Abstract
Lennox–Gastaut syndrome (LGS) is a devastating childhood epilepsy syndrome characterized by the occurrence of multiple types of seizures and cognitive decline. Most children suffer from frequent seizures that are refractory to current medical management. Recent clinical trials have suggested that addition of clobazam may improve the clinical outcome for some LGS patients. Although clobazam has been available for over five decades, it has only recently been approved by the US Food and Drug Administration for this indication. As a 1,5-benzodiazepine, clobazam is structurally related to the widely used 1,4-benzodiazepines, which include diazepam. Clobazam has been shown to modulate GABAergic neurotransmission by positive allosteric modulation of GABAA receptors, and to increase expression of transporters for both GABA and glutamate. The active metabolite n-desmethylclobazam (norclobazam) also modulates GABAA receptors, and the relative importance of these two compounds in the clinical effectiveness of clobazam remains an open question. Clinical trials involving clobazam as an addon therapy in a variety of pediatric epilepsy populations have found a significant improvement in seizure control. In patients with LGS, clobazam may have greatest efficacy for drop seizures. Longstanding clinical experience suggests that clobazam is a safe and well tolerated antiepileptic drug with infrequent and mild adverse effects. These results suggest that adjunctive treatment with clobazam may be a reasonable option for LGS patients, particularly those who are treatment-resistant.
Lennox–Gastaut syndrome
Lennox–Gastaut syndrome (LGS) is a catastrophic epileptic encephalopathy with a poor prognosis and limited treatment options. Although rare, LGS constitutes 3%–10% of childhood epilepsies, due to its intractable nature.Citation1–Citation5 Generally, LGS onset occurs before 8 years of age, with a peak at 3–5 years,Citation5–Citation7 and is more common in males.Citation1,Citation6,Citation8 LGS is identified by its characteristic triad of symptoms, including multiple generalized seizure types, a slow spike and wave (≤2.5) pattern in the awake electroencephalogram, and cognitive decline. The types of seizures most commonly associated with LGS are tonic, atypical absence, myoclonic, and atonic seizures,Citation5,Citation6 but many LGS patients also experience generalized tonic-clonic and focal seizures.Citation2,Citation4,Citation6,Citation9,Citation10 In addition to the slow spike and wave pattern, bursts of paroxysmal fast activity during sleep are also classically present on the electroencephalogram and may be associated with subtle tonic seizures.Citation1,Citation5,Citation6 Up to 90% of patients with LGS have mental retardation and experience cognitive deterioration,Citation2,Citation3 and many children also develop behavioral and psychological problems, including aggression, hyperactivity, and characteristics of autism.Citation3,Citation5,Citation11
LGS often results from an underlying neurological injury or disorder, such as hypoxic-ischemic encephalopathy, cerebral palsy, tuberous sclerosis complex, or cortical dysplasia, but approximately 30% of LGS cases are cryptogenic, having no clear cause.Citation1,Citation5–Citation7 Diagnosis is difficult and may take years because in addition to the various etiologies of LGS, the syndrome lacks a uniform clinical presentation,Citation6 and often patients do not have all of the diagnostic elements at the onset of epilepsy.Citation5 LGS is resistant to treatment and often, in part due to the multiple seizure types, a combination of antiepileptic drugs is required.Citation3,Citation6–Citation8,Citation12 LGS is considered an epileptic encephalopathy, in which the degree of cognitive deterioration present is thought to be related to seizure frequency and burden of epileptic discharges.Citation4,Citation5,Citation11
Current treatment options
A broad spectrum antiepileptic drug or combination of antiepileptic drugs is frequently necessary to treat the multiple seizure types associated with LGS.Citation3,Citation6–Citation8,Citation12 Valproate is often used as a first-line treatment for LGS by many physicians because it is effective for both generalized and focal seizures and is not known to worsen any seizure types associated with LGS.Citation13,Citation14 However, valproate is rarely effective as monotherapyCitation3 and has not been approved by the US Food and Drug Administration for this purpose.Citation3,Citation6,Citation12,Citation15 Adverse events related to valproate use can be serious, including hepatic toxicity and pancreatitis, and there are many potential drug interactions.Citation16
Felbamate, lamotrigine, topiramate, and rufinamide are all approved by the Food and Drug Administration as adjunctive treatments for LGS. Each of these antiepileptic drugs has been tested in randomized, double-blind, placebo-controlled clinical trials demonstrating their efficacy for seizures associated with LGS.Citation3,Citation7,Citation12 There have been no studies comparing approved treatment options for LGS patients,Citation15 and comparing results from different trials is complicated by variations in study populations, concurrent use of other antiepileptic drugs, and differences in the types of reported data.Citation3,Citation7 A Cochrane database review of treatment options for LGS included seven randomized, controlled studies that evaluated rufinamide, lamotrigine, cinromide, felbamate, thyrotropin-releasing hormone, and topiramate in children and adults with LGS.Citation7 In each of these studies, the drug being evaluated was compared with placebo, with the exception of a study evaluating thyrotropin-releasing hormone, which compared low-dose and high-dose efficacy. In their review, Hancock and CrossCitation7 concluded that an optimum treatment option could not be identified from these studies, but that lamotrigine, rufinamide, topiramate, and felbamate may be useful as adjunctive therapies.
Felbamate was the first antiepileptic drug approved for use as addon therapy for LGS.Citation3 Since its approval in 1993, felbamate has been associated with aplastic anemia and hepatic failure, and due to these severe adverse events, its use has been limited to patients who have not responded to other antiepileptic drugs.Citation17–Citation19 Lamotrigine, approved as an adjunctive treatment for LGS in 1998, is a broad spectrum antiepileptic drug that is effective against multiple seizure types.Citation20–Citation22 The most common side effect of lamotrigine is a mild skin rash,Citation21,Citation23,Citation24 but Stevens–Johnson syndrome and toxic epidermal necrolysis have occurred in rare cases.Citation22,Citation23 Drug interactions with lamotrigine are common, complicating its use in combination therapy.Citation25 Topiramate, approved for use in LGS in 2001, lacks the risk of life-threatening adverse events, like those associated with lamotrigine and felbamate,Citation3 but has been associated with cognitive impairment,Citation26–Citation28 although this can often be minimized by slow titration.Citation3,Citation10,Citation15 Rufinamide, approved in 2011, may be particularly effective for drop seizures (due to either tonic or atonic events) in children with LGS.Citation29 Rufinamide has been associated with somnolence and vomiting,Citation29 which can be mitigated by slowed titration.Citation30
If pharmacological treatment fails, other options include the ketogenic diet, vagus nerve stimulation, corpus callosotomy, and resective surgery.Citation3,Citation6,Citation12 The ketogenic diet, ie, a high-fat, low-protein, and low-carbohydrate diet, has been shown to decrease drop seizure frequency in patients who do not respond to antiepileptic drugs, including patients with LGS.Citation31–Citation34 In studies of the ketogenic diet in the treatment of children with refractory epilepsy including LGS, the diet provided complete seizure control for more than 50% of patients.Citation34 Common side effects include gastrointestinal symptoms, such as nausea, vomiting, and constipation, which may be improved by decreasing the nonlipid to lipid ratio. Compliance with the diet may also be difficult to maintain in patients with cognitive and behavioral problems.Citation15 Although vagus nerve stimulation is not as effective in patients with LGS as it is in patients with partial epilepsy,Citation35 it has been demonstrated to decrease seizure frequency with minimal adverse effects.Citation35–Citation37 Corpus collosotomy is used to decrease the spread of epileptic discharges between hemispheres and can be helpful for patients with intractable drop attacks.Citation38 There may be a seizure focus in symptomatic cases of LGS such as those caused by tuberous sclerosis or cortical dysplasia, in which case resective surgery may be effective.Citation12,Citation39
Each of the approved antiepileptic drugs is effective for some patients, but many LGS patients continue to have seizures even with the use of multiple antiepileptic drugs, and combination therapy puts these patients at increased risk for experiencing side effects.Citation1,Citation7,Citation8 It is clear that new options are necessary for these treatment-resistant patients. One such option is the use of clobazam, a 1,5-benzodiazepine, which may be particularly effective in pediatric populations.
Clobazam, a 1,5-benzodiazepine
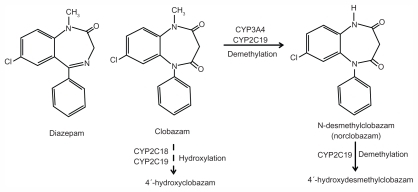
Clobazam was initially proposed as an effective anticon-vulsant and anxiolytic with an improved side effect profile compared with the 1,4-benzodiazepines, which include diaz-epam and clonazepam ().Citation2,Citation40,Citation41 The original reportCitation42 found clobazam to be effective in several animal models of acute seizures, and it was first reported to have therapeutic activity in patients with a variety of seizure disorders by Gastaut and Low in 1979.Citation43 Clobazam (marketed under the brand names Frisium®, Urbanyl®, Onfi, and Mystan®) is now available in many countries as adjunctive therapy for several types of seizures.
Figure 1 Clobazam (7-chloro-1-methyl-5-phenyl-1,5-benzodiazepine-2,4-dione). Structures of diazepam, clobazam, and norclobazam and major metabolic pathways for clobazam and norclobazam.
Clobazam acts primarily through positive allosteric modulation of GABAA receptors, a mechanism of action shared by all clinically useful benzodiazepines. These ligandgated chloride channels are responsible for fast inhibitory neurotransmission throughout the central nervous system, and drugs that enhance their activity are often effective anxiolytics, sedatives, and anticonvulsants. While the benzodiazepines are widely considered to be safe and effective for the treatment of acute seizures, their clinical utility for long-term therapy is often limited by side effects and the development of tolerance.Citation41
Metabolism of clobazam
The primary pathway for metabolism of clobazam is demethylation by cytochrome P450 (CYP)3A4 and CYP2C19 to its active metabolite n-desmethylclobazam (norclobazam, ).Citation44 Clobazam can be hydroxylated to an inactive form, but this appears to be a minor pathway. CPY2C19 also acts on norclobazam, inactivating it through hydroxylation.Citation44,Citation45 Since norclobazam itself is an anticonvulsant, an increase in its levels through inhibition of CYP2C19 can greatly increase the duration of therapeutic effect. Mutations in CYP2C19 that reduce its activity are relatively common, with nearly 3% of Caucasians and up to 20% of Asians characterized as “poor metabolizers”.Citation46 In epileptic patients treated with clobazam, the norclobazam to clobazam ratio was found to be dramatically higher in those with mutations in CYP2C19.Citation44,Citation47,Citation48 Interestingly, one study found that clobazam therapy was more effective in patients with defective CYP2C19 alleles, with no correlation to adverse side effects,Citation49 which may suggest a prominent role for norclobazam in determining the therapeutic benefits. However, others have reported an increased occurrence of side effects, primarily sedation, with clobazam administration in patients carrying CYP2C19 mutations, and clobazam doses may need to be reduced for some in this patient population.Citation47
Studies in animal models of seizure and epilepsy
Clobazam has demonstrated effectiveness in a wide variety of animal models, including acute and chronic seizures and genetic forms of epilepsy.Citation2,Citation50 In recent studies, clobazam generally showed efficacy similar to that of the 1,4- benzodiazepines, albeit with lower potency when compared with diazepam or clonazepam.Citation51–Citation54 The side effect profile, development of tolerance, and withdrawal hyperexcitability produced by clobazam were all similar to that seen with diazepam in these animal models.Citation51 However, the activity of clobazam was not identical to the 1,4-benzodiazepines in all cases, because clobazam was found to be more effective in a model of inherited epilepsy,Citation53 and had a distinct profile of activity against acute seizures.Citation51
Activity at GABAA receptors
A variety of studies have clearly shown that, like the 1,4-benzodiazepines, clobazam is a positive allosteric modulator of GABAA receptors. Direct enhancement of the response by clobazam to applied GABA was demonstrated in cultured corticalCitation55 and cerebellarCitation56 neurons, and clobazam was also found to slow the decay of miniature inhibitory post-synaptic currents in brain slices from rat hippocampus.Citation57
Neuronal GABAA receptors are structurally heterogeneous, and the pentameric channel can be assembled from a combination of at least 16 different subunit subtypes (including α1–6, β1–3, γ1–3, δ, ɛ, π, and θ).Citation58 These subunits show different patterns of expression throughout the brain, and their levels change throughout development and in response to pathological conditions, including seizure activity.Citation59 The subunit composition of the receptor greatly influences its pharmacological properties.
Benzodiazepine agonists do not modulate receptors containing α4 or α6 subunits, and require the presence of a γ subunit.Citation60 Clobazam appears to share the same binding site as other benzodiazepine agonists, because a mutation in the γ subunit had a similar effect on potency of both diazepam and clobazam.Citation61 However, clobazam and norclobazam have been tested directly on very few GABAA receptor isoforms, and no comprehensive studies of the subunit dependence of their activity have been reported for either compound.
The modulatory activity of clobazam, norclobazam, and diazepam was compared at recombinant α3β3γ2 receptors,Citation62 which is likely to be a significant isoform in the developing brain.Citation59 In that study, clobazam had efficacy similar to that of diazepam, but lower potency, consistent with the higher clobazam doses required in animal studies. Relative to one another, norclobazam and clobazam had similar potency at these receptors, although norclobazam showed lower efficacy. Citation62 Few other studies have been performed to examine the possible subunit dependence of clobazam or norclobazam activity at GABAA receptors. Clobazam was shown to enhance the response of α1β2γ1 receptors modestlyCitation63 and to bind to an α5-containing receptor population from rat hippocampus with characteristics similar to those of diazepam. Citation64 It is important to understand whether clobazam or norclobazam show a different pattern of subunit selectivity compared with other benzodiazepines, which might explain the distinct characteristics associated with clobazam. Drugs that modulate different receptor populations would be expected to have unique effects on seizure activity, sedation, and anxiety,Citation65,Citation66 and could also produce different levels of tolerance development and abuse potential.Citation67
In addition to direct modulation of GABAA receptor activity, clobazam was shown to cause a region-specific increase in expression of transporters for GABA (GAT3) and glutamate (GLT-1) in an animal model of temporal lobe epilepsy. Citation68 This alteration may have been an indirect effect from the reduction in seizure activity, because clobazam had no effect on transporter levels in control (seizure-free) animals. The impact of these changes in the clinical effectiveness of clobazam is not known, but an increase in GLT-1 could potentially reduce the high hippocampal glutamate levels associated with epileptogenesis in animal models of temporal lobe epilepsy.Citation69 Modulation of voltage-gated Na+ and Ca2+ channels by clobazam has also been suggested by some authors,Citation2,Citation70 although no studies have demonstrated a direct action at these channels.
Does norclobazam have a therapeutic role?
It is clear that norclobazam is an active metabolite of clobazam, with direct anticonvulsant activity both in animal models of epilepsy and in patients with refractory epilepsy.Citation70 Less clear are the relative roles of each of these compounds in the therapeutic and side effect profiles of clobazam. In epilepsy patients, the degree of seizure control was correlated with blood levels of norclobazam rather than clobazam.Citation72 Studies with both neurons and recombinant expression systems have shown that norclobazam acts as a positive allosteric modulator of GABAA receptors, with a similar potency but lower efficacy than clobazam.Citation55,Citation62 It has been suggested that partial agonists at modulatory sites might have improved side effect profiles compared with full agonists,Citation73 and indeed, norclobazam was associated with reduced development of tolerance compared with clobazam in a mouse seizure model.Citation71 However, very few studies have directly examined the properties of norclobazam. If norclobazam is a primary mediator of the anticonvulsant effects of clobazam, further studies into its mechanism(s) of action are warranted.
Clinical trials in Lennox–Gastaut syndrome and other pediatric epilepsies
Clobazam was first synthesized in the 1960s and is approved for use as an antiepileptic drug in over 100 countries.Citation2 Thus, longstanding clinical experience indicates that clobazam is a safe and effective addon therapy for many patients (). In many countries, clobazam has been used as a first-line antiepileptic drug in pediatric epilepsy, and in spite of other options becoming available, it continues to be used as an adjunctive therapy for patients with treatment-resistant epilepsy.Citation74–Citation76 In the US, until its October 2011 approval by the Food and Drug Administration, clobazam was only obtained from foreign pharmacies and paid for out-of-pocket by patients. Thus, the use of clobazam in the US was typically limited to patients with severe epilepsy that had proven refractory to multiple medication options.Citation30,Citation77 However, clobazam is anticipated to be more widely available from early 2012 for LGS patients. Clobazam was granted orphan drug status by the Food and Drug Administration in December 2008, and a new drug application submitted in March 2011 for use in children with LGS was approved in October 2011.
Table 1 Clobazam as addon therapy in refractory pediatric epilepsy
In six open-label prospective studies evaluating the efficacy of clobazam as addon therapy for pediatric patients with refractory epilepsy, 54%–85% of patients experienced at least a 50% decrease in seizure frequencyCitation74,Citation78–Citation83 (). These studies included a total of 423 patients, with 98 patients identified as having LGS. Most studies did not provide distinct data for the LGS population, but SugaiCitation80 reported that 62% of LGS patients in the group evaluated for short-term efficacy and half of LGS patients followed for at least 6 months had a 50% or greater decrease in seizure frequency on clobazam. In another study, 64% of 25 patients with LGS achieved at least a 50% decrease in seizure frequency.Citation74 Jan and ShaabatCitation79 noted that three of the 14 LGS patients included in their study continued to have daily seizures while taking clobazam, a higher proportion than in the rest of the study population.
Two retrospective studies on the efficacy of clobazam as addon therapy for pediatric patients also reported significant reductions in seizure frequencyCitation84,Citation85 (). Da Silveira et alCitation84 evaluated 100 patients who received clobazam as addon therapy for refractory focal epilepsy, and 33% of these patients had a 75% or greater decrease in seizure frequency. Silva et alCitation85 reviewed the efficacy of clobazam as addon therapy for 97 pediatric patients with epileptic encephalopathies. Of the patients in this study, 28 had LGS. Thirty-seven percent of all patients had a 50% or greater decrease in seizure frequency, and complete seizure control was achieved in nine patients.
In 1990, Keene et alCitation86 reported the results of a double-blind, placebo-controlled, crossover study evaluating clobazam as addon therapy in 21 patients aged 2–19 years with refractory epilepsy. Fifty-two percent of patients in the clobazam arms had a 50% or greater decrease in seizure frequency. More recently, Conry et alCitation8 reported the results of a multicenter, double-blind Phase II study evaluating low-dose (0.25 mg/kg/day) or high-dose (1 mg/kg/day) clobazam in 68 patients with LGS, aged 2–26 years. Eighty-three percent of patients in the high-dose group had a 50% or greater reduction in seizure frequency compared with baseline. In addition to decreased seizure frequency, patients had improved global assessments on both high-dose and low-dose clobazam,Citation8 consistent with prior work suggesting improved cognitive and behavioral performance on clobazam.Citation74,Citation78 Following the encouraging results of the Phase II study, a multicenter, randomized, double-blind, Phase III study was performed.Citation87 This study evaluated the efficacy of low-dose (0.25 mg/kg/day), medium-dose (0.5 mg/kg/day), and high-dose (1 mg/kg/day) clobazam versus placebo as addon therapy for 238 patients with LGS, aged 2–54 years. Fifty-eight percent of patients in the medium-dose group and 77% of patients in the high-dose group had a 50% or greater decrease in seizure frequency. Improved global assessments were reported for patients in all dosage groups compared with placebo.
Adverse effects in epilepsy patients
Adverse effects from clobazam are generally similar to those of the other benzodiazepines, but perhaps less frequent. Conry et alCitation8 reported little difference in the occurrence of side effects in patients receiving clobazam 0.25 mg/kg/day and those receiving 1.0 mg/kg/day. The most common adverse effect is somnolence, reported by 9%–19% of patients.Citation8,Citation78,Citation81,Citation84 Other common side effects include behavioral abnormalities, irritability, ataxia, and drooling, each occurring in under 10% of patients.Citation8,Citation81,Citation84 Notably, in spite of the efficacy observed in many patients, an increase in seizures, worsening of seizures, or development of new seizure types have been reported in up to 5%–13% of patients.Citation8,Citation74,Citation80,Citation84 In the only double-blind trial, Conry et alCitation8 reported 13% with adverse events related to seizures, each mild or moderate in severity, and more common in the low-dose clobazam group than in the high-dose group. Other studies reporting adverse seizure-related events were open-label, prospective,Citation74,Citation80 or retrospectiveCitation84 in nature without randomization or control arms. Because the rate and types of seizures often fluctuate over several weeks or months in patients with LGS, it remains unclear whether these episodes of seizure worsening are related to clobazam administration.Citation3,Citation8
Tolerance is an issue with many antiepileptic drugs, especially benzodiazepines, and the loss of efficacy of clobazam in some patients has been noted. Reports of the development of tolerance among published studies varied from as few as 10% to as many as 87% of patients.Citation81,Citation84 For up to 70% of patients who developed tolerance, efficacy returned after stopping and reintroducing clobazam after 2–3 months or after increasing the dosage.Citation74,Citation80,Citation81 Others noted persistent efficacy for more than one year in as many as 85% of patients who experienced improved seizure control, and some patients maintained complete seizure control during this time.Citation85
Clobazam is typically initiated at a low dose, often 5 mg/ day or 0.1 mg/kg/day for smaller patients, and increased at 5–7 day intervals until a minimum effective dose is reached or side effects occur.Citation74,Citation79 Studies have suggested that slow titration may help avoid adverse effects and that when present, side effects may be reduced or eliminated with dose reduction.Citation79,Citation80 Doses of 0.2–3.8 mg/kg/dayCitation2,Citation73 have been used in trials evaluating the use of clobazam (). In our experience, doses up to 2 mg/kg/day divided into twice daily doses are often required. Rarely, higher doses up to 3 mg/kg/day are required and tolerated.
Interactions with stiripentol and other antiepileptic drugs
Clobazam has been coadministered with a wide variety of other antiepileptic drugs, with few reported harmful drug– drug interactions. Any inhibitors or inducers of CYP2C19 can have an impact on clobazam and norclobazam levels, and coadministration of CYP2C19 inhibitors has been successfully used to enhance the duration and efficacy of clobazam treatment, possibly by increasing levels of norclobazam. This interaction seems particularly beneficial when clobazam is coadministered with stiripentol (Diacomit®), an antiepileptic drug, which is both a GABAA receptor modulator and a potent CYP2C19 inhibitor.Citation88–Citation90 Clobazam and stiripentol act via separate mechanisms at the GABAA receptorCitation57,Citation62 and stiripentol can dramatically increase norclobazam levels.Citation45 Animal studies have demonstrated a significant positive interaction between clobazam and stiripentol, with both an additive pharmacodynamic interaction and a large increase in the brain concentration of clobazam.Citation54 The combination of clobazam with stiripentol is widely used in the treatment of patients with Dravet syndrome (severe myoclonic epilepsy of infancy).Citation88 In contrast with its possibly beneficial interaction with stiripentol, clobazam has also been reported to inhibit the metabolism of valproate, so has the potential to increase valproateassociated toxicity.Citation91 Overall, clobazam is generally well tolerated when combined with most of the antiepileptic drugs commonly used in clinical practice.
Summary
LGS is an epileptic encephalopathy with childhood onset that is characterized by multiple seizure types and an intractable nature. LGS is also associated with a number of cognitive and behavioral problems that progress over time, often even after seizure control has improved. Clobazam has been demonstrated to decrease the overall rate of seizures in patients with LGS, with a significant reduction in the frequency of drop seizures, often considered to be the most disabling type of seizure associated with the syndrome.Citation3,Citation6,Citation10,Citation12 Improved global assessments for patients on clobazam have been noted, which may warrant further investigation. Hancock and CrossCitation7 reported that the behavioral and cognitive deterioration associated with LGS are the symptoms that are hardest to cope with for many families. Further work needs to be done to characterize fully the activity of both clobazam and norclobazam, its active metabolite, at different GABAA receptor populations and to optimize the incorporation of clobazam into a treatment plan.
Clobazam has been used as a first-line treatment in many countries, and is now frequently used as an adjunctive therapy for patients with refractory epilepsy. Its recent approval by the Food and Drug Administration will now allow its use for LGS patients in the US. The antiepileptic drugs currently approved for the treatment of LGS are not effective for all patients and each is associated with significant side effects. Other safe and effective options for treatment-resistant patients are needed, and recent studies of clobazam suggest that it may be an effective and well tolerated option for patients with LGS.
Disclosure
The authors report no conflicts of interest in this work.
References
- MarkandOLennox-Gastaut syndrome (childhood epileptic encephalopathy)J Clin Neurophysiol200320642644114734932
- NgYTCollinsSDClobazamNeurotherapeutics20074113814417199029
- van RijckevorselKTreatment of Lennox-Gastaut syndrome: overview and recent findingsNeuropsychiatr Dis Treat2008461001101919337447
- MichoulasAFarrellKMedical management of Lennox-Gastaut syndromeCNS Drugs201024536337420158289
- CamfieldPDefinition and natural history of Lennox-Gastaut syndromeEpilepsia201152Suppl 53921790560
- ArzimanoglouAFrenchJBlumeWLennox-Gastaut syndrome: a consensus approach on diagnosis, assessment, management, and trial methodologyLancet Neurol200981829319081517
- HancockECCrossHHTreatment of Lennox-Gastaut syndromeCochrane Database Syst Rev200983CD00327719588340
- ConryJANgYTPaolicchiJMClobazam in the treatment of Lennox-Gastaut syndromeEpilepsia20095051158116619170737
- ShieldsWDCatastrophic epilepsy in childhoodEpilepsia200041Suppl 2S2610885734
- TrevathanEInfantile spasms and Lennox-Gastaut syndromeJ Child Neurol200217Suppl 22S92S2211952036
- CamfieldPCamfieldCEpileptic syndromes in childhood: clinical features, outcomes, and treatmentEpilepsia200243Suppl 3273212060004
- MontourisGRational approach to treatment options for Lennox-Gastaut syndromeEpilepsia201152Suppl 5102021790561
- WhelessJWClarkDFCarpenterDTreatment of pediatric epilepsy: expert opinion, 2005J Child Neurol200520Suppl 1S15616615562
- WhelessJWClarkeDFArzimanoglouACarpenterDTreatment of pediatric epilepsy: European expert opinion, 2007Epileptic Discord200794353412
- SchmidtDBourgeoisBA risk-benefit assessment of therapies for Lennox-Gastaut syndromeDrug Saf200022646747710877040
- BryantAEDreifussFEValproic acid hepatic fatalities. III. US experience since 1986Neurology19964624654698614514
- O’NeilMGPerdunCSWilsonMBMcGownSTPatelSFelbamate-associated fatal acute hepatic necrosisNeurology1996465145714598628501
- KaufmanDWKellyJPAndersonTHarmonDCShapiroSEvaluation of case reports of aplastic anemia among patients treated with felbamateEpilepsia19973812126512699578520
- PellockJMFaughtELeppikIEShinnarSZupancMLFelbamate: consensus of current clinical experienceEpilepsy Res2006712–38910116889941
- DonaldsonJAGlauserTAOlberdingLSLamotrigine adjunctive therapy in childhood epileptic encephalopathy (the Lennox Gastaut Syndrome)Epilepsia199738168739024186
- FarrellKConnollyMBMunnRPengSMacWilliamsLMProspective, open-label, add-on study of lamotrigine in 56 children with intractable generalized epilepsyPediatr Neurol19971632012059165509
- MotteJTrevathanEArvidssonJFBarreraMNMullensELManascoPLamotrigine for generalized seizures associated with the Lennox-Gastaut syndrome. Lamictal Lennox-Gastaut Study GroupN Engl J Med199733725180718129400037
- DooleyJCamfieldPGordonKCamfieldCWirrellESmithELamotrigine-induced rash in childrenNeurology19964612402428559384
- SchlumbergerEChavezFPlaciosLReyEPajotNDulacOLamotrigine in treatment of 120 children with epilepsyEpilepsia19943523593678156958
- KannerAMFreyMAdding valproate to lamotrigine: a study of their pharmacokinetic interactionNeurology200055458859110953201
- FaughtEWilderBJRamsayRETopiramate placebo-controlled dose-ranging trial in refractory partial epilepsy using 200-, 400-, and 600-mg daily dosagesNeurology1996466168416908649570
- MartinRKuznieckyRHoSCognitive effects of topiramate, gabapentin, and lamotrigine in healthy young adultsNeurology19995223213279932951
- ThompsonPJBaxendaleSADuncanJSSanderJWEffects of topiramate on cognitive functionJ Neurol Neurosurg Psychiatry200069563664111032616
- GlauserTKlugerGSachdeoRKraussGPerdomoCArroyoSRufinamide for generalized seizures associated with Lennox-Gastaut syndromeNeurology200870211950195818401024
- Chu-ShoreCJThieleEANew drugs for pediatric epilepsySemin Pediatr Neurol201017421422321183127
- FreemanJMViningEPPillasDJPyzikPLCaseyJCKellyMTThe efficacy of the ketogenic diet-1998: a prospective evaluation of intervention in 150 childrenPediatrics19981026135813639832569
- FreemanJMViningEPKossoffEHPyzikPLYeXGoodmanSNA blinded, crossover study of the efficacy of the ketogenic dietEpilepsia200950232232518717710
- ViningEPFreemanJMBallaban-GilKA multicenter study of the efficacy of the ketogenic dietArch Neurol19985511143314379823827
- SeoJHLeeYMLeeJSJangHCKimHDEfficacy and tolerability of the ketogenic diet according to lipid:nonlipid ratios – comparison of 3:1 with 4:1 dietEpilepsia200748480180517386059
- RychlickiFZamponiNTrignaniRRicciutiRAIacoangeliMScerratiMVagus nerve stimulation: clinical experience in drug-resistant pediatric epileptic patientsSeizure200615648349016899378
- FrostMGatesJHelmersSLVagus nerve stimulation in children with refractory seizures associated with Lennox-Gastaut syndromeEpilepsia20014291148115211580762
- RossignolELortieAThomasTVagus nerve stimulation in pediatric epileptic syndromesSeizure2009181343718657451
- CukiertABurattiniJAMarianiPPExtended, one-stage callosal section for treatment of refractory secondarily generalized epilepsy in patients with Lennox-Gastaut and Lennox-like syndromesEpilepsia200647237137416499762
- YouSJLeeJKKoTSEpilepsy surgery in a patient with Lennox-Gastaut syndrome and cortical dysplasiaBrain Dev20072916717017005346
- HanksGWClobazam: pharmacological and therapeutic profileBr J Clin Pharmacol19797Suppl 1151S155S35198
- RissJCloydJGatesJCollinsSBenzodiazepines in epilepsy: pharmacology and pharmacokineticsActa Neurol Scand20081182698618384456
- BarzaghiFFournexRMantegazzaPPharmacological and toxicological properties of clobazam (1-phenyl-5-methyl-8-chloro-1,2,4,5-tetrahydro-2,4-diketo-3H-1,5-benzodiazepine), a new psychotherapeutic agentArzneimittelforschung19732356836864740211
- GastautHLowMDAntiepileptic properties of clobazam, a 1–5 benzodiazepine, in manEpilepsia1979204437446383476
- GiraudCTranAReyEVincentJTréluyerJMPonsGIn vitro characterization of clobazam metabolism by recombinant cytochrome P450 enzymes: importance of CYP2C19Drug Metab Dispos200432111279128615483195
- GiraudCTreluyerJMReyEIn vitro and in vivo inhibitory effect of stiripentol on clobazam metabolismDrug Metab Dispos200634460861116415114
- BertilssonLGeographical/interracial differences in polymorphic drug oxidation. Current state of knowledge of cytochrome P450 (CYP) 2D6 and 2C19Clin Pharmacokinet19952931922098521680
- ContinMSangiorgiSRivaRParmeggianiAAbaniFBaruzziAEvidence of polymorphic CYP2C19 involvement in the human metabolism of n-desmethylclobazamTher Drug Monit200224673774112451290
- KosakiKTamuraKSatoRSamejimaHTanigawaraYTakahashiTA major influence of CYP2C19 genotype on the steady-state concentration of N-desmethylclobazamBrain Dev200426853053415533655
- SeoTNagataRIshitsuTImpact of CYP2C19 polymorphisms on the efficacy of clobazam therapyPharmacogenomics20089552753718466100
- MeldrumBSChapmanAGHortonRWClobazam: anticonvulsant action in animal models of epilepsy [proceedings]Br J Clin Pharmacol19797Suppl 159S60S35206
- LöscherWRundfeldtCHönackDEbertULong-term studies on anticonvulsant tolerance and withdrawal characteristics of benzodiazepine receptor ligands in different seizure models in mice. I. Comparison of diazepam, clobazam and abercarnilJ Pharm Exp Ther19962792561572
- ŠlamberováRMarešPVorlíčekJClobazam exerts an anticonvulsant action in immature ratsPhysiol Res19984743013059803479
- MiuraYAmanoSToriiRIharaNClobazam shows a different antiepileptic action profile from clonazepam and zonisamide in Ihara epileptic ratsEpilepsy Res200249318920212076840
- LuszczkiJJTrojnarMKRatnarajNPatsalosPNCzuczwarSJInteractions of stiripentol with clobazam and valproate in the mouse maximal electroshock-induced seizure modelEpilepsy Res201090318819820493662
- NakamuraFSuzukiSNishimuraSYagiKSeinoMEffects of clobazam and its active metabolite on GABA-activated currents in rat cerebral neurons in cultureEpilepsia19963787287358764810
- GattaECupelloADi BraccioMNew 1,5-benzodiazepine compounds: activity at native GABA(A) receptorsNeuroscience2010166391792320096335
- QuilichiniPPChironCBen-AriYGozlanHStiripentol, a putative antiepileptic drug, enhances the duration of opening of GABA-A receptor channelsEpilepsia200647470471616650136
- WhitingPJBonnertTPMcKernanRMMolecular and functional diversity of the expanding GABA-A receptor gene familyAnn NY Acad Sci199986864565310414349
- GalanopoulouASGABA(A) receptors in normal development and seizures: friends or foes?Curr Neuropharmacol20086112019305785
- KorpiERGründerGLüddensHDrug interactions at GABA(A) receptorsProg Neurobiol200267211315912126658
- OgrisWPöltlAHauerBAffinity of various benzodiazepine site ligands in mice with a point mutation in the GABA receptor gamma2 subunitBiochem Pharmacol20046881621162915451405
- FisherJLInteractions between modulators of the GABA(A) receptor: Stiripentol and benzodiazepinesEur J Pharmacol2011654216016521237147
- KhomSBaburinITiminENHohausASieghartWHeringSPharmacological properties of GABAA receptors containing gamma1 subunitsMol Pharmacol200669264064916272224
- LiMSzaboARosenbergHCEvaluation of native GABA(A) receptors containing an alpha 5 subunitEur J Pharmacol20014131637211173064
- RudolphUCrestaniFMöhlerHGABA(A) receptor subtypes: dissecting their pharmacological functionsTrends Pharmacol Sci200122418819411282419
- RudolphUMöhlerHGABA-based therapeutic approaches: GABAA receptor subtype functionsCurr Opin Pharmacol200661182316376150
- RowlettJKPlattDMLelasSAtackJRDawsonGRDifferent GABAA receptor subtypes mediate the anxiolytic, abuse-related, and motor effects of benzodiazepine-like drugs in primatesProc Natl Acad Sci U S A2005102391592015644443
- DoiTUedaYTokumaruJWillmoreLJMolecular regulation of glutamate and GABA transporter proteins by clobazam during epileptogenesis in Fe(+++)-induced epileptic ratsBrain Res Mol Brain Res20051422919616274841
- UedaYDoiTTokumaruJCollapse of extracellular glutamate regulation during epileptogenesis: down-regulation and functional failure of glutamate transporter function in rats with chronic seizures induced by kainic acidJ Neurochem200176389290011158261
- MehndirattaMMKrishnamurthyMRajeshKNSinghGClobazam monotherapy in drug naïve adult patients with epilepsySeizure200312422622812763470
- HaighJRPullarTGentJPDailleyCFeelyMN-desmethylclobazam: a possible alternative to clobazam in the treatment of refractory epilepsy?Br J Clin Pharmacol19872322132183828198
- KinoshitaMIkedaABegumTTeradaKShibasakiHEfficacy of low-dose, add-on therapy of clobazam (CLB) is produced by its major metabolite, N-desmethyl-CLBJ Neurol Sci20072631–2444817588610
- WhitingPJGABA-A receptors: a viable target for novel anxiolytics?Curr Opin Pharmacol200661242916359919
- MunnRFarellKOpen study of clobazam in refractory epilepsyPediatr Neurol1993964654697605555
- Canadian Study Group for Childhood EpilepsyClobazam has equivalent efficacy to carbamazepine and phenytoin as monotherapy for childhood epilepsyEpilepsia19983999529599738674
- MillsJKLewisTGMughalKAliIUgurAWhitehouseWPRetention rate of clobazam, topiramate, and lamotrigine in children with intractable epilepsy at 1 yearSeizure201120540240521414810
- MontenegroMAArifHNahmEAResorSRJrHirschLJEfficacy of clobazam as add-on therapy for refractory epilepsy: experience at a US epilepsy centerClin Neuropharmacol200831633333819050410
- FarrellKBenzodiazepines in the treatment of children with epilepsyEpilepsia198627Suppl 1S45523743524
- JanMMShaabatAOClobazam for the treatment of intractable childhood epilepsySaudi Med J200021762262411500723
- SugaiKClobazam as a new antiepileptic drug and clorazepate dipotassium as an alternative antiepileptic drug in JapanEpilepsia200445Suppl 8S2025
- KalraVSethRMishraDSahaNCClobazam in refractory childhood epilepsyIndian J Pediatr201077326326620177827
- ShethRDRonenGMGouldenKJPenneySBodensteinerJBClobazam for intractable pediatric epilepsyJ Child Neurol19951032052087642889
- VadjaFJBladinPFParsonsBJClinical experience with clobazam: a new 1,5 benzodiazepine in the treatment of refractory epilepsyClin Exp Neurol1985211771823843217
- da SilveiraMRMentenegroMAFranzonRCGuerreiroCAGeurreiroMMEffectiveness of clobazam as add-on therapy in children with refractory focal epilepsyArq Neuropsiquiatr2006643B70571017057871
- SilvaRCMontenegroMAGeurreiroCAGeurreiroMMClobazam as add-on therapy in children with epileptic encephalopathyCan J Neurol Sci200633220921316736732
- KeeneDLWhitingSHumphreysPClobazam as an add-on drug in the treatment of refractory epilepsy of childhoodCan J Neurol Sci19901733173192207888
- ConryJANgYDrummondRStolleJSagarSEfficacy and safety of clobazam in the treatment of seizures associated with Lennox-Gastaut syndrome: results of a phase III trial [abstract]Proceedings of the 64th Annual Meeting of the American Epilepsy SocietyDecember 3–7, 2010San Antonio, Tx20101.283
- TrojnarMKWojtalKTrojnarMPCzuczwarSJStiripentol. A novel antiepileptic drugPharmacol Rep200557215416015886413
- ChironCDulacOThe pharmacological treatment of Dravet syndromeEpilepsia201152Suppl 2727521463285
- FisherJLThe effects of stiripentol on GABA(A) receptorsEpilepsia201152Suppl 2767821463286
- TheisJGKorenGDanemanRInteractions of clobazam with conventional antiepileptics in childrenJ Child Neurol19971232082139130097