
Abstract
Purpose
Schizophrenia is a severe, chronic condition accounting for disproportionate healthcare utilization. Antipsychotics can reduce relapse rates, but the characteristics of schizophrenia may hinder medication adherence. A phase 3b open-label clinical trial used aripiprazole tablets with sensor (AS; includes pills with ingestible event-marker, wearable sensor patches and smartphone application) in adults with schizophrenia. This post hoc analysis explored how healthcare providers’ (HCPs) usage of a dashboard that provided medication ingestion information impacted treatment decisions and clinical assessments.
Patients and Methods
Participants used AS for 3–6 months. HCPs were instructed to check the dashboard regularly, identify features used, and report impact on treatment decisions. After stratifying HCPs by frequency of dashboard checks and resulting treatment decisions, changes from baseline were calculated for Positive and Negative Syndrome Scale (PANSS), Clinical Global Impression (CGI)–Severity of Illness and CGI-Improvement (CGI-I), and Personal and Social Performance (PSP), and compared using Mann–Whitney U-tests and rank-biserial correlation coefficient (r) effect sizes.
Results
To ensure sufficient opportunity for AS engagement, 113 participants who completed ≥3 months on study were analyzed. HCPs most often accessed dashboard data regarding medication ingestion and missed doses. HCPs recommended adherence counseling and participant education most often. Participants whose HCPs used the dashboard more and recommended adherence counseling and participant education (n=61) improved significantly more than participants with less dashboard-active HCPs (n=49) in CGI-I mean score (2.9 versus 3.4 [p=0.004]), total PANSS (mean change: −9.2 versus −3.1 [p=0.0002]), PANSS positive subscale (−3.2 versus −1.5 [p=0.003]), PANSS general subscale (−4.3 versus −1.2 [p=0.02]), and Marder factor for negative symptoms (−1.9 versus 0.0 [p=0.03]). Most HCPs found the dashboard easy to use (74%) and helpful for improving conversations with participants about their treatment plan and progress (78%).
Conclusion
This provider dashboard may facilitate discussions with patients about regular medication-taking, which can improve patient outcomes.
Plain Language Summary
Patients with schizophrenia often do not take their medication regularly. If a patient’s prescribed medication is not helping their symptoms, it can be hard for doctors to know why. Is the medication not working or is it not being taken correctly? Technology may help answer this question.
In this study, participants chose to take tablets of aripiprazole (an antipsychotic used to treat schizophrenia) containing a sensor that sends a signal when the pill has been taken. The signal was picked up by a patch on the participant’s skin, which sent this information to a smartphone app (for participants) and an online dashboard (for doctors). Doctors used this information to see if study participants were taking their medication regularly.
This study used surveys completed by doctors to answer the following question: Did the dashboard provide useful information that helped doctors determine the best treatment plan for study participants? Participants were divided into 2 groups: those whose doctors used the dashboard often and adjusted treatment and those whose doctors did not use the dashboard this way.
When doctors used the dashboard frequently and recommended that study participants get counseling on taking their medication or other education, participants’ schizophrenia symptoms improved more than participants whose doctors checked the dashboard less frequently or who did not make the same treatment suggestions.
Information from the dashboard helped doctors talk to study participants with schizophrenia about their illness and helped doctors decide the best treatment plan.
Introduction
The global prevalence of schizophrenia has been increasing, from 13.1 million in 1990 to nearly 21 million in 2016.Citation1 In the United States (US), 0.3–1.6% of the population is diagnosed with schizophrenia,Citation2–4 depending on the criteria used.Citation5 Yet despite the relatively low rate of occurrence, care of patients with schizophrenia accounts for 2.5% of total annual healthcare costs, due to greater use of inpatient treatment and more frequent emergency department visits in nonadherent patientsCitation2 and a higher inpatient admission rate for patients with schizophrenia.Citation6 A recent meta-analysis of 34 studies found the standardized mortality rate of people with schizophrenia to be 3.08 (95% confidence interval [CI], 2.88–3.31),Citation7 with the increased mortality impacted by heightened risk of suicide and medical comorbidities.Citation3,Citation8
While antipsychotics are the foundation of treatment for patients with schizophrenia,Citation9 many patients have a suboptimal response to these treatments,Citation10 particularly patients experiencing primary negative symptoms.Citation11 Achieving optimal pharmacotherapy for patients with schizophrenia is difficultCitation12 and is further complicated by medication nonadherence,Citation13,Citation14 which is a common challenge in this patient population.Citation15 In a 2020 meta-analysis of 9 studies, 56% of 2643 patients with schizophrenia were nonadherent to their medications.Citation16 Side effects of medication, disease characteristics (eg, impaired cognition, symptoms such as delusions or depression), negative patient attitudes, lack of insight, perceived stigma, and low-quality relationships with healthcare providers (HCPs) or therapists can contribute to nonadherence.Citation13,Citation16,Citation17 Nonadherence to antipsychotics is linked to symptom relapse, poorer quality of life, increased healthcare expenditures, resistance to subsequent treatment, greater use of emergency services, and psychiatric rehospitalization.Citation13,Citation16,Citation18,Citation19 In a study of 63 patients who discontinued their antipsychotic medication following first-episode psychosis, 57% relapsed within 12 months, with a median time to relapse of 8 months.Citation20 Of the patients who relapsed, 52.8% were admitted to the hospital.Citation20 Therefore, once patients with schizophrenia are discharged from the hospital, their need for continued care remains high.Citation21
Patients with schizophrenia need continuous integrated healthcare to prevent relapse and early mortality.Citation22 Conceptually, continuity of care is defined as a trust-based longitudinal relationship in which a patient’s HCP or care team maintains contact to monitor the patient’s progress, improve communication, and enable shared decision-making.Citation23–25 Continuity of care is associated with lower healthcare costs, reduced acute treatment events,Citation22 fewer hospital admissions,Citation26 and reduced risk of death.Citation27 In a US nationwide survey, patients with schizophrenia or schizoaffective disorder who had >1 change to their key HCP or psychiatrist in the past 12 months were less likely to be satisfied with their treatment, feel that they had been helped by services, or know how to access help in times of crisis, compared with patients who did not experience changes.Citation28 Among participants with serious mental illness (SMI), lack of continuity with providers was cited by both participants and their providers as a reason underlying participants’ decision to disengage from treatment and services.Citation29
However, achieving continuity of care in patients with schizophrenia and other SMIs is difficult. There is a national shortage of mental health providers, with a median of 1 provider per 380 individuals across the US.Citation30 Patients often have trouble accessing a provider; a survey conducted by the National Council on Behavioral Health found that 38% of the patients had to wait ≥1 week for an appointment with a mental health provider.Citation31 Once patients are able to schedule a visit with their provider, the process of actually getting mental healthcare is impaired by travel time to reach the appointment, costs, short visit lengths, lack of communication between the patient and provider, and insufficient access to relevant information for the patient and provider.Citation31–33 Individuals generally overestimate their medication adherence when they self-report, due to the impact of recall or reporting bias;Citation34 in patients with schizophrenia, accurate self-reporting of when they take their medication can be further challenged by active psychotic symptoms or lack of insight.Citation35,Citation36
Digital technologies can help deliver healthcare and advance research in patients with SMIs, including schizophrenia.Citation37,Citation38 Moreover, digital technologies may improve continuity of care by enabling providers to stay in contact with their patients.Citation39 Among those self-identifying as having schizophrenia, schizoaffective disorder, or a schizophrenia spectrum disorder, 90% reported having access to >1 personal computer, public computer, phone (smartphone, mobile, or landline), and tablet; 36% reported using web-based technology often or very often to cope with their schizophrenia.Citation40 For HCPs caring for patients with SMI, technology-assisted care tools can aid clinical supervision, extend HCP availability, increase the accuracy of some health information (eg, medication ingestion), tailor services to individual patients, and direct focus to patients most in need of intensive services.Citation41,Citation42 Digital technologies may help providers address challenges with medication adherence, such as using objective ingestion data to determine adherenceCitation35,Citation43 or informing and potentially adjusting medication regimens in treatment-nonresponsive patients.Citation35,Citation44 For example, a 2021 study of a digital antipsychotic medication reported 63.4% of study days with good sensor patch coverage, detected 56.4% of ingestible event-markers, generated an adherence metric of 86.6%, and was considered satisfactory and helpful by a majority of patients with SMI.Citation45
A recent, phase 3b, mirror-image, open-label, single-arm clinical trial compared outcomes for patients with schizophrenia who had a history of psychiatric hospitalization when they used standard-of-care (SOC) oral antipsychotics versus when they used ABILIFY MYCITE® (aripiprazole tablets with sensor [AS]).Citation46 AS consists of aripiprazole tablets embedded with an ingestible event-marker sensor, wearable sensor patches and a smartphone application, and is indicated for the treatment of adults with schizophrenia or bipolar I disorder, and as adjunct treatment for adults with major depressive disorder.Citation47 In the AS system, clinicians can review patient medication ingestion data via a web-based dashboard, and patients can access their data via the smartphone application.Citation47 In the primary analysis of this mirror-image study, comparison of discordant pairs revealed that after participants with schizophrenia initiated AS in the prospective period, no participants were hospitalized who had not been previously hospitalized in the retrospective period when they took SOC oral antipsychotics, whereas significantly more participants were hospitalized while taking SOC in the retrospective period and were not rehospitalized after initiating AS (9.7% of participants at 3-month comparison and 19.8% at 6-month comparison).Citation46 While digital tools seem poised to improve some aspects of patient–provider relationships, little is known about how clinicians engage with these tools or how these providers apply the information provided.
The aim of this post hoc analysis was to explore how HCPs’ dashboard usage impacted treatment decisions and clinical outcome assessments in participants with schizophrenia. To understand whether participants whose HCPs used the dashboard frequently had improved outcomes compared with participants whose HCPs accessed the dashboard less often, we evaluated the frequency with which HCPs accessed AS dashboards, features used most often, and resulting treatment recommendations, and how these usage patterns impacted longitudinal clinical assessments.
Materials and Methods
Study Design
This was a post hoc analysis of clinical data prospectively collected from a phase 3b mirror-image, open-label trial evaluating AS (NCT03892889). The full study methods have been previously described.Citation46 Briefly, eligible adults were aged 18–65 years, had been diagnosed with schizophrenia per the Diagnostic and Statistical Manual of Mental Disorders, fifth edition, had a Positive and Negative Syndrome Scale (PANSS) scoreCitation48 between 60 and 90, and had ≥1 inpatient psychiatric hospitalization(s) in the past 4 years. Participants had been prescribed oral SOC antipsychotics for at least the previous 6 months and then were switched to AS for at least 3 months and up to 6 months based on investigator feedback and participant preference. After participants switched to AS, HCPs were instructed to check the dashboard at least every 2 weeks and to complete a dashboard review survey each time they used the dashboard to identify which dashboard features they had used and how these impacted their resulting treatment decisions for participants.
Definition of HCP Groups for Comparison
“High dashboard use” providers (HDUPs) were defined as those who checked the dashboard at least every 3 weeks and, if their patient recorded ingestions on <80% of study days, recommended adherence counseling and participant education. The threshold of checking the dashboard at least every 3 weeks was specified post hoc to identify which HCPs were looking at the dashboard between monthly study site visits with participants. HCPs who did not meet the above criteria were considered “low dashboard use” providers (LDUPs). This analysis consisted of two groups of participants: the modified intent-to-treat (mITT) population included participants who completed ≥3 months of AS use or took ≥80% of their study medication during the first 3 months of the primary study, while the population who discontinued early (D/C) included participants who discontinued prior to 3 months of AS use. Clinical assessments were collected in the mITT population at baseline and at each participant’s last study visit, which occurred between 3 and 6 months after study initiation; clinical assessments included the Positive and Negative Syndrome Scale (PANSS),Citation48 Clinical Global Impression–Severity of Illness (CGI-S) and CGI-Improvement (CGI-I),Citation49 and Personal and Social Performance (PSP) scales.Citation50 HCPs completed the Physician Utility Survey at study termination.
Statistical Analyses
Mann–Whitney U-tests and rank-biserial correlation coefficient (r) effect sizes were used to determine whether the change from baseline to assessment at last visit in clinical assessments and mean scores for the Physician Utility Survey differed between participants with HDUPs and participants with LDUPs. Python Programming Language (version 3.8) was used for these analyses, with the pingouin package and significance criteria of p≤0.05.
Results
Patient Characteristics
A total of 277 participants enrolled in the study, with a mean baseline PANSS score of 71.5. Of the full study population, 88.1% had taken aripiprazole in the past (though were not necessarily taking it at the study start); additional medications taken prior to study start have been described previously.Citation46 There were 113 participants included in the mITT population and 164 participants in the D/C population who discontinued prior to 3 months in the study. The primary study reached interim analysis criteria, showing a benefit to participants from the intervention, and was stopped early for efficacy. Within the post hoc analysis group, 34/164 participants (21%) were discontinued by the sponsor for this reason. Participant demographics are shown in .
Table 1 Participant Demographics
Frequency of Dashboard Usage
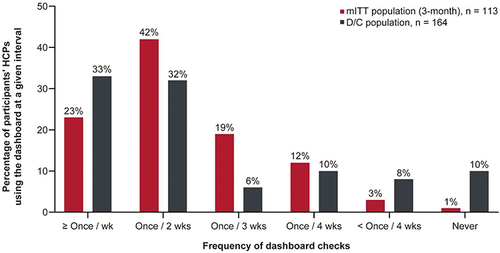
An example dashboard readout for fictional study participants is depicted in Figure S1. The dashboard included data on the participant’s ingestion record, mood, step counts, and rest amount and quality. HCPs demonstrated a high overall frequency of AS dashboard use (). In the mITT population, 95/113 (84.1%) participants’ HCPs checked the dashboard at least once every 3 weeks. Among the D/C population, 117/164 (71.3%) participants’ HCPs checked the dashboard at least once every 3 weeks.
Figure 1 Frequency of participants’ HCPs’ dashboard usage.
Dashboard Features Used by HCPs
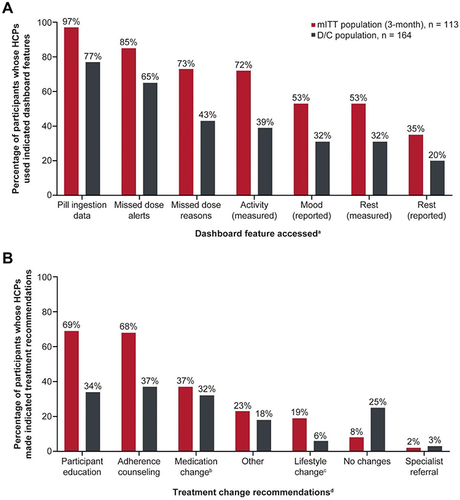
Information on pill ingestion and missed-dose alerts were the most common dashboard features HCPs reported using in both groups; as shown in , fewer of the D/C population’s HCPs used these features compared with mITT participants’ HCPs (pill ingestion feature: D/C, 77%; mITT, 97%). Participant-reported rest was the dashboard feature used least by HCPs (mITT, 35%; D/C, 20%).
Figure 2 Dashboard features used by HCPs and resulting treatment decisions.
Treatment Recommendations Resulting from Dashboard Usage
In the mITT population, most participants’ HCPs recommended participant education (69%) and adherence counseling (68%), while 37% of HCPs opted to make medication changes (). Referral to a specialist was the least common change to a treatment plan, made by 2% of HCPs. Few HCPs (8%) reported making no changes to their participants’ treatment plan. Among the D/C population’s HCPs, adherence counseling and participant education were the most common treatment recommendations (37% and 34%, respectively), with 32% of HCPs opting to make a medication change (). Referral to a specialist was recommended least often, with 3% of D/C participants’ HCPs opting for this change to the treatment plan. One-quarter of D/C participants’ HCPs reported making no changes to the treatment plan, though this may have been impacted by participants’ early discontinuation.
Change from Baseline in Clinical Assessments
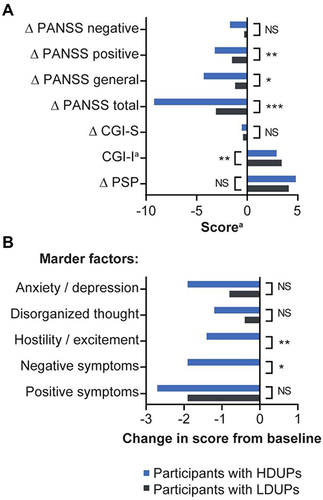
Clinical assessments were only analyzed for participants in the mITT population who completed ≥3 months of treatment to ensure sufficient duration of time for participants to gain familiarity with AS and for HCPs to make substantial use of the dashboard. As shown in and , participants with HDUPs (n=61) demonstrated significantly greater improvements from baseline in CGI-I (p=0.004), total PANSS (p=0.0002), PANSS general subscale (p=0.02), and PANSS positive subscale (p=0.003) compared with participants with LDUPs (n=52). The effect size of changes in scores from baseline between participants with HDUPs versus LDUPs in CGI-I (r=0.30), PANSS positive subscale (r=0.33), and total PANSS (r=0.40) were considered medium,Citation51 while the effect size of changes in scores from baseline in PANSS general subscale (r=0.26) and PANSS negative subscale (r=0.20) were considered small ().Citation51 Participants with HDUPs were slightly older compared with participants with LDUPs (mean age, 48 years versus 42 years) and had slightly higher total PANSS scores at baseline (74 versus 69; p=0.002). Age was not significantly correlated with changes in any of the clinical scales. Differences between participants’ scores with HDUPs versus LDUPs for PANSS negative subscale, CGI-S, and PSP scales were not statistically significant. Marder factors corresponding to hostility/excitement and negative symptoms demonstrated significantly greater improvement from baseline in participants with HDUPs compared with participants with LDUPs ( and ). The effect size of the change from baseline for hostility/excitement (r=0.31) was considered medium between participants with HDUPs versus LDUPs, while the effect size for negative symptoms (r=0.24) was considered small.Citation51
Table 2 Clinical Outcome Assessments by Participants’ HCPs’ Dashboard Usage
Figure 3 Participant scores on clinical outcome measures in the mITT population.
Perceived Usefulness of the AS System
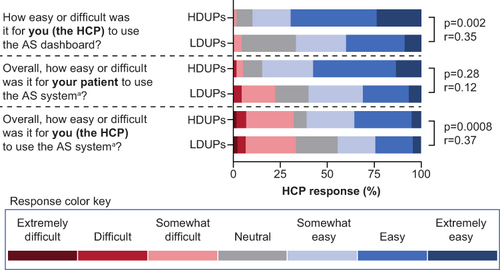
Based on responses to the Physician Utility Survey shown in and in Tables S1 and S2, both HDUPs and LDUPs found the dashboard somewhat easy, easy, or extremely easy to use (cumulative percentages between groups: 89.8% and 66.7%, respectively [comparison of mean between groups: p=0.0008; r=0.37]). Most HCPs found the overall AS system somewhat easy, easy, or extremely easy to use, with a total of 84.8% of HDUPs and 60.0% of LDUPs responding in this manner (p=0.002; r=0.37) (). A total of 61.0% of HDUPs reported that their patients found AS somewhat easy, easy, or extremely easy to use, while 44.4% of LDUPs reported the same; conversely, 32.2% of HDUPs reported that their patients found using AS somewhat difficult, difficult, or extremely difficult compared with 33.3% of LDUPs (p=0.28; r=0.12). Notably, most HDUPs (total of 79.7%) and LDUPs (total of 66.7%) felt that the AS system was at least somewhat helpful in improving conversations with study participants about their treatment plan and progress. A total of 81.4% of HDUPs and 77.8% of LDUPs found AS to be helpful in engaging participants in self-management of their condition.
Figure 4 Comparison of select paraphrased utility and satisfaction results from HCPs in the Physician Utility Survey.
Discussion
This post hoc analysis focused on usage patterns of the HCP dashboard feature of the AS system, which was accessed by HCPs caring for outpatients with schizophrenia who had a history of psychiatric hospitalization. Dashboard usage was high among HCPs regardless of whether participants completed 3 months on AS or discontinued early, with 84% and 71% of the participants’ HCPs checking the dashboard at least every 3 weeks, respectively. HCPs for participants in the D/C population were slightly more likely to report checking the dashboard less than once every 4 weeks or never, though this may be because of minimal time on study due to participant discontinuation. The features of the AS dashboard accessed most frequently by both the mITT and D/C group HCPs were the ingestion information and missed-dose alerts. These data helped inform HCP treatment decisions, with approximately two-thirds of participants’ HCPs in the mITT population recommending adherence counseling (68%) and/or participant education (69%). In the D/C population, notably fewer participants’ HCPs opted to recommend adherence counseling (37%) or participant education (34%), though this may again be due to shorter time on the AS system for these participants. HCPs were similarly likely to recommend a medication change (32%) among D/C participants. Participants with HCPs who used the AS dashboard frequently (ie, checked the dashboard at least every 3 weeks and recommended adherence counseling/patient education) saw greater improvements from baseline in clinical assessments compared with participants with HCPs who used the dashboard less often. These included improvements in PANSS total, PANSS general subscale, and PANSS positive subscale scores; Marder factors corresponding to hostility/excitement and negative symptoms; and CGI-I. Most HCPs found the dashboard and overall AS system easy to use, though HDUPs rated the system higher in usability than did LDUPs (Table S1). Most study participants found AS to be helpful in improving communication with their healthcare team. Overall, HCPs caring for patients with schizophrenia found that the AS dashboard provided useful information and aided communication relative to participants’ care plan.
Successful treatment for schizophrenia focuses on three components: (1) patients adhering to a treatment regimen; (2) patients self-engaging in the management of their condition; and (3) developing effective therapeutic relationships between patients and their HCPs.Citation52 Optimizing pharmacotherapy can be challenging for providers. If a patient is not achieving sufficient symptom relief, the HCP must determine if the treatment plan needs to be modified or if the patient is not taking their medication consistently.Citation53 Accurately assessing adherence during outpatient care is challenging,Citation53 as providers often overestimate adherence compared with pharmacy records, even among established patients.Citation54 When the treatment team is unaware of patient nonadherence, they may conclude incorrectly that the medication is not working.Citation13 Likewise, some antipsychotics that require weeks or months to reach maximal efficacy can reduce adherence because the patient believes the therapy does not work.Citation12,Citation16 This may lead to unnecessary adjustments to the treatment regimen, such as increasing dosage, changing medications, or adding new medications.Citation13 The AS system can provide this key information to inform a patient’s care plan; as an example, when providers had access to patient drug adherence information, they made more informed treatment decisions for nonadherent or poorly controlled patients compared with providers who did not have that information.Citation55
Achieving maximal symptom relief is further complicated by how different types of patients’ symptoms respond to treatment. While antipsychotic medications are generally effective at reducing positive symptoms of psychosis, negative symptoms are considered insufficiently treated with current pharmacologic options.Citation56 In our study, participants with HDUPs demonstrated greater improvements in CGI-I, PANSS, and multiple PANSS subscales compared with participants with LDUPs. To identify the impact of baseline PANSS scores on posttreatment change in PANSS scores, we further split groups of HDUPs and LDUPs into participants with baseline PANSS scores <75 (mild-to-moderate symptom severity, n=68; range, 60–74) and those with PANSS scores ≥75 (moderate-to-severe symptom severity, n=45; range, 75–90).Citation57 Among participants with LDUPs, those with less severe symptoms had a relatively small mean change from baseline compared with participants with more severe symptoms, who saw a comparatively large change from baseline (−1.5 versus −8.0). Among participants with HDUPs, there was less difference in mean change in PANSS scores from baseline based on symptom severity at study entry (−7.8 for mild-to-moderate symptoms versus −10.6 for moderate-to-severe symptoms). The difference in improvement for participants with mild-to-moderate symptoms was significantly different in those with LDUPs versus HDUPs (−1.5 and −7.8, respectively [p=0.006]); in contrast, the improvement from baseline in participants with more severe symptoms did not significantly differ between LDUP and HDUP groups (−8.0 and −10.6, respectively [p=0.24]). There was a numerical improvement in participants with more severe symptoms in the HDUP group, but the small sample size was not sufficient to see statistical significance, warranting further analysis on a larger sample of participants. These findings parallel a recent meta-analysis of schizophrenia clinical trials, in which patients with higher baseline PANSS scores demonstrated greater improvement following treatment.Citation58 Thus, while baseline PANSS clearly impacts changes in these clinical scales, the effect of HCP engagement is robust and may help mitigate the gap between different tiers of disease severity.
Relative to other scales, differences between study participants with HDUPs versus LDUPs were not statistically significant for PANSS negative subscale, CGI-S, and PSP scales; this was likely due to the magnitude of the differences and sample sizes. However, Marder factors for hostility/excitement and negative symptoms improved significantly more in participants with HDUPs. In a recent meta-analysis, the use of psychological or psychosocial interventions significantly improved negative symptoms in patients experiencing psychosis compared with care as usual.Citation59 The authors of this meta-analysis noted that increased social contact might mitigate the impact on psychosis of nearly every psychological or psychosocial intervention studied, highlighting the importance of developing the participant–provider relationship.Citation59
Interactions between patients and providers can serve as critical junctures at which providers can use personalized interventions to improve clinical outcomes, such as adherence counseling.Citation52 However, implementation of these practices may be inadequate in clinical settings. In a study of commercially insured patients with SMI in postacute settings, only 58% of first visits with providers involved discussion of compliance with antipsychotic medication, a lower rate than that for patients with either bipolar disorder (64%) or major depression (63%).Citation52 This is notable given a 2021 study by Forma et al, in which patients who had ≥2 discussions about medication adherence with their providers had a 76% reduced risk of an acute psychiatric event during the following year.Citation60 A recent study by Xia et al using a person-centered adherence counseling intervention among patients with SMI found that the intervention increased adherence 30 days postdischarge by 33% and reduced the likelihood of rehospitalization (odds ratio: 0.32; 95% CI: 0.11–0.93 [p=0.037]) compared with patients given treatment as usual.Citation61 A meta-analysis of six studies of adherence therapy given to patients with schizophrenia spectrum disorders found a significant improvement in psychiatric symptoms compared with treatment as usual.Citation62 In our study, participants whose HCPs used the dashboard more and recommended counseling and education showed greater improvements in schizophrenia symptom severity. This is notable given the findings from the primary analysis of this study by Cohen et al,Citation46 which reported significant reductions in psychiatric hospitalizations when participants used AS. By providing objective, longitudinal feedback, AS may help providers identify which patients might benefit from targeted interventions, such as adherence counseling.
In a recent study by Browne et al, patients rating therapeutic alliances with their providers favorably was associated with patients having greater treatment engagement.Citation63 Similarly, providers or observers rating patient therapeutic alliances favorably was associated with greater treatment engagement and improved positive and negative symptoms.Citation63 In our analysis, 32.2% of the HDUPs and 33.3% of the LDUPs reported that study participants found AS at least somewhat difficult to use. This contrasts with participants’ own reports of usability as reported in a separate post hoc analysis of the primary study, in which only 12% of the participants reported AS at least somewhat difficult to use.Citation64 This discrepancy in participants’ responses occurred to a similar degree in LDUPs and HDUPs. In our study, 74.0% of the HCPs (both HDUPs and LDUPs) reported that the AS system helped engage study participants in self-management of their condition. Moreover, 79.8% of the HCPs indicated that AS improved conversations with study participants about their treatment plan and progress. These findings suggest that the AS system can create opportunities to increase or improve communication between patients and providers. Objective medication ingestion data can serve to guide discussions about medication adherence and the participant’s treatment plan and help foster communication to grow the patient–provider therapeutic alliance. Additionally, AS can help bridge the care gap between office visits by alerting providers to when participants discontinue their medications.
This study was limited by the overall high usage of the dashboard by HCPs, which restricts exploration of potential effects of very low dashboard use, and by the relatively small sample sizes. As our findings are based on post hoc subgroups, possible biases may exist due to confounders inherent in these data. For example, participants who stayed on treatment long enough for HCPs to take treatment actions may have had better underlying prognoses compared with those participants who discontinued early. Thus, we analyzed clinical outcomes only in the mITT population, in which participants either completed 3 months’ AS use or took ≥80% of their study medication. HCPs of the D/C participants had less time to make treatment recommendations, and any changes that were made to treatment recommendations may have had insufficient time to impact participants’ symptoms before study discontinuation. Additionally, the improvement in scores in patients in the HDUP group may reflect inherent qualities of those HCPs; further studies are needed to address this limitation. Finally, although 60% of the participants discontinued the study (some of whom were discontinued due to early termination for efficacy), this was within the range of 19–75% as reported in a meta-analysis of clinical trials of antipsychotic medications;Citation65 more research is required to understand how the digital nature of the AS system impacts its uptake and use by patients with SMI and their care providers.
Conclusion
Providers who care for patients with schizophrenia found that the AS dashboard was easy to use and improved communication with study participants. Higher provider dashboard usage was associated with improvements in PANSS scores (total score and positive and general subscales) and in Marder factor scores for negative symptoms and hostility/excitement. The HCP dashboard for the AS system may promote discussion between providers and patients about adherence and regular medication-taking and aid HCPs in making treatment decisions, potentially leading to better patient outcomes.
Data Sharing Statement
To submit inquiries related to Otsuka clinical research, or to request access to individual participant data (IPD) associated with any Otsuka clinical trial, please visit https://clinical-trials.otsuka.com. For all approved IPD-access requests, Otsuka will share anonymized IPD on a remotely accessible data-sharing platform.
Ethics Approval and Informed Consent
The trial was conducted by study investigators, coordinators, raters, and nurses, in accordance with local laws and the International Council for Harmonisation Good Clinical Practice guidelines. The protocol was approved by Advarra for trial sites 1–56, 58–62, 65–67, and 72–75; by The Nathan Kline Institute for Psychiatric Research for trial site 57; by the Springfield Committee for Research Involving Human Subjects (Southern Illinois University School of Medicine) for trial site 63; and by WIRB-Copernicus for trial site 70. After receiving a complete trial description, all participants signed a written informed consent form. Participants were identified by unique numbers to protect their privacy.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
JMC and HF are employees of Otsuka Pharmaceutical Development & Commercialization, Inc. JCRF was an employee of Otsuka Pharmaceutical Development & Commercialization, Inc at the time the study was conducted. JGS is the principal investigator and sole owner of Uptown Research Institute, LLC, which has received clinical trial grants from Otsuka. EAC has no conflicts to disclose. JPL has received research grant support from Avanir, Roche, Takeda, Otsuka, Lundbeck, Intracellular, and GW Pharmaceuticals. The authors report no other conflicts of interest in this work.
Acknowledgments
The authors would like to thank the clinicians, study staff, participants, and the families of those who kindly participated in this study. Medical writing support for this manuscript was provided by Shawna Matthews, PhD (ORCID: 0000-0003-2332-385X), of Oxford PharmaGenesis Inc., Newtown, PA, USA, in accordance with Good Publication Practice 3 (GPP3) guidelines (http://www.ismpp.org/gpp3), and was funded by of Otsuka Pharmaceutical Development & Commercialization, Inc.
Additional information
Funding
References
- Charlson FJ, Ferrari AJ, Santomauro DF, et al. Global epidemiology and burden of schizophrenia: findings from the Global Burden of Disease Study 2016. Schizophr Bull. 2018;44(6):1195–1203. doi:10.1093/schbul/sby058
- Desai R, Nayak RE. Effects of medication nonadherence and comorbidity on health resource utilization in schizophrenia. J Manag Care Spec Pharm. 2019;25(1):37–46. doi:10.18553/jmcp.2019.25.1.037
- Schizophrenia. National Institute of Mental Health; 2018. Available from: https://www.nimh.nih.gov/health/statistics/schizophrenia. Accessed March 4, 2022.
- Chen E, Bazargan-Hejazi S, Ani C, et al. Schizophrenia hospitalization in the US 2005–2014: examination of trends in demographics, length of stay, and cost. Medicine. 2021;100(15):e25206. doi:10.1097/md.0000000000025206
- Mojtabai R. Estimating the prevalence of schizophrenia in the United States using the multiplier method. Schizophr Res. 2021;230:48–49. doi:10.1016/j.schres.2021.02.010
- Fitch K, Iwasaki K, Villa KF. Resource utilization and cost in a commercially insured population with schizophrenia. Am Health Drug Benefits. 2014;7(1):18–26.
- Oakley P, Kisely S, Baxter A, et al. Increased mortality among people with schizophrenia and other non-affective psychotic disorders in the community: a systematic review and meta-analysis. J Psychiatr Res. 2018;102:245–253. doi:10.1016/j.jpsychires.2018.04.019
- Wander C. Schizophrenia: opportunities to improve outcomes and reduce economic burden through managed care. Am J Manag Care. 2020;26(3 Suppl):S62–S68. doi:10.37765/ajmc.2020.43013
- Patel KR, Cherian J, Gohil K, Atkinson D. Schizophrenia: overview and treatment options. P T. 2014;39(9):638–645.
- Vita A, Minelli A, Barlati S, et al. Treatment-resistant schizophrenia: genetic and neuroimaging correlates. Front Pharmacol. 2019;10:402. doi:10.3389/fphar.2019.00402
- Correll CU, Schooler NR. Negative symptoms in schizophrenia: a review and clinical guide for recognition, assessment, and treatment. Neuropsychiatr Dis Treat. 2020;16:519–534. doi:10.2147/NDT.S225643
- Vadiei N, Chien J, Enwereji J, Myslinski B, Guzman A. Start low, go fast? Antipsychotic titration patterns at an inpatient psychiatric hospital. Ment Health Clin. 2020;10(5):275–281. doi:10.9740/mhc.2020.09.275
- Haddad PM, Brain C, Scott J. Nonadherence with antipsychotic medication in schizophrenia: challenges and management strategies. Patient Relat Outcome Meas. 2014;5:43–62. doi:10.2147/prom.S42735
- Lam WY, Fresco P. Medication adherence measures: an overview. Biomed Res Int. 2015;2015:217047. doi:10.1155/2015/217047
- Greene M, Yan T, Chang E, Hartry A, Touya M, Broder MS. Medication adherence and discontinuation of long-acting injectable versus oral antipsychotics in patients with schizophrenia or bipolar disorder. J Med Econ. 2018;21(2):127–134. doi:10.1080/13696998.2017.1379412
- Semahegn A, Torpey K, Manu A, Assefa N, Tesfaye G, Ankomah A. Psychotropic medication non-adherence and its associated factors among patients with major psychiatric disorders: a systematic review and meta-analysis. Syst Rev. 2020;9(1):17. doi:10.1186/s13643-020-1274-3
- Kim J, Ozzoude M, Nakajima S, et al. Insight and medication adherence in schizophrenia: an analysis of the CATIE trial. Neuropharmacology. 2020;168:107634. doi:10.1016/j.neuropharm.2019.05.011
- Kane JM, Correll CU. Optimizing treatment choices to improve adherence and outcomes in schizophrenia. J Clin Psychiatry. 2019;80(5). doi:10.4088/JCP.IN18031AH1C
- Desalegn D, Girma S, Abdeta T. Quality of life and its association with current substance use, medication non-adherence and clinical factors of people with schizophrenia in Southwest Ethiopia: a hospital-based cross-sectional study. Health Qual Life Outcomes. 2020;18(1):82. doi:10.1186/s12955-020-01340-0
- Di CS, Upthegrove R, Mallikarjun P. The relapse rate and predictors of relapse in patients with first-episode psychosis following discontinuation of antipsychotic medication. Early Interv Psychiatry. 2018;12(5):893–899. doi:10.1111/eip.12385
- Trang A. Continuity of care for patients with schizophrenia in communities with limited resources. Ment Illn. 2018;10(1):7585. doi:10.4081/mi.2018.7585
- van der Lee APM, Hoogendoorn A, de Haan L, Beekman ATF. Discontinuity of psychiatric care for patients with schizophrenia, relation to previous psychiatric care and practice variation between providers: a retrospective longitudinal cohort study. BMC Psychiatry. 2021;21(1):319. doi:10.1186/s12888-021-03319-7
- Haggerty JL, Reid RJ, Freeman GK, Starfield BH, Adair CE, McKendry R. Continuity of care: a multidisciplinary review. BMJ. 2003;327(7425):1219–1221. doi:10.1136/bmj.327.7425.1219
- Freeman GK, Olesen F, Hjortdahl P. Continuity of care: an essential element of modern general practice? Fam Pract. 2003;20(6):623–627. doi:10.1093/fampra/cmg601
- Nowak DA, Sheikhan NY, Naidu SC, Kuluski K, Upshur REG. Why does continuity of care with family doctors matter? Review and qualitative synthesis of patient and physician perspectives. Can Fam Physician. 2021;67(9):679–688. doi:10.46747/cfp.6709679
- van der Lee A, de Haan L, Beekman A. Schizophrenia in the Netherlands: continuity of care with better quality of care for less medical costs. PLoS One. 2016;11(6):e0157150. doi:10.1371/journal.pone.0157150
- Hoertel N, Limosin F, Leleu H. Poor longitudinal continuity of care is associated with an increased mortality rate among patients with mental disorders: results from the French National Health Insurance Reimbursement Database. Eur Psychiatry. 2014;29(6):358–364. doi:10.1016/j.eurpsy.2013.12.001
- Sanatinia R, Cowan V, Barnicot K, et al. Loss of relational continuity of care in schizophrenia: associations with patient satisfaction and quality of care. BJPsych Open. 2016;2(5):318–322. doi:10.1192/bjpo.bp.116.003186
- Smith TE, Easter A, Pollock M, Pope LG, Wisdom JP. Disengagement from care: perspectives of individuals with serious mental illness and of service providers. Psychiatr Serv. 2013;64(8):770–775. doi:10.1176/appi.ps.201200394
- Reinert M, Fritze D, Nguyen T. Report: the state of mental health in America; 2022. Available from: https://mhanational.org/sites/default/files/2022%20State%20of%20Mental%20Health%20in%20America.pdf. Accessed July 5, 2022.
- National Council for Behavioral Health. America’s mental health 2018; 2018. Available from: https://www.cohenveteransnetwork.org/wp-content/uploads/2018/10/Research-Summary-10-10-2018.pdf. Accessed July 8, 2022.
- Torrey WC, Drake RE. Practicing shared decision making in the outpatient psychiatric care of adults with severe mental illnesses: redesigning care for the future. Community Ment Health J. 2010;46(5):433–440. doi:10.1007/s10597-009-9265-9
- Kowalski CP, McQuillan DB, Chawla N, et al. ‘The hand on the doorknob’: visit agenda setting by complex patients and their primary care physicians. J Am Board Fam Med. 2018;31(1):29–37. doi:10.3122/jabfm.2018.01.170167
- Anghel LA, Farcas AM, Oprean RN. An overview of the common methods used to measure treatment adherence. Med Pharm Rep. 2019;92(2):117–122. doi:10.15386/mpr-1201
- Knights J, Heidary Z, Peters-Strickland T, Ramanathan M. Evaluating digital medicine ingestion data from seriously mentally ill patients with a Bayesian Hybrid Model. NPJ Digit Med. 2019;2(1):20. doi:10.1038/s41746-019-0095-z
- De Las Cuevas C, de Leon J. Self-report for measuring and predicting medication adherence: experts’ experience in predicting adherence in stable psychiatric outpatients and in pharmacokinetics. Patient Prefer Adherence. 2020;14:1823–1842. doi:10.2147/PPA.S242693
- Torous J, Staples P, Barnett I, Onnela JP, Keshavan M. A crossroad for validating digital tools in schizophrenia and mental health. NPJ Schizophr. 2018;4(1):6. doi:10.1038/s41537-018-0048-6
- Lim MH, Penn DL. Using digital technology in the treatment of schizophrenia. Schizophr Bull. 2018;44(5):937–938. doi:10.1093/schbul/sby081
- Gallinat C, Moessner M, Apondo S, Thomann PA, Herpertz SC, Bauer S. Feasibility of an intervention delivered via mobile phone and internet to improve the continuity of care in schizophrenia: a randomized controlled pilot study. Int J Environ Res Public Health. 2021;18(23):12391. doi:10.3390/ijerph182312391
- Gay K, Torous J, Joseph A, Pandya A, Duckworth K. Digital technology use among individuals with schizophrenia: results of an online survey. JMIR Ment Health. 2016;3(2):e15. doi:10.2196/mental.5379
- Substance Abuse and Mental Health Services Administration. Report: using technology-based therapeutic tools in behavioral health services. Treatment Improvement Protocol (TIP) series 60. Rockville, MD. HHS Publication; 2015.
- Steinkamp JM, Goldblatt N, Borodovsky JT, et al. Technological interventions for medication adherence in adult mental health and substance use disorders: a systematic review. JMIR Ment Health. 2019;6(3):e12493. doi:10.2196/12493
- Kopelowicz A, Baker RA, Zhao C, Brewer C, Lawson E, Peters-Strickland T. A multicenter, open-label, pilot study evaluating the functionality of an integrated call center for a digital medicine system to optimize monitoring of adherence to oral aripiprazole in adult patients with serious mental illness. Neuropsychiatr Dis Treat. 2017;13:2641–2651. doi:10.2147/NDT.S143091
- Frias J, Virdi N, Raja P, Kim Y, Savage G, Osterberg L. Effectiveness of digital medicines to improve clinical outcomes in patients with uncontrolled hypertension and type 2 diabetes: prospective, open-label, cluster-randomized pilot clinical trial. J Med Internet Res. 2017;19(7):e246. doi:10.2196/jmir.7833
- Fowler JC, Cope N, Knights J, et al. Hummingbird Study: results from an exploratory trial assessing the performance and acceptance of a digital medicine system in adults with schizophrenia, schizoaffective disorder, or first-episode psychosis. Neuropsychiatr Dis Treat. 2021;17:483–492. doi:10.2147/ndt.S290793
- Cohen EA, Skubiak T, Boskovic DH, et al. Phase 3b multicenter, prospective, open-label trial to evaluate the effects of a digital medicine system on inpatient psychiatric hospitalization rates for adults with schizophrenia. J Clin Psychiatry. 2022;83(3):21m14132. doi:10.4088/JCP.21m14132
- Abilify MyCite (aripiprazole tablets with sensor), for oral use; 2020.
- Kay S, Fiszbein A, Opler L. The Positive and Negative Syndrome Scale (PANSS) for schizophrenia. Schizophr Bull. 1987;13(2):261–276. doi:10.1093/schbul/13.2.261
- Busner J, Targum SD. The Clinical Global Impressions Scale: applying a research tool in clinical practice. Psychiatry. 2007;4(7):28–37.
- Juckel G. Personal and social performance scale. In: Michalos AC, editor. Encyclopedia of Quality of Life and Well-Being Research. Springer, Dordrecht; 2014:4719–4724. doi:10.1007/978-94-007-0753-5_2141
- Cohen J. The significance of a product moment rs. In: Statistical Power Analysis for the Behavioral Sciences. Lawrence Erlbaum Associates; 1988:75–108.
- Martin C, Koep E, White J, Belland A, Waters H, Forma F. Treatment compliance communications between patients with severe mental illness and treating healthcare providers: a retrospective study of documentation using healthcare reimbursement claims and medical chart abstraction. Pragmat Obs Res. 2021;12:49–63. doi:10.2147/POR.S303453
- Martin KB. Accuracy of psychiatrists’ assessment of medication adherence in an outpatient setting. Cureus. 2020;12(12):e11847. doi:10.7759/cureus.11847
- Stephenson JJ, Tunceli O, Gu T, et al. Adherence to oral second-generation antipsychotic medications in patients with schizophrenia and bipolar disorder: physicians’ perceptions of adherence vs. pharmacy claims. Int J Clin Pract. 2012;66(6):565–573. doi:10.1111/j.1742-1241.2012.02918.x
- Shafrin J, Schwartz TT, Lakdawalla DN, Forma FM. Estimating the value of new technologies that provide more accurate drug adherence information to providers for their patients with schizophrenia. J Manag Care Spec Pharm. 2016;22(11):1285–1291. doi:10.18553/jmcp.2016.22.11.1285
- Căpățînă OO, Micluția IV, Fadgyas-Stănculete M. Current perspectives in treating negative symptoms of schizophrenia: a narrative review. Exp Ther Med. 2021;21(3):276. doi:10.3892/etm.2021.9707
- Leucht S, Kane JM, Kissling W, Hamann J, Etschel E, Engel RR. What does the PANSS mean? Schizophr Res. 2005;79(2–3):231–238. doi:10.1016/j.schres.2005.04.008
- Gopalakrishnan M, Zhu H, Farchione TR, et al. The trend of increasing placebo response and decreasing treatment effect in schizophrenia trials continues: an update from the US Food and Drug Administration. J Clin Psychiatry. 2020;81(2). doi:10.4088/JCP.19r12960
- Lutgens D, Gariepy G, Malla A. Psychological and psychosocial interventions for negative symptoms in psychosis: systematic review and meta-analysis. Br J Psychiatry. 2017;210(5):324–332. doi:10.1192/bjp.bp.116.197103
- Forma F, Koep E, White J, Belland A, Waters H, Martin C. Impact of treatment-related discussions on healthcare resource use and costs among patients with severe mental illness. Curr Med Res Opin. 2021;37(10):1799–1809. doi:10.1080/03007995.2021.1943341
- Xia XS, Poremski D, Ubana RL, Ravichandran N. Promoting medication adherence among psychiatric patients with a history of nonadherence: a clinical practice improvement program. J Psychiatr Pract. 2020;26(4):284–293. doi:10.1097/PRA.0000000000000482
- Gray R, Bressington D, Ivanecka A, et al. Is adherence therapy an effective adjunct treatment for patients with schizophrenia spectrum disorders? A systematic review and meta-analysis. BMC Psychiatry. 2016;16(1):90. doi:10.1186/s12888-016-0801-1
- Browne J, Wright AC, Berry K, et al. The alliance-outcome relationship in individual psychosocial treatment for schizophrenia and early psychosis: a meta-analysis. Schizophr Res. 2021;231:154–163. doi:10.1016/j.schres.2021.04.002
- Cochran JM, Fang H, Le Gallo C, Peters-Strickland T, Lindenmayer JP, Reuteman-Fowler JC. Participant Engagement and Symptom Improvement: Aripiprazole Tablets with Sensor for the Treatment of Schizophrenia. 2022;16:1805–1817. doi: 10.2147/PPA.S362889
- Rabinowitz J, Levine SZ, Barkai O, Davidov O. Dropout rates in randomized clinical trials of antipsychotics: a meta-analysis comparing first- and second-generation drugs and an examination of the role of trial design features. Schizophr Bull. 2009;35(4):775–788. doi: 10.1093/schbul/sbn005