Abstract
Background and objectives:
Previous studies in alcohol-dependent patients have shown an attentional bias (AB) under related substance cues, which can lead to relapse. This AB can be evaluated by the alcohol Stroop test (AST). The AST is a modified Stroop task in which participants have to name the color of an alcohol-related word or a neutral word. AB is the response-time difference between these two types of words. The goal of the current study was to examine modification of AB during specialized hospitalization for alcohol dependence, with the suppression of a training bias that could be present in within-subject design.
Methods:
Individuals with alcohol-dependence disorders (Diagnostic and Statistical Manual of Mental Disorders, 4th edition) and admitted for withdrawal in the addiction unit of the University Hospital of Clermont-Ferrand (test group, n = 42) and persons with no alcohol or psychiatric disorder (control group, n = 16), recruited among colleagues and friends of the staff, performed the AST. A subgroup of the test group performed the AST in admission (admission group, n = 19), and another subgroup undertook the test immediately before discharge (discharge group, n = 23).
Results:
Results showed an AB only for patients seen at admission (F[1,55] = 3.283, P = 0.075). Moreover, we observed that the AB in the admission group (mean = 34 ms, standard deviation [SD] = 70.06) was greater than the AB in the control group (mean = 23 ms, SD = 93.42), itself greater than the AB in the discharge group (mean = −12 ms, SD = 93.55) (t[55] = −1.71; P = 0.09).
Conclusion:
Although the results are preliminary, the present study provides evidence for changes in the AB during alcohol-addiction treatment and for the value of these methods to diminish AB during detoxification.
Introduction
Alcohol is regularly consumed by 20% of French adults, and more than 6.4 million French people consume it daily.Citation1 Alcohol is responsible for 33,000 deaths per year in France,Citation2 and comorbidity with psychiatric disorders is important.Citation3 Alcohol abuse and dependence lead to somatic, psychological, family, social, professional, and financial disruption.Citation4,Citation5
Dependent patients have a special link with the substance, with an inability to refrain from it (according to Diagnostic and Statistical Manual of Mental Disorders, 4th edition [DSM-IV] criteria).Citation6 Therapeutic strategies for alcohol dependence are based on acute treatment (withdrawal) and long-term rehabilitation.Citation7 After withdrawal, relapse prevention is the major challenge for the treatment of this disease. Usually, two approaches are combined: psychotherapy and pharmacotherapy.Citation7 Recently, new psychotherapeutic approaches developed to improve cognitive impairments described in mental illnesses (eg, schizophrenia or bipolar disorder) have been used in the treatment of addictions.Citation8
The functioning of the brain of an addicted patient may differ from that of a nonaddict.Citation9 A dependent subject no longer has full control of their external environment. This lack of control led to the observation that substance-related stimuli (ie, the word “alcohol” for an alcohol-dependent patient) induced strong activation compared with non-substance-related stimuli. This activation results in an attentional bias (AB) in which the attentional system is not able to filter correctly the external information. AB can also be defined as “a phenomenon whereby attentional channeling is directed toward personally valued stimuli, despite an individual’s efforts to ignore them.”Citation10,Citation11 Thus, AB would be strongly associated with relapse, and in particular with craving.Citation12 Development and an increase in craving are influenced by the excess of attention to substance cues.Citation13 Thus, craving and AB are highly correlated.Citation10,Citation14–Citation16
The evaluation of AB at the end of hospitalization is evident: several authors have shown that this can predict the likelihood of relapse and therefore the effectiveness of the treatment.Citation10 Indeed, Cox et alCitation17 observed that after 4 weeks of hospitalization, patients who had a greater AB had an increased risk of relapse compared with those who had a lower AB.
One purpose of a support intervention is thus to reduce AB. The most used tool to show AB in the case of psychological disorders is a modified Stroop task.Citation11 The classic Stroop taskCitation18 is used in clinical practice to highlight attentional deficits. In this task, participants are instructed to name the color of the ink used to write a word, eg, red, when the word “door” is written in red. In 1935, Stroop showed in one of the conditions of his study that participants required more time to name the color when the word itself was an incongruent color (for example, “blue” written in red) than when it was a congruent color (“blue” written in blue). This task measures the participant’s ability to ignore irrelevant stimuli (the meaning of the word) and to focus on the relevant stimulus (the color of the word). The more the stimulus is semantically close to the color name, the more ignoring it is difficult.Citation19
The emotional Stroop task is a modification of the original to highlight a lack of attention related to an emotional concept (for review, see Williams et al).Citation11 In an emotional Stroop task, Stroop interference is achieved by words emotionally relevant for the participant. For patients with anxiety disorders, the time to name the color of the word is longer when the word is related to the concept of anxiety than when the word is neutral. In patients with post-traumatic stress disorder, this effect is especially marked when the selected words refer to the traumatic event. This interference would be a cue that the patient filters information in an inappropriate way. In this case, the concept linked to the disorder is active and present in memory automatically, and too much attention is allocated to this information.Citation20 The result is then a longer processing time to treat another feature of the stimulus – the color.
In the alcohol Stroop test (AST; recently reviewed),Citation10 stimuli are alcohol-related words. An AB towards alcohol is noticeable when participants require more time to name the color of an alcohol-related word than for a neutral word. Cox et alCitation17 showed that patients at admission to inpatient treatment have a greater AB than a group of nonabusers, who themselves have a greater AB than patients in discharge after 4 weeks of treatment.
Our study was designed to evaluate the efficacy of hospital care on the modification of AB. For this, we compared the AB score in alcohol-dependent admission to inpatient treatment in the French version of the AST. We expected to observe results similar to those of previous studies:Citation17 patients at admission should have a greater AB than nonabusers, whose AB should be greater than patients at discharge. The classic Stroop effect, measuring the general capacity of attention, should not be significantly different between these three groups, indicating that the reduction in attention bias is not due to an increase in attentional capacities. Cox et alCitation17 used a within-subjects design, which could be a problematic method because the second measure of AB could just reflect a learning process. We chose to use a between-subjects design, also indicating that the reduction in AB is not due to a learning process.
Methods
Participants
The test group was composed of alcohol-dependent participants who were recruited from the University Hospital Gabriel-Montpied in Clermont-Ferrand, and more specifically the ward devoted to the treatment of addictive disorders. All subjects were evaluated and diagnosed as dependent by a senior addiction specialist with extensive clinical experience (FP), using DSM-IV criteria.
One subgroup of the test group, the admission group, was composed of patients included during the 4 days after their admission, and another subgroup, the discharge group, was composed of patients included immediately prior to discharge, approximately 4 weeks after their admission. The control group consisted of healthy volunteers who had never presented addictive, neurological, or psychiatric disorders. They were unaware of the objectives of the study.
All participants had normal or corrected-to-normal color vision. They were French, and had no language disorders. All participants gave written informed consent to participate in this study, as required by the local ethical committee. Finally, all patients in the test group had undergone standard oxazepam treatment (see ).
Table 1 Sex and age of participants in this study
Measures
Stimuli consisted of four neutral words: “robe” (dress), “pont” (bridge), train, and studio; four words semantically related to the notion of alcohol: “alcool” (alcohol), Ricard, “vin” (wine), and whisky; and four color names: “rouge” (red), “jaune” (yellow), “bleu” (blue), and “vert” (green). Stimuli were individually presented in lowercase letters in Courier New font, 72-point bold, centered on the screen. On average, a word covered a visual angle of 3° broad and height 0.9°. There were three different blocks: one for the neutral words, one for the words for colors, and one for words related to alcohol. The color words were always presented in an incongruent way (eg, “red” appeared only in green, blue, or yellow). In addition, an analysis of the objective frequencies of the words from the French lexical database Lexique 3Citation21 showed no significant difference between alcohol-related words with the exception of the word Ricard, which was not contained in this base, and neutral words (t[5] = −0.96, P = 0.38), and color words and neutral words (t[6] = −0.4, P = 0.71).
Procedure
The experiment was conducted in a quiet room for nonabuser participants and in patients’ hospital rooms. Following the reading of consent, they were informed that the study measured their perception of color.
Participants were installed at a computer. The presentation of stimuli and recording of response times were managed and measured to the nearest millisecond by the DMDX program.Citation22 The response times were recorded by a microphone on the PC. The choice of a verbal response was preferred to the choice of a manual response. Manual response offers worse Stroop interference,Citation23 and it remains less natural, because it requires a learning phase. The participants were seated about 50 cm from the screen. They were instructed to concentrate on the fixation cross (+) for 500 ms before it was replaced by the word. They were to name the color of the word, and they were reminded to respond as quickly as possible, and without error.
As recommended,Citation24 stimuli were presented in blocks to avoid the cognitive influence of the item “alcohol” being carried over to the following item. The experiment began with a set of two practice blocks. In the first, the words were replaced by a series of Xs (eg, XXXXX). Participants had to name the colors (ten in total). This step allowed detection of possible color-perception problems or problems related to poor microphone detection. The second practice phase was the presentation of neutral words, not used in the rest of the study (“voiture” [car], “fauteuil” [chair], “route” [road], “télévision” [television], and “chaussure” [shoe]) (in total, ten items).
Finally, the three blocks were presented in random order between participants, with a pause of a few seconds between each block. In total, except for practice items, each participant saw 72 items. The words were presented in three different colors, twice for each block.
Statistical analyses
The average response time given by item for each block of correct answers was analyzed. Responses less than 300 ms and more than 1500 ms were excluded from analyses (less than 1% of data). The tests were first made on the words semantically related to alcohol, compared with neutral words, then on the color words compared with neutral words, using SPSS 19 (IBM, Armonk, NY, USA). A Shapiro-Wilk test on the two principal variables (Alcohol Stroop interference and Classical Stroop interference) indicated that these two variables were normally distributed (P = 0.37 for Alcohol Stroop interference and P = 0.097 for classical Stroop interference).
Two types of analysis were undertaken, with a repeated-measures plan of 2 × 3 with type of stimulus (color words or alcohol-related words vs neutral words) and the status of the participant (nonabusers vs admitted patient vs discharged patients). We conducted contrast analysis to assess the intensity of the Stroop effect (classic and alcohol) in different groups of patients and controls. In addition, we undertook comparisons for each type of participant with a Bonferroni adjustment on this data. Response latencies and error proportions are presented in .
Table 2 Latencies of correct answers (in milliseconds), proportions of errors, and standard deviation (in parentheses) presented by type of stimulus (color words, alcohol-related words vs neutral words) and status of the participant (nonabusers vs patients at admission vs discharged patients)
Results
Population description
Forty-two patients were recruited to the test group. Nineteen comprised the admission group, and 23 comprised the discharge group. Sixteen participants made up the control group. All characteristics of the population are listed in . There was no difference between groups on the basis of age or sex (Fs < 1).
Alcohol-related words compared with neutral words
This response-time analysis revealed an effect of type of stimulus (F[1,55] = 5.752, P < 0.05) and an effect of status of the participant (F[2,55] = 4.25, P < 0.05). The interaction between these two factors was not significant (F < 1) ().
Figure 1 Classic Stroop effect (difference in response-time average, in milliseconds, for color words and neutral words) and alcohol Stroop effect (difference in response-time average, in milliseconds, for alcohol-related and neutral words) for each participant group, and associated standard errors.
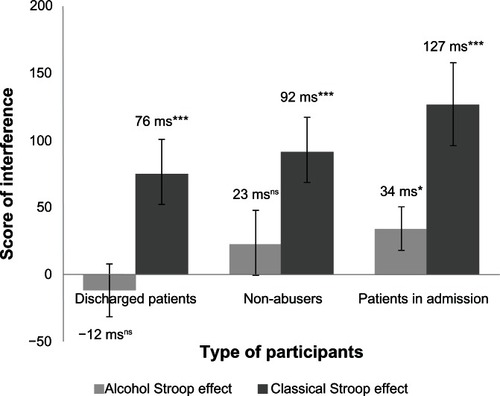
To analyze these specific results, we conducted a linear contrast analysis on the AST. This showed a trend effect of status of the participant (t[55] = −1.714, P = 0.092), indicating that patients on admission had an alcohol Stroop effect greater than the nonabusers, who themselves had a higher effect than discharged patients. Orthogonal contrasts centered on this linear contrast were not significant (t[55] = 1.174, P = 0.246).
Planned comparisons showed that patients in admission had a tendency towards an alcohol Stroop effect (34 ms, F[1,55] = 3.283, P = 0.075) while nonabusers and discharged patients did not have this alcohol Stroop effect (respectively, 23 ms, F[1,55] = 1.252, P = 0.268 and 12 ms, F[1,55] = 1.552, P = 0.218).
The mixed model on error-proportions analysis did not show any effect of type of stimulus or status of the participant, and these two factors had no interactions.
Color words compared with neutral words
The response-time analysis revealed a type of stimulus effect (F[1,55] = 43.53, P < 0.001), indicating that response times to the color words were generally greater than for neutral words. The analysis also revealed an effect of status of the participant (F[2,55] = 6.164, P < 0.05), indicating that the response times were different from nonabusers, patients at admission, or those at discharge. The interaction between these two factors was not significant (F[2,55] = 1.343, P = 0.269).
We conducted a linear contrast analysis on these data. This did not show any effect of status of the participant (t[55] = 1.393, P = 0.169) on the Stroop effect, indicating that there was no difference between the participants on the classic Stroop effect.
Planned comparisons showed a classic Stroop effect for all participants: 127 ms at admission (F[1,55] = 25.096, P < 0.001), 92 ms for nonabusers (F[1,55 = 11.178, P < 0.001], and 76 ms for discharged patients (F[1,55] = 9.497, P < 0.01).
We found no effect of type of stimulus on error proportions (F < 1), but status of the participant had an effect on error proportions (F[2,55] = 3.723, P < 0.05), and there was interaction between these two factors (F[2,55] = 3.134, P = 0.05). Planned comparisons showed that only patients on admission had a difference in error proportions (F[2,55] = 5.63, P < 0.05).
Discussion
Our results on AB measured with a French version of the AST showed a trend difference between our three groups of participants: AB was greater in patients on admission, whose AB was greater than that of nonabusers, who had a greater AB than that observed in discharged patients. These results suggest an improvement in cognitive performances against related-substance cues in the treatment period.
In spite of low statistical power, these results are consistent with those reported in the literature.Citation17 While we observed a decrease in the classic Stroop effect on response times, it did not differ significantly between the different types of participant. This seems to indicate that the observed decrease in AB was not completely due to a better attentional process, nor to an effect of the attentional process of the oxazepam treatment, which is in accordance with the literature.Citation17 Our results show that hospital care leads to reduced AB in alcohol-dependent patients. Our results had the same pattern as those of Cox et al,Citation17 who used a within-subjects design. A between-subjects design could be problematic for drawing conclusions, because it is difficult to be sure that there was no other factor of difference between the two groups. Our results, viewed together with previous results, seem to indicate that diminution of AB was not due to a training bias and that the difference observed between patients at admission and at discharge could be observed with the two types of design.
Williams et alCitation11 have shown that the subjective frequency of items has an influence on the Stroop task. The more frequently a word is encountered by an individual, the more it creates interference. The difference observed between our patients at admission, when they were confronted with many alcohol-related items, and our nonabusers could be explained by this phenomenon, but this seems unlikely, because we also observed a difference between patients at admission and at discharge, patients who could estimate that the subjective frequency of items used was comparable. Cox et alCitation17 used the staff in the same unit of addiction treatment as their patients, a group control, to avoid this bias. These authors continued to observe a difference between patients and the control group concerning AB. This suggests that the emotional valence of a word is more important in the emotional Stroop task than the subjective frequency. The AB reduction in patients between admission and discharge is probably due to a decline in the emotional importance of alcohol-related words.
This decrease between patients at admission and at discharge is probably an indication of the efficacy of the treatment on this dimension. Indeed, the use of psychotropic drugs (ie, oxazepam) can have an effect on the emotional processing of stimuli.Citation25 Thus, the decrease in AB for discharged patients may be due to decreased emotional perception. Moreover, the cognitive-care services probably encourage the patient to establish a functioning inhibiting process from alcohol-related cues. Indeed, patients are advised to participate in discussion groups, for psychological education and relapse prevention, and to engage in individual behavioral and cognitive therapy.
We must nevertheless be careful with these results, due to limitations on use of the Stroop task to explore AB. Indeed, the origins of AB are actually the subject of debate. This AB could be a problem of initial orientation of spatial attention or a disengagement bias. Phaf and KanCitation26 showed recently in a review that AB can occur in short stimulus-onset asynchrony (between 50 and 200 ms), which favors an initial orientation spatial bias, but also an AB with long stimulus-onset asynchrony, reflecting a disengagement bias. Field and CoxCitation10 explained that these two processes are involved in AB. Unfortunately, the Stroop task cannot distinguish between these two types of process.Citation27 The diminution observed could be attributed to either explanation. It is difficult to determine which process is enhanced by hospital care: initial spatial orientation or the disengagement process. Moreover, the emotional Stroop effect could reflect the fact that emotional stimuli are less readily suppressed or filtered in normal populations, with negative consequences for primary task performance.Citation28 Indeed, studies on the emotional Stroop task showed an effect with emotional words in a normal population.Citation29 This effect exists in reading, lexical decision, and color naming.Citation30 These tasks are all slower with emotional words, and this delay is immune to task-irrelevant variation and to changes in the relative salience of the words and the colors. Further, the delay was absent when emotional and neutral words appeared in a single block, suggesting that the so-called emotional Stroop effect could reflect a stimulus-driven generic slowdown effect rather than a selective-attention mechanism, such as that associated with the classic Stroop effect.
The AST used and developed in this study could indicate the efficacy of the general concept of AB in the hospital care of a patient, even if it cannot highlight exactly the process involved in this diminution.
At a clinical level, this study and the observation of AB in a patient population underline the importance of this process in pathology. As mentioned previously, AB is positively correlated with craving and relapse.Citation17 These data support the importance of AB in the maintenance of the disorder.
The Alcohol Attention-Control Training Program developed in a nonaddicted population shows that participants in this program reduce their alcohol consumption and their AB during the following 3 months.Citation31 This type of “reducing AB” program could be an interesting topic for treatment of alcohol dependence.
Conclusion and perspectives
This study, associated with the previous results of a study of ABCitation17 with the AST, shows a diminution of AB for hospitalized patients. Treatment that works on this AB will probably benefit the patient, and more specifically be associated with a diminution of relapse.
The use of other measures of AB could be considered to explore in more specific detail which process exactly is enhanced during treatment. An answer to this question could allow us to design a more specific rehabilitation program, and to be more efficient in the hospital care of these patients.
Acknowledgements
This work was supported by a grant from the Institut de Recherches Scientifiques, Economiques et Sociales sur les Boissons. The authors thank the three anonymous reviewers for their helpful advice, comments, and suggestions on previous drafts of the manuscript. We thank Bruno Pereira too for his assistance concerning statistical analysis.
Disclosure
The authors report no conflicts of interest in this work.
References
- CostesJMPrincipales données épidémiologiques concernant les addictions en FranceReynaudMTraité d’addictologieParisMédecine-Sciences Flammarion2006
- KhazaalYZullinoDDépendances aux substances et comorbidités psychiatriques: tendances actuelles Available from: http://guidereha.ch/sites/default/files/document/file/04_medinfo0902_dependances.pdf. Accessed August 17, 2012.
- ComptonWMThomasYFStinsonFSGrantBFPrevalence, correlates, disability, and comorbidity of DSM-IV drug abuse and dependence in the United States: results from the national epidemiologic survey on alcohol and related conditionsArch Gen Psychiatry200764556657617485608
- HeatherNPleasures and pains of our favorite drugHeatherNPetersTJStockwellTRHandbook of Alcohol Dependence and Related ProblemsNew YorkWiley2001514
- SchallMKemenyAMaltzmanIFactors associated with alcohol use in university studentsJ Stud Alcohol19925321221361560664
- American Psychiatric AssociationDiagnostic and Statistical Manual of Mental Disorders4th edWashingtonAmerican Psychiatric Association1994
- MannKHermannDIndividualised treatment in alcohol-dependent patientsEur Arch Psychiatry Clin Neurosci2010260Suppl 2S116S12020953618
- VocciFJCognitive remediation in the treatment of stimulant abuse disorders: a research agendaExp Clin Psychopharmacol200816648449719086769
- VolkowNDThe addicted human brain: insights from imaging studiesJ Clin Invest2003111101444145112750391
- FieldMCoxWAttentional bias in addictive behaviors: a review of its development, causes, and consequencesDrug Alcohol Depend2008971–212018479844
- WilliamsJMGMathewsAMacLeodCThe emotional Stroop task and psychopathologyPsychol Bull199612013248711015
- AntonRFWhat is craving? Models and implications for treatmentAlcohol Res Health199923316517310890811
- FieldMEastwoodBExperimental manipulation of attentional bias increases the motivation to drink alcoholPsychopharmacology2005183335035716235080
- FieldMChristiansenPColeJGoudieADelay discounting and the alcohol Stroop in heavy drinking adolescentsAddiction2007102457958617309540
- FieldMCraving and cognitive biases for alcohol cues in social drinkersAlcohol Alcohol200540650451016157608
- SayetteMAHuffordMREffects of cue exposure and deprivation on cognitive resources in smokersJ Abnorm Psychol199410348128187822584
- CoxWMHoganLMKristianMRRaceJHAlcohol attentional bias as a predictor of alcohol abusers’ treatment outcomeDrug Alcohol Depend200268323724312393218
- StroopJRStudies of interference in serial verbal reactionsJ Exp Psychol Gen193512111523
- NeelyJHKahanTAIs semantic activation automatic? A critical re-evaluationRoedigerHL3rdNairneJSNeathISurprenantAMThe Nature of Remembering: Essays in Honor of Robert G. CrowderWashingtonAmerican Psychological Association20016993
- PerettiCSAnxiety and cognition disordersEncephale1998243256259 French.9696920
- NewBPallierCBrysbaertMFerrandLLexique 2: a new French lexical databaseBehav Res Methods Instrum Comput200436351652415641440
- ForsterKIForsterJCDMDX: a Windows display program with millisecond accuracyBehav Res Methods Instrum Comput200335111612412723786
- MacLeodCMHalf a century of research on the Stroop effect: an integrative reviewPsychol Bull199110921632032034749
- CoxWMFadardiJSPothosEMThe addiction-Stroop test: theoretical considerations and procedural recommendationsPsychol Bull2006132344347616719569
- FouksLPinalieBPorcheronJBCardonAThe clinical activity of oxazepamActa Psychiatr Scand197858S27499103
- PhafRHKanKJThe automaticity of emotional Stroop: a meta-analysisJ Behav Ther Exp Psychiatry200738218419917112461
- MacLeodCMathewsATataPAttentional bias in emotional disordersJ Abnorm Psychol198695115203700842
- YiendJThe effects of emotion on attention: a review of attentional processing of emotional informationCogn Emot2010241347
- KahanTAHelyCDThe role of valence and frequency in the emotional Stroop taskPsychon Bull Rev200815595696018926988
- AlgomDChajutELevSA rational look at the emotional Stroop phenomenon: a generic slowdown, not a Stroop effectJ Exp Psychol Gen2004133332333815355142
- FadardiJSCoxWMReversing the sequence: reducing alcohol consumption by overcoming alcohol attentional biasDrug Alcohol Depend2009101313714519193499