

Abstract
Objective
To explore the timing of relapse following drug discontinuation and its relationship to estimated plasma levels and elimination half-life by comparing data from a randomized, placebo-controlled discontinuation study of cariprazine with those from similarly designed and conducted randomized control trials of other oral atypical antipsychotics (AAPs).
Methods
Data from a long-term, randomized, double-blind, placebo-controlled relapse prevention study in participants with schizophrenia (NCT01412060) were analyzed. Similarly designed, published studies of other AAPs were used for comparison. Time to drug-placebo relapse separation and relapse rates were estimated from Kaplan–Meier curves and evaluated descriptively. Separation was defined as a sustained difference of ≥5% incidence of relapse between the AAP and placebo curves.
Results
The Kaplan–Meier curve for cariprazine showed a time to drug-placebo relapse separation at 6–7 weeks after randomization, compared to the Kaplan–Meier curves for the other AAPs, which showed earlier separation at 1–4 weeks. The placebo relapse rates at 4 weeks after randomization were 5% for cariprazine and 8–34% for other AAPs. Geometric mean values of model-predicted plasma concentrations for total active cariprazine moieties (sum of cariprazine, desmethyl-cariprazine, and didesmethyl-cariprazine) were 20.0 and 6.1 nM at 2 and 4 weeks after discontinuation, respectively. Elimination half-lives of other AAPs and their active metabolites (<4 days) suggest that plasma concentrations would be low or negligible at 2–4 weeks after last dose.
Conclusion
Discontinuation of cariprazine treatment appeared to be associated with a delayed incidence of relapse compared with other AAPs, which may be due to the longer half-life of cariprazine and its active metabolites.
Supplementary materials
Table S1 List of independent ethics committee and institutional review boards
Table S2 Detailed stability criteria used in the relapse prevention studies
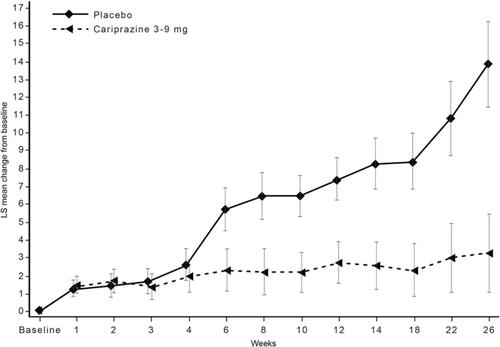
Figure S1 By-week change from baseline in PANSS total score (MMRM).
Abbreviations: LS, least squares; MMRM, mixed-effects model for repeated measures; PANSS, Positive and Negative Syndrome Scale.
References
- Durgam S, Earley W, Li R, et al. Long-term cariprazine treatment for the prevention of relapse in patients with schizophrenia: A randomized, double-blind, placebo-controlled trial. Schizophr Res. 2016;176(2–3):264–271. doi:10.1016/j.schres.2016.06.030
- Fleischhacker WW, Hobart M, Ouyang J, et al. Efficacy and safety of brexpiprazole (OPC-34712) as maintenance treatment in adults with schizophrenia: A randomized, double-blind, placebo-controlled study. Int J Neuropsychopharmacol. 2017;20(1):11–21. doi:10.1093/ijnp/pyw076
- Peuskens J, Trivedi J, Malyarov S, et al. Prevention of schizophrenia relapse with extended release quetiapine fumarate dosed once daily: A randomized, placebo-controlled trial in clinically stable patients. Psychiatry (Edgmont). 2007;4(11):34–50.
- Beasley CM, Jr., Sutton VK, Hamilton SH, et al. A double-blind, randomized, placebo-controlled trial of olanzapine in the prevention of psychotic relapse. J Clin Psychopharmacol. 2003;23(6):582–594. doi:10.1097/01.jcp.0000095348.32154.ec
- Tandon R, Cucchiaro J, Phillips D, et al. A double-blind, placebo-controlled, randomized withdrawal study of lurasidone for the maintenance of efficacy in patients with schizophrenia. J Psychopharmacol. 2016;30(1):69–77. doi:10.1177/0269881115620460
- Kane JM, Mackle M, Snow-Adami L, Zhao J, Szegedi A, Panagides J. A randomized placebo-controlled trial of asenapine for the prevention of relapse of schizophrenia after long-term treatment. J Clin Psychiatry. 2011;72(3):349–355. doi:10.4088/JCP.10m06306
- Weiden PJ, Manning R, Wolfgang CD, et al. A randomized trial of Iloperidone for prevention of relapse in schizophrenia: The REPRIEVE Study. CNS Drugs. 2016;30:735–747. doi:10.1007/s40263-016-0345-4
- Kramer M, Simpson G, Maciulis V, et al. Paliperidone extended-release tablets for prevention of symptom recurrence in patients with schizophrenia: a randomized, double-blind, placebo-controlled study. J Clin Psychopharmacol. 2007;27(1):6–14. doi:10.1097/JCP.0b013e31802dda4a
Availability of Data and Material
Allergan will share de-identified patient-level data and/or study-level data, including protocols and clinical study reports, for this clinical trial. To request access to the data, the researcher must sign a data use agreement. All shared data are to be used for non-commercial purposes only. More information can be found on http://www.allerganclinicaltrials.com/.
Acknowledgments
Writing and editorial assistance was provided by Katharine Fang, PhD, of Prescott Medical Communications Group (Chicago, IL), a contractor of Allergan. The authors thank Laishun Chen, PhD, for contributing to early discussions regarding plasma concentrations and EC50. A poster of the results in this manuscript was previously presented at the 171st Annual Meeting of the American Psychiatric Association, May 5-9, 2018, New York City, NY (abstract not published) and the 2019 Congress of the Schizophrenia International Research Society, April 10-14, 2019, Orlando, FL (this poster’s abstract was published in Schizophr Bull. 2019;45 Suppl 2:S317; https://academic.oup.com/schizophreniabulletin/article/45/Supplement_2/S317/5434430). Financial support for this work was provided by Allergan and Gedeon Richter Plc.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
Financial arrangements of the authors with companies whose products may be related to the present report are listed below, as declared by the authors. C. Correll has been a consultant and/or advisor to or has received honoraria from: Alkermes, Allergan, Angelini, Boehringer-Ingelheim, Gedeon Richter, Gerson Lehrman Group, Indivior, IntraCellular Therapies, Janssen/J&J, LB Pharma, Lundbeck, Medavante-ProPhase, Medscape, Merck, Neurocrine, Noven, Otsuka, Pfizer, Recordati, ROVI, Servier, Sumitomo Dainippon, Sunovion, Supernus, Takeda, and Teva. He has provided expert testimony for Bristol-Myers Squibb, Janssen, and Otsuka. He has served on a Data Safety Monitoring Board for Boehringer-Ingelheim, Lundbeck, ROVI, Supernus, and Teva. He has received royalties from UpToDate and grant support from Janssen and Takeda, and he is also a shareholder of LB Pharma. R. Jain has received grant funding from, or served as a consultant, on advisory boards or on speakers’ bureaus for Addrenex, Alkermes, Allergan, AstraZeneca, Avanir, Forum, Janssen, Lilly, Lundbeck, Merck, Neos Therapeutics, Neurocrine Biosciences, Otsuka, Pamlab, Pfizer, Rhodes, Supernus, Shionogi, Shire, Sunovion, Supernus, Takeda, Teva, and Tris Pharmaceuticals. J. Meyer has received speaking or advising fees from Acadia, Alkermes, Allergan, Arbor Scientia, Bristol-Myers Squibb, Merck, Neuroscience Education Institute, Neurocrine, Otsuka America, Sunovion, and Teva. A. Periclou, T. Carrothers, M. Patel, and W. Earley are employees of Allergan. Á. Barabássy is an employee of Gedeon Richter Plc. Allergan and Gedeon Richter Plc. The authors report no other conflicts of interest in this work.