Abstract
Background
With a US Food and Drug Administration-labeled indication to treat attention-deficit/hyperactivity disorder (ADHD), the nonstimulant guanfacine has become the preferred α2-agonist for ADHD treatment. However, significant interindividual variability has been observed in response to guanfacine. Consequently, hypotheses of a contributing interaction with the ubiquitously expressed drug transporter, P-glycoprotein (P-gp), have arisen. We performed an in vitro study to determine if guanfacine is indeed a substrate of P-gp.
Methods
Intracellular accumulation of guanfacine was compared between P-gp expressing LLC-PK1/MDR1 cells and P-gp-negative LLC-PK1 cells to evaluate the potential interaction between P-gp and guanfacine. Cellular retention of guanfacine was analyzed using a high-performance liquid chromatographic-ultraviolet method. Rhodamine6G, a known P-gp substrate, was included in the study as a positive control.
Results
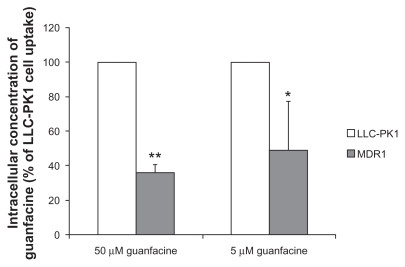
At guanfacine concentrations of 50 μM and 5 μM, intracellular accumulation of guanfacine in LLC-PK1/MDR1 cells was, 35.9% ± 4.8% and 49.0% ± 28.3% respectively, of that in LLC-PK1 cells. In comparison, the concentration of rhodamine6G, the positive P-gp substrate, in LLC-PK1/MDR1 cells was only 5% of that in LLC-PK1 cells.
Conclusion
The results of the intracellular accumulation study suggest that guanfacine is, at best, a weak P-gp substrate. Therefore, it is unlikely that P-gp, or any genetic variants thereof, are a determining factor in the interindividual variability of response observed with guanfacine therapy.
Introduction
Guanfacine, initially marketed as an antihypertensive agent, is a selective α2-adrenergic agonist believed to exert its antihypertensive activity by decreasing sympathetic tone in the central nervous system and reducing vascular resistance.Citation1 However, because of its preferential effects on α2A-adrenoreceptors, which are believed to play a role in attentional and organizational functions in the prefrontal cortex, guanfacine became a drug of interest in the treatment of attentiondef icit/hyperactivity disorder (ADHD).Citation2,Citation3 Although psychostimulants, such as methylphenidate and amphetamine, are considered first-line treatments for ADHD, they are discontinued in approximately 5% of patients due to lack of efficacy or unwanted side effects.Citation4 When psychostimulants are ineffective or only partially effective in reducing target symptoms, clinicians may opt to utilize nonstimulant medications, such as the α2-agonists clonidine and guanfacine, as either adjunctive treatments or monotherapy. Because of its greater selectivity for the α2A-adrenoreceptor, a longer half-life, a potentially decreased side effect burden, and a US Food and Drug Administration-labeled indication to treat ADHD as monotherapy or as an adjunct to stimulant medications, guanfacine has become the preferred α2-agonist for use in ADHD.Citation5 Additionally, a number of published studies have demonstrated the efficacy of guanfacine in reducing target symptoms of ADHD in children and adolescents.Citation5–Citation7
As is the case with the more traditional psychostimulants, methylphenidate and amphetamine, significant interindividual variability in response to guanfacine has been reported. For example, in a prospective trial of guanfacine in children with comorbid pervasive developmental disorder and ADHD, the improvement from baseline ADHD symptom scores ranged widely (ie, −1 to 41 points).Citation8 Similarly, in a large retrospective chart review of children with pervasive developmental disorders receiving guanfacine, the rate of positive response ranged from 13% to 39%, depending on the patient population assessed.Citation9 A trend indicating clear superiority of guanfacine over placebo, albeit with significant interindividual variability in endpoint ratings of ADHD symptoms, is a consistent finding in the published literature.Citation6,Citation10
Interindividual variation in drug response and disposition may be attributed to varied drug transporter activity, which is mediated by an array of single nucleotide polymorphisms (SNPs), as well as other endogenous and exogenous substances that may serve as transporter inhibitors or inducers.Citation11,Citation12 P-glycoprotein (P-gp) is the most thoroughly studied member of the adenosine triphosphate-binding cassette transporter superfamily, and is expressed throughout the body in the intestinal epithelium, hepatocytes, renal tubular cells, adrenal gland, blood–brain barrier, blood–testis barrier, and blood–placenta barrier.Citation13 In humans, P-gp is encoded by the ABCB1/MDR1 gene.Citation14,Citation15 Because of its ubiquitous expression and broad specificity, changes in P-gp expression or efflux activity induced by drug treatments, diet, environmental factors, or SNPs can greatly impact drug disposition, pharmacokinetics, and clinical response.Citation16,Citation17 Hence, identification of P-gp substrates is important for therapeutic optimization and the avoidance of drug–drug interactions.
Several published studies have investigated the potential interaction between guanfacine and P-gp. Mahar Doan et al conducted an in vitro study to determine whether guanfacine is a substrate of P-gp utilizing a Transwell cell culture model with P-gp-expressing Madin Darby canine kidney cells. The ratio of the transport velocity of guanfacine in the direction of basolateral-to-apical to apical-to-basolateral was found to be 1.2, indicating that guanfacine is not a P-gp substrate.Citation18 Similarly, based upon a computational method (topological substructural molecular design approach), other investigators predicted that guanfacine would be unlikely to serve as a P-gp substrate.Citation19
Although these data suggest that guanfacine is not a P-gp substrate, a recently published clinical study examined the potential influence of the known SNPs variant of P-gp, C3435T, on response to guanfacine treatment in children diagnosed with ADHD. The authors concluded that patients genotyped and found to carry the C3435T variant showed significantly less clinical improvement in ADHD symptoms relative to patients who were wild-type for the gene.Citation20 The C3435T variant has previously been shown to influence both gene expression and substrate specificity of P-gp.Citation17,Citation21 Thus, the association between therapeutic response and the C3435T SNPs suggests that P-gp plays a role in the transport of guanfacine. Therefore, the purpose of this study was to use a different cell line (human P-gp-overexpressing porcine kidney epithelial cell line LLC-PK1/MDR1) and a different in vitro model (intracellular uptake) relative to that previously published to determine if guanfacine is indeed a P-gp substrate.
Materials and methods
Materials
The porcine kidney epithelial cell line LLC-PK1 and human P-gp-overexpressing mutant LLC-PK1/MDR1 cells were kindly provided by Dr Kari Kivistö (Dr Margarete Fischer-Bosch Institute of Clinical Pharmacology, Stuttgart, Germany). Fetal bovine serum, trypsin, and Dulbecco’s Modified Eagle Medium containing 4500 mg/L glucose, 4 mM l-glutamine, and sodium pyruvate were obtained from Hyclone Co (Logan, UT). Dulbecco’s phosphate- buffered saline, penicillin, and streptomycin were purchased from Mediatech Inc (Herndon, VA). Guanfacine and rhodamine6G were obtained from Sigma Co (St Louis, MO). The Pierce bicinchoninic acid protein assay kit (Thermo Scientific, Rockford, IL) was used to determine protein concentrations. All other agents were of high analytical grade and commercially available.
Cell cultures and intracellular uptake studies
LLC-PK1 and LLC-PK1/MDR1 cells were cultured at 37°C in Dulbecco’s Modified Eagle Medium supplemented with 10% fetal bovine serum, 1% penicillin, and streptomycin in an atmosphere of 5% CO2 and 95% relative humidity. Cells (1 mL) were seeded into 24-well plates at a density of 1 × 105 cells/mL. Culture medium was replaced every two days until cells reached confluence. To investigate the potential influence of P-gp on guanfacine transport, intracellular accumulation of guanfacine was measured in LLC-PK1/MDR1 cells and P-gp-negative LLC-PK1 cells. Rhodamine6G, a well-known P-gp substrate, was included as a positive control. After cells reached confluence, the culture medium was replaced by transport buffer (serum-free Dulbecco’s Modified Eagle Medium) for a 30-minute preincubation at 37°C. Transport buffer was then removed and the test compounds (5 μM rhodamine6G, 5 μM guanfacine, or 50 μM guanfacine) were added, and an additional 60-minute incubation period commenced. Next, the solutions were discarded, and the cells were washed three times with ice-cold Dulbecco’s phosphate-buffered saline and solubilized with 1% Triton X-100. Intracellular accumulation of rhodamine6G was measured using a fluorescent microplate reader with a 530 nm excitation and a 580 nm emission wavelength, which is a well established method.Citation22 Cellular retention of guanfacine was analyzed by the high-performance liquid chromatographic assay described below. The concentrations of rhodamine6G and guanfacine were calculated from their respective standard curves, and standardized with the cellular protein content determined by a Pierce bicinchoninic acid protein kit.
High-performance liquid chromatographic analysis
A novel high-performance liquid chromatographic-ultraviolet detection method for guanfacine quantification was developed for this study. Briefly, 100 μL of acetonitrile containing the internal standard, p-nitrophenol 100 μM, was added to a 100 μL sample and vortexed. Samples were centrifuged at 13,200 rpm at 4°C for 30 minutes to remove proteins. The supernatant (50 μL) was injected into the high-performance liquid chromatography column for analysis. Separation was performed on a reverse-phase column (Luna 5μ C8, 250 × 4.6 mm) at 40°C. The mobile phase consisted of 25% acetonitrile and 75% KH2PO4 (10 mM, pH 4), and the flow rate was 1.0 mL/min. Guanfacine was detected by ultraviolet absorption at 220 nm.
Data analysis
All data are presented as means ± standard deviation. Intracellular concentrations of rhodamine6G and guanfacine in LLC-PK1/MDR1 cells are expressed as the percentages of that in LLC-PK1 cells. A two-tailed unpaired Student’s t-test was used for data analyses, with a P value of ≤0.5 considered statistically significant.
Results
The P-gp substrate properties of guanfacine were assessed by measuring intracellular drug accumulations in LLCPK1 and LLC-PK1/MDR1 cells. The results shown in indicate that, at a guanfacine concentration of 50 μM, the intracellular concentration of guanfacine was three-fold higher in LLC-PK1 cells than in LLC-PK1/MDR1 cells (35.9% ± 4.8% of LLC-PK1 cell uptake, P < 0.01). Similarly, at a guanfacine concentration of 5 μM, the intracellular concentration of guanfacine was two-fold higher in LLC-PK1 cells than in LLC-PK1/MDR1 cells (49.0% ± 28.3%, P < 0.05). By comparison, the concentration of the positive P-gp control substrate, rhodamine6G, in LLC-PK1/MDR1 cells was only 5% of that in LLCPK1 cells. Overall, these results suggest that guanfacine is, at best, a weak substrate for P-gp.
Figure 1 Intracellular concentrations of guanfacine in LLC-PK1 and LLC-PK1/MDR1 cells. Each column represents the mean percentages of intracellular guanfacine concentrations relative to that in LLC-PK1 cells, with a bar representing the standard deviation of three independent measurements.
Discussion
An estimated 100,000 patients die each year of adverse drug reactions in the US, thus making adverse drug reactions one of the leading causes of death in hospitalized patients.Citation23 Some of these deaths are caused by drug–drug interactions. Most drug interactions occur as an unexpected result of changes in pharmacokinetics due to drug coadministration. Combined pharmacotherapy in child, adolescent, and adult psychiatric patients has recently become a growing practice.Citation24–Citation26 Because ADHD therapeutic agents are the most commonly used psychotropic drugs in children and adolescents and are often used in combination with other therapeutic agents on an acute or chronic basis, the potential for drug–drug interactions, at least in theory, is extremely high.Citation27–Citation29
Interaction of psychotropic drugs with P-gp has been well documented in recent years. For example, Uhr et al demonstrated that a series of antidepressant medications, including venlafaxine and paroxetine, are substrates for P-gp.Citation30 Additionally, Wang et al reported that the antipsychotic risperidone and its active metabolite, 9-hydroxy-risperidone, are both P-gp substrates.Citation31 Other psychotropic agents that have been documented as substrates of P-gp to some degree include (R)-methadone, (S)-methadone, olanzapine, d-modafinil, l-modafinil, and d-methylphenidate.Citation29,Citation32,Citation33 Because P-gp is the most important efflux transporter at the blood–brain barrier, entry of these substrates into the central nervous system is greatly limited. Furthermore, a number of psychotropic drugs have been found to be P-gp inhibitors, which may affect disposition of coadministered P-gp substrates.Citation29,Citation34,Citation35
Prominent variability of response has been reported in patients taking guanfacine to treat ADHD.Citation6,Citation8–Citation10 In a recent study, variation in response to guanfacine correlated to a single nucleotide polymorphism of the MDR1 gene, the gene encoding for human P-gp.Citation20 The present study was therefore performed to determine if guanfacine, like many other psychotropic drugs, is a P-gp substrate.
The results of the intracellular accumulation study of guanfacine in P-gp-expressing cells suggest that guanfacine is, at best, a weak P-gp substrate. Specifically, the accumulation of guanfacine in LLC-PK1/MDR1 cells was approximately 30%–50% of that in LLC-PK1 cells under our experimental conditions. In comparison, the intracellular concentration of the established P-gp substrate rhodamine6G in LLC-PK1/MDR1 cells was only 5% of that in control cells. Thus, it appears the role of P-gp in guanfacine transport is minor, and P-gp is unlikely to be one of the determinants of the interindividual variability in response to guanfacine therapy. Thus, the reported effect of the MDR1 SNP C3435T on the response to guanfacine treatment must be interpreted carefully and warrants further investigation.
Acknowledgment
We would like to acknowledge the University of Florida Department of Pharmacotherapy and Translational Research Summer Research Training Program for providing support to perform this research.
Disclosure
The authors report no conflicts of interest in this work.
References
- SorkinEMHeelRCGuanfacine: A review of its pharmacodynamic and pharmacokinetic properties, and therapeutic efficacy in the treatment of hypertensionDrugs19863143013363519177
- ArnstenAFCaiJXGoldman-RakicPSThe alpha-2 adrenergic agonist guanfacine improves memory in aged monkeys without sedative or hypotensive side effects: Evidence for alpha-2 receptor subtypesJ Neurosci1988811428742982903226
- AveryRFranowiczJCSStudholmeCvan DyckCHArnstenAFTThe alpha-2A-adrenoceptor agonist, guanfacine, increases regional cerebral blood flow in dorsolateral prefrontal cortex and improves accuracy in monkeys performing a spatial working memory taskNeuropsychopharmacology200023324024910942848
- CrenshawTMKavaleKAFornessSRReeveREAttention deficit hyperactivity disorder and the efficacy of stimulant medication: A meta-analysisScruggsTEMastropieriMAAdvances in Learning and Behavioral DisabilitiesGreenwich, CTJAI Press1999
- BiedermanJMelmedRDPatelAfor SPD503 Study GroupA randomized, double-blind, placebo-controlled study of guanfacine extended release in children and adolescents with attention-deficit/hyperactivity disorderPediatrics20081211e73e8418166547
- NewcornJHSchulzKPHalperinJMAdrenergic agonists: Clonidine and guanfacineMartinAScahillLCharneyDSLeckmanJFPediatric Psychopharmacology: Principles and PracticeNew York, NYOxford2003
- ScahillLChappelPBKimYSA placebo-controlled study of guanfacine in the treatment of children with tic disorders and attention deficit hyperactivity disorderAm J Psychiatry200115871067107411431228
- ScahillLAmanMGMcDougleCJA prospective open trial of guanfacine in children with pervasive developmental disordersJ Child Adolesc Psychopharmacol200616558959817069547
- PoseyDJPuntneyJISasherTMKemDLMcDougleCJGuanfacine treatment of hyperactivity and inattention in pervasive developmental disorders: A retrospective analysis of 80 casesJ Child Adolesc Psychopharmacol200414223324115319020
- CummingsDDSingerHSKriegerMMillerTLMahoneEMNeuropsychiatric effects of guanfacine in children with mild Tourette syndrome: A pilot studyClin Neuropharmacol200225632533212469007
- BeringerPMSlaughterRLTransporters and their impact on drug dispositionAnn Pharmacother20053961097110815886292
- BoschTMMeijermanIBeijnenJHSchellensJHGenetic polymorphisms of drug-metabolising enzymes and drug transporters in the chemotherapeutic treatment of cancerClin Pharmacokinet200645325328516509759
- ThiebautFTsuruoTHamadaHGottesmanMMPastanIWillinghamMCCellular localization of the multidrug-resistance gene product P-glycoprotein in normal human tissuesProc Natl Acad Sci U S A19878421773577382444983
- SchuetzEGBeckWTSchuetzJDModulators and substrates of P-glycoprotein and cytochrome P4503A coordinately up-regulate these proteins in human colon carcinoma cellsMol Pharmacol19964923113188632764
- WacherVJWuCYBenetLZOverlapping substrate specificities and tissue distribution of cytochrome P4503A and P-glycoprotein: Implications for drug delivery and activity in cancer chemotherapyMol Carcinog20001331291347619215
- HitzlMDrescherSvan der KuipHThe C3435T mutation in the human MDR1 gene is associated with altered efflux of the P-glycoprotein substrate rhodamine 123 from CD56+ natural killer cellsPharmacogenetics200111429329811434506
- HoffmeyerSBurkOvon RichterOFunctional polymorphisms of the human multidrug-resistance gene: Multiple sequence variations and correlation of one allele with P-glycoprotein expression and activity in vivoProc Natl Acad Sci U S A20009773473347810716719
- Mahar DoanKMHumphreysJEWebsterLOPassive permeability and P-glycoprotein-mediated efflux differentiate central nervous system (CNS) and non-CNS marketed drugsJ Pharmacol Exp Ther200230331029101712438524
- CabreraMAGonzálezIFernándezCNavarroCBermejoMA topological substructural approach for the prediction of P-glycoprotein substratesJ Pharm Sci200695358960616432877
- McCrackenJTAmanMGMcDougleCJPossible influence of variant of the P-glycoprotein gene (MDR1/ABCB1) on clinical response to guanfacine in children with pervasive developmental disorders and hyperactivityJ Child Adolesc Psychopharmacol20102011520166790
- Kimchi-SarfatyCOhJMKimI-WA “silent” polymorphism in the MDR1 gene changes substrate specificityScience2007315581152552817185560
- SarverJGKlisWAByersJPErhardtPWMicroplate screening of the differential effects of test agents on Hoechst 33342, rhodamine 123, and rhodamine 6G accumulation in breast cancer cells that overexpress P-glycoproteinJ Biomol Screen200271293411897053
- LazarouJPomeranzBHCoreyPNIncidence of adverse drug reactions in hospitalized patients: A meta-analysis of prospective studiesJAMA199827915120012059555760
- ConnorDFOzbayrakKRKusiakKACaponiABMelloniRHJrCombined pharmacotherapy in children and adolescents in a residential treatment centerJ Am Acad Child Adolesc Psychiatry19973622482549031578
- SaferDJZitoJMDosReisSConcomitant psychotropic medication for youthsAm J Psychiatry2003160343844912611822
- WilensTESpencerTBiedermanJWozniakJConnorDCombined pharmacotherapy: An emerging trend in pediatric psychopharmacologyJ Am Acad Child Adolesc Psychiatry19953411101127860450
- GreenhillLLHalperinJMAbikoffHStimulant medicationsJ Am Acad Child Adolesc Psychiatry199938350351210230181
- SpencerTBiedermanJWilensTAttention-deficit/hyperactivity disorder and comorbidityPediatr Clin North Am199946591592710570696
- ZhuH-JWangJ-SDonovanJLInteractions of attention-deficit/hyperactivity disorder therapeutic agents with the efflux transporter P-glycoproteinEur J Pharm Sci20085782–3148158
- UhrMGrauerMTHolsboerFDifferential enhancement of antidepressant penetration into the brain in mice with abcb1ab (mdr1ab) P-glycoprotein gene disruptionBiol Psychiatry200354884084614550684
- WangJ-SRuanYTaylorRMDonovanJLMarkowitzJSDeVaneCLThe brain entry of risperidone and 9-hydroxyrisperidone is greatly limited by P-glycoproteinJ Neuropsychopharmacology200474415419
- WangJ-SRuanYTaylorRMDonovanJLMarkowitzJSDeVaneCLBrain penetration of methadone (R)- and (S)-enantiomers is greatly increased by P-glycoprotein deficiency in the blood-brain barrier of abcb1a gene knockout micePsychopharmacology20041731–213213814712343
- WangJ-STaylorRRuanYDonovanJLMarkowitzJSDeVaneCLOlanzapine penetration into brain is greater in transgenic abcb1a P-glycoprotein-deficient mice than FVB1 (wild-type) animalsJ Neuropsychopharmacology2004293551557
- WangJ-SZhuH-JMarkowitzJSDonovanJLDeVaneCLEvaluation of antipsychotic drugs as inhibitors of multidrug resistance transporter P-glycoproteinPsychopharmacology2006187441542316810505
- ZhuH-JWangJ-SMarkowitzJSDonovanJLGibsonBBDeVaneCLRisperidone and paliperidone inhibit P-glycoprotein activity in vitroNeuropsychopharmacology200732475776416936711