Abstract
Background:
Generalized anxiety disorder (GAD) is often presented with major depression (MD). GAD-MD can be a chronic and disabling condition, and patients suffering from this disorder often respond poorly to psychopharmacological treatment and experience side effects with medication. Therefore, there is a high demand for effective nonpharmacological therapy for GAD-MD patients. The current study explores the use of a radioelectric asymmetric conveyer (REAC) device in the treatment of GAD-MD.
Methods:
Participants were 24 patients diagnosed with GAD-MD being treated at a public psychiatric center. All patients were dissatisfied with their current pharmacological treatment. Patients were evaluated using the 21-item Hamilton Depression (HAM-D) rating scale and the Symptom Check List-90-Revised (SCL-90R) before and after REAC brain stimulation treatment cycles.
Results:
After REAC brain stimulation treatment, all patients experienced a significant reduction in anxiety and depression. These results were confirmed by physician examination, HAM-D scores, and SCL-90R total scores.
Conclusion:
These results indicate a role for REAC brain stimulation in the management of psychiatric conditions, specifically, GAD-MD comorbidity. REAC treatments are synergistic to drug therapy and appear to be helpful in reducing the side effects of medication. Future studies should evaluate the long-term effects of REAC treatment.
Introduction
According to available epidemiological data, generalized anxiety disorderCitation1–Citation4 (GAD) is the most common anxiety disorderCitation5–Citation7 and one of the most common psychiatric conditions in the general population. The prevalence of GAD ranges from 4% to 8%. However, the actual figure for this condition is most likely double that number. Although GAD can be a chronic and disabling condition with a poor response to psychopharmacological treatment, it is one of the most unrecognized (both by the patient and the physician) and, consequently, undertreated mental pathologies.Citation1,Citation8,Citation9 Current therapies for GAD include serotonin and noradrenaline reuptake inhibitorsCitation10–Citation12 (eg, venlafaxine and duloxetine) and selective serotonin reuptake inhibitorsCitation12–Citation18 (eg, paroxetine and escitalopram), along with psychotherapeutic approaches,Citation19,Citation20 such as cognitive behavioral therapy.Citation21–Citation23 The delay in diagnosis, the chronic and continuous nature of the disorder, and importantly, inadequate response to current drug therapies may lead to demoralization, which often complicates GAD with major depression (MD). Unlike other psychiatric disorders, to date there are no known “physical” treatment options (eg, transcranial magnetic stimulation) for patients suffering from GAD comorbid with MD. While the majority of patients suffering from GAD-MD are treated by private psychiatrists,Citation24 the few who are seen in public psychiatric services are often seeking alternatives to traditional psychopharmacological treatment. The current study was conducted in a public psychiatry service outpatient setting with the goal of evaluating the efficacy of radioelectric asymmetric conveyer (REAC)Citation25,Citation26 brain stimulation in patients with comorbid GAD and MD. REAC treatments have proven efficacy in ameliorating motor behavior abnormalities,Citation27 stress-related disorders, depression, anxiety,Citation28–Citation33 and bipolar disorder.Citation34 In addition, REAC treatments are painless, noninvasive, and have no known adverse effects. The extensive use of “physical” approaches, such as REAC, as routine therapeutic protocols in the management of mental disorders, particularly those characterized by poor compliance and/or resistance to pharmacological treatment, is discussed.
Methods
The present study was approved by the Croce e Carle hospital ethics committee, Cuneo, Italy, and registered at the Australian New Zealand Clinical Trials Register. The study was conducted according to the principles of the Declaration of Helsinki.
Twenty-four outpatients (20 females and four males, mean age 46.7 ± 8.9 years) diagnosed with GAD-MD using current Diagnostic and Statistical Manual of Mental Disorders Fourth Revision criteria and the Symptom Checklist-90-Revised (SCL-90R)Citation35,Citation36 participated in the study. The patients were being treated at the Psychiatric Hospital of Cuneo, Italy. All patients were dissatisfied with the results of their ongoing medical treatment of serotonin and noradrenaline reuptake inhibitors or selective serotonin reuptake inhibitors at a standard dose and duration of treatment. All participants were maintained on their current pharmacological treatment. At baseline (T0), the average 21-item Hamilton Depression (HAM-D)Citation37 rating scale score was 15.5 ± 4.6, corresponding to a “mild” level of severity. The SCL-90R and HAM-D were administered prior to and after a standard cycle of REAC treatments (one Neuro Postural OptimizationCitation32 followed by 18 Neuro Psycho Physical OptimizationCitation32 sessions). Nine SCL-90R clusters were examined, ie, somatization, obsession-compulsion, interpersonal sensitivity, depression, anxiety, anger-hostility, phobic anxiety, paranoid ideation, and psychotic behavior. The SCL-90R was specifically used due to its greater sensitivity to critical clinical aspects of anxiety (ie, interpersonal sensitivity and phobic anxiety) than the classic Hamilton Anxiety Scale (HAM-A).Citation38 In addition, the overlap between HAM-D and HAM-A is well known.
REACCitation25,Citation26 was applied using a medical device based on an innovative biostimulation technology. REAC typically runs within a frequency range of 2.4, 5.8, or 10.5 gHz. For the current study, a frequency of 10.5 gHz, with a specific absorption rate of 7 μW/kg, was used. The REAC pulse protocol was seven radiofrequency bursts of 500 msec each, applied by touching the metallic tip of the REAC probe (Convogliatore di Radianza Modulante, Asmed, Italy) to the ear pavilion using Neuro Postural Optimization and Neuro Psycho Physical Optimization protocols which have been described in detail elsewhere.Citation31–Citation34 The time interval from the initial clinical assessment until the last Neuro Psycho Physical Optimization session was approximately one month. Data were analyzed with t-tests, Wilcoxon signed-rank tests and Sign-tests. Statistical significance was set at P < 0.05.
Results
REAC treatments were well tolerated, with a good safety profile, and there were no withdrawals from the study due to side effects. After REAC treatment, all patients showed a significant reduction in anxiety and depression symptomatology. In addition, the clinical picture of each patient, as measured by physician evaluation, was described either as “improved” or “very improved.” Moreover, clinical improvement was confirmed by psychometric test scores (– and ). The average HAM-D total score decreased from 15.5 ± 4.6 to 4.6 ± 2.2 (t = 10.472, df = 46, P < 0.001, see and ). These results indicate an improvement from “mild depression” to an “absence of depression.” Scores on all clusters of the SCL-90R scale were significantly decreased after REAC treatment. and show results for each specific symptomatic cluster on the SCL-90R scale, providing a more accurate picture of the quality of the clinical response.
Figure 1 Hamilton Depression rating scale scores (means ± standard deviation).
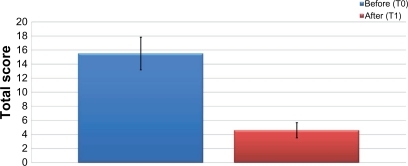
Figure 2 Hamilton Depression rating scale scores. Sum of the values of each cluster, before and after Neuro Psycho Physical Optimization treatment.
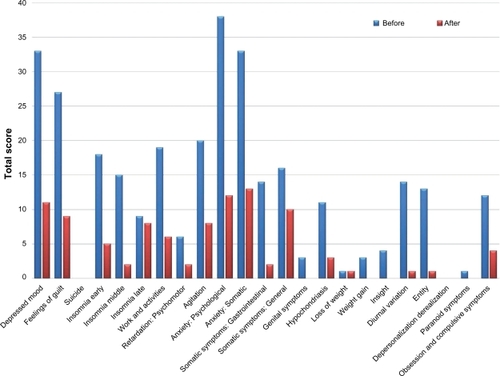
Figure 3 Hamilton Depression rating scale scores, mean of the value for each cluster, before and after Neuro Psycho Physical Optimization treatment.
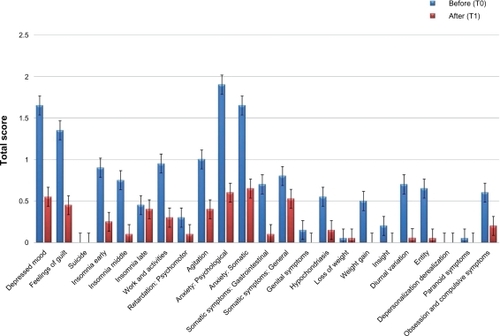
Figure 4 Mean value of each Symptom Check List-90-Revised cluster before and after Neuro Psycho Physical Optimization treatment.
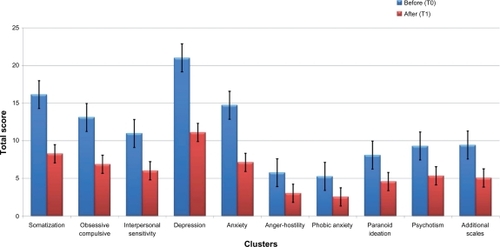
Table 1 Symptom Check List-90-Revised statistics for each cluster
Discussion
REAC treatment resulted in significant decreases in both anxiety and depressive symptomatology. The remission of depressive symptomatology was demonstrated by a significant decrease in average HAM-D total score. All patients, after approximately 1 month of REAC treatment scored <8 on the HAM-D. In clinical terms, 1 month is similar to the delay of action of all categories of antidepressant and antianxiety medication.Citation39 In addition, there was a notable response of all SCL-90R clusters to REAC treatment. The remission of psychiatric symptomatology was maximally affectedCitation27 in the majority of the clusters after Neuro Psycho Physical Optimization treatment. Moreover, the effect was observed in clusters that are typically refractory to the action of psychotropic drugs (ie, interpersonal sensitivity, somatization, and psychotic behavior). These results may be related to complex cortical dysregulationCitation40 which is not accessible to pharmacological action.
GAD-MD comorbidity often represents a psychopharmacological challenge, primarily due to a characteristic hypersensitivity to side effects coupled with the need for a high drug dosage. GAD-MD seems particularly sensitive to Neuro Psycho Physical Optimization treatments using REAC.Citation31–Citation33 In addition, REAC treatment appears to protect patients from jitteriness syndrome,Citation41,Citation42 which is frequently a cause of self-withdrawal from medication in GAD-MD patients.
REAC treatment appears to work synergistically with classic drug treatment, thereby optimizing clinical results.Citation34 Importantly, while all subjects continued medication during REAC treatment, many patients were able to reduce the dosage due to amelioration of their clinical condition. These results are particularly beneficial in patients who experience side effects from their medication.Citation34,Citation30 Therefore, the reduction in drug dosage needed as a result of REAC treatment, significantly increased the safety and tolerability profiles of serotonin and noradrenaline reuptake inhibitors and selective serotonin reuptake inhibitors.Citation43–Citation49
The mechanism of action of REAC treatment is mostly likely associated with remodulation of the abnormal brain activity seen in psychiatric disorders. This normalizing action appears to be crucial in anxiety disorders, where hyperfunctioning of newly developing, “reverberant,” and short intracortical pathways is well established, and is most likely related to fear and avoidance behaviors.Citation50–Citation52 Recent magnetic resonance imaging studies have confirmed these hypotheses.Citation34
Subjects in the current study showed a good response to REAC. The marked and rapid clinical efficacy, along with safety, tolerability, and ease of use, suggests more extensive use of REAC in public as well as private psychiatric settings, and the possibility of use in additional psychiatric disorders. The beneficial effects of REAC treatment in bipolar disorder have recently been demonstrated.Citation34
Amelioration of psychiatric symptoms using typical pharmacological treatments is elusive, and therefore, an innovative medical device such as REAC may serve as a beneficial adjunct. Moreover, REAC treatment sessions allow the physician to establish a close and more continuous relationship with patients. The doctor-patient relationship has been shown to be critical in promoting adherence to prescribed therapies.
While the current study was conducted exclusively in ambulatory patients, the advantages of REAC treatment may prove to be beneficial in the treatment of hospitalized patients. Further studies in a greater number of patients, using double-blind and placebo-controlled protocols, are needed. Long-term studies designed to evaluate the stability of REAC treatment are also required.
Acknowledgements
The authors would like to thank the medical staff at Struttura Complessa di Psichiatria, Cuneo, Italy, Matteo Lotti Margotti for data analysis, and Giorgio Saragò, Lucia Aravagli, and Stefania Bini of the Rinaldi Fontani Institute for their helpful advice.
Disclosure
Salvatore Rinaldi and Vania Fontani are the inventors of the radioelectric asymmetric conveyer system.
References
- BaldwinDSAjelKIGarnerMPharmacological treatment of generalized anxiety disorderCurr Top Behav Neurosci2010245346721309121
- MackenzieCSReynoldsKChouKLPaguraJSareenJPrevalence and correlates of generalized anxiety disorder in a national sample of older adultsAm J Geriatr Psychiatry20111930531521427639
- MichelsonSELeeJKOrsilloSMRoemerLThe role of values – consistent behavior in generalized anxiety disorderDepress Anxiety20112835836621308890
- NewmanMGLleraSJA novel theory of experiential avoidance in generalized anxiety disorder: a review and synthesis of research supporting a contrast avoidance model of worryClin Psychol Rev20113137138221334285
- BruceTJSaeedSASocial anxiety disorder: a common, underrecognized mental disorderAm Fam Physician19996023112010593322
- el-MiedanyYMel-RasheedAHIs anxiety a more common disorder than depression in rheumatoid arthritis?Joint Bone Spine20026930030612102277
- ZamorskiMAWardRKSocial anxiety disorder: common, disabling, and treatableJ Am Board Fam Pract20001325126010933289
- GoncalvesDCPachanaNAByrneGJPrevalence and correlates of generalized anxiety disorder among older adults in the Australian National Survey of Mental Health and Well-BeingJ Affect Disord201113222323021429587
- BlondeauJBouvetteAGeneralized anxiety disorder: recognizing it and understanding its impact on the cognitive functioningSante Ment Que201035221245 French.21076796
- CravelloLCaltagironeCSpallettaGThe SNRI venlafaxine improves emotional unawareness in patients with post-stroke depressionHum Psychopharmacol20092433133619330795
- SclarDARobisonLMSkaerTLConcomitant triptan and SSRI or SNRI use: a risk for serotonin syndromeHeadache20084812612918005139
- VlahiotisADevineSTEichholzJKautznerADiscontinuation rates and health care costs in adult patients starting generic versus brand SSRI or SNRI antidepressants in commercial health plansJ Manag Care Pharm20111712313221348545
- BitranSFarabaughAHAmeralVEDo early changes in the HAM-D-17 anxiety/somatization factor items affect the treatment outcome among depressed outpatients? Comparison of two controlled trials of St John’s wort (Hypericum perforatum) versus a SSRIInt Clin Psychopharmacol20112620621221278577
- HaliburnJAdolescent suicide and SSRI antidepressantsAustralas Psychiatry20101858721117851
- McCabeCMishorZFilippiniNCowenPJTaylorMJHarmerCJSSRI administration reduces resting state functional connectivity in dorso-medial prefrontal cortexMol Psychiatry20111659259421263442
- RucciPFrankEScoccoPTreatment-emergent suicidal ideation during 4 months of acute management of unipolar major depression with SSRI pharmacotherapy or interpersonal psychotherapy in a randomized clinical trialDepress Anxiety20112830330921308882
- SansoneRASansoneLASSRI-induced indifferencePsychiatry (Edgmont)201071418
- SilverHSusserEDanovichLSSRI augmentation of antipsychotic alters expression of GABA(A) receptor and related genes in PMC of schizophrenia patientsInt J Neuropsychopharmacol20111457358421208484
- GosselinPLadouceurRMorinCMDugasMJBaillargeonLBenzodiazepine discontinuation among adults with GAD: a randomized trial of cognitive-behavioral therapyJ Consult Clin Psychol20067490891917032095
- LadouceurRLegerEDugasMFreestonMHCognitive-behavioral treatment of generalized anxiety disorder (GAD) for older adultsInt Psychogeriatr20041619520715318764
- GaudianoBAReview: cognitive behavioural therapy is an effective treatment for depression, panic disorder, and generalised anxiety disorder, but may be less effective in severe casesEvid Based Ment Health200698016868199
- HabyMMDonnellyMCorryJVosTCognitive behavioural therapy for depression, panic disorder and generalized anxiety disorder: a meta-regression of factors that may predict outcomeAust N Z J Psychiatry20064091916403033
- ProudfootJRydenCEverittBClinical efficacy of computerised cognitive-behavioural therapy for anxiety and depression in primary care: randomised controlled trialBr J Psychiatry2004185465415231555
- DavidsonJRFeltnerDEDugarAManagement of generalized anxiety disorder in primary care: identifying the challenges and unmet needsPrim Care Companion J Clin Psychiatry2010122
- RinaldiSFontaniV inventors;RinaldiSFontaniV assignees.Radioelectric asymmetric conveyer for therapeutic use US patent EP1301241 (B1).10112006
- RinaldiSFontaniV inventors;RinaldiSFontaniV assignees.Radioelectric asymmetric conveyer for therapeutic use US patent 7,333,8592001.
- CastagnaARinaldiSFontaniVMannuPRadioelectric asymmetric brain stimulation and lingual apex repositioning in patients with atypical deglutition20114209213
- CastagnaARinaldiSFontaniVAravagliLMannuPMargottiMLDoes osteoarthritis of the knee also have a psychogenic component? Psycho-emotional treatment with a radio-electric device vs intra-articular injection of sodium hyaluronate: an open-label, naturalistic studyAcupunct Electrother Res20103511620578643
- CollodelGMorettiEFontaniVEffect of emotional stress on sperm qualityIndian J Med Res200812825426119052335
- MannuPRinaldiSFontaniVCastagnaALotti MargottiMRadio electric treatment vs es-citalopram in the treatment of panic disorders associated with major depression: an open-label, naturalistic studyAcupunct Electrother Res20093413514920344882
- RinaldiSFontaniVAravagliLMargottiMLPsychological and symptomatic stress-related disorders with radio-electric treatment: psychometric evaluationStress and Health2010265350358
- RinaldiSFontaniVAravagliLMannuPPsychometric evaluation of a radio electric auricular treatment for stress related disorders: a double-blinded, placebo-controlled controlled pilot studyHealth Qual Life Outcomes201083120302662
- RinaldiSFontaniVMorettiEA new approach on stress-related depression and anxiety: neuro-psycho-physical-optimization with radio electric asymmetric conveyerIndian J Med Res201013218919420716819
- MannuPRinaldiSFontaniVCastagnaALong-term treatment of bipolar disorder with a radioelectric asymmetric conveyorNeuropsychiatr Dis Treat2011737337921822388
- PedersenGKarterudSIs SCL-90R helpful for the clinician in assessing DSM-IV symptom disorders?Acta Psychiatr Scand200411021522415283742
- OlsenLRMortensenELBechPThe SCL-90 and SCL-90R versions validated by item response models in a Danish community sampleActa Psychiatr Scand200411022522915283743
- Serrano-DuenasMSoledad SerranoMConcurrent validation of the 21-item and 6-item Hamilton Depression Rating Scale versus the DSM-IV diagnostic criteria to assess depression in patients with Parkinson’s disease: an exploratory analysisParkinsonism Relat Disord20081423323817977055
- KadouriACorrubleEFalissardBThe improved Clinical Global Impression Scale (iCGI): development and validation in depressionBMC Psychiatry20077717284321
- TadicAWagnerSGorbulevSPeripheral blood and neuropsychological markers for the onset of action of antidepressant drugs in patients with major depressive disorderBMC Psychiatry2011111621269443
- CarverCSJohnsonSLJoormannJSerotonergic function, two-mode models of self-regulation, and vulnerability to depression: what depression has in common with impulsive aggressionPsychol Bull200813491294318954161
- BennettJAMoiofferMStantonSPDwightMKeckPEJrA risk-benefit assessment of pharmacological treatments for panic disorderDrug Saf1998184194309638387
- SinclairLIChristmasDMHoodSDAntidepressant-induced jitteriness/anxiety syndrome: systematic reviewBr J Psychiatry200919448349019478285
- ByrdLSerotonin syndrome: what is it? causes, recognition, and managementGeriatr Nurs20103138738920960693
- CosterSVisserMHTouwDJWirtzPWSerotonin syndrome with sertraline and indomethacinJ Clin Psychopharmacol20103046847020631569
- EvansRWTepperSJShapiroRESun-EdelsteinCTietjenGEThe FDA alert on serotonin syndrome with use of triptans combined with selective serotonin reuptake inhibitors or selective serotonin-norepinephrine reuptake inhibitors: American Headache Society position paperHeadache2010501089109920618823
- LawyerTIJensenJWeltonRSSerotonin syndrome in the deployed settingMil Med201017595095221265300
- PeacockLEWrightFSerotonin syndrome secondary to tramadol and citalopramAge Ageing20114052821414947
- RothrockJFTriptans, SSRIs/SNRIs and serotonin syndromeHeadache2010501101110220618824
- SanyalDChakrabortySBhattacharyyaRAn interesting case of serotonin syndrome precipitated by escitalopramIndian J Pharmacol20104241841921189920
- RockstrohBSWienbruchCRayWJElbertTAbnormal oscillatory brain dynamics in schizophrenia: a sign of deviant communication in neural networkBMC Psychiatry200774417760978
- RisslingAJMakeigSBraffDLLightGANeurophysiologic markers of abnormal brain activity in schizophreniaCurr Psychiatry Rep20101257257820857348
- KirbyEDFriedmanARCovarrubiasDBasolateral amygdala regulation of adult hippocampal neurogenesis and fear-related activation of newborn neuronsMol Psychiatry6142011 [Epub ahead of print.]