPrevalence of medically treated children with ADHD and type 1 diabetes in Germany – Analysis of two representative databasesJ Pediatr Endocrinol Metab201629111293129727754966
- ChenMHPanTLHsuJWRisk of type 2 diabetes in adolescents and young adults with attention-deficit/hyperactivity disorderJ Clin Psychiatry2018793 pii: 17m11607
- CrunkhornSPattiMELinks between thyroid hormone action, oxidative metabolism, and diabetes risk?Thyroid200818222723718279023
- CakalozBAkayAPBoberEYulugBThyroid function and oppositional defiant disorder: more than a coincidence in prepubertal boys with attention-deficit hyperactivity disorder?J Neuropsychiatry Clin Neurosci2011232E9E10
- SiesserWBZhaoJMillerLRChengSYMcDonaldMPTransgenic mice expressing a human mutant beta1 thyroid receptor are hyperactive, impulsive, and inattentiveGenes Brain Behav20065328229716594981
- NICEAttention deficit hyperactivity disorder: diagnosis and management2018 Available from: www.nice.org.uk/guidance/NG87Accessed January 1, 2019
- Catalá-LópezFHuttonBNúñez-BeltránAThe pharmacological and non-pharmacological treatment of attention deficit hyperactivity disorder in children and adolescents: a systematic review with network meta-analyses of randomised trialsPLoS One2017127e018035528700715