
Abstract
Purpose
Evidence supporting secondary stroke in sub-Saharan Africa is scarce. This study describes the incidence of stroke recurrence and associated risk factors in sub-Saharan Africa.
Methods and Materials
Scientific databases were systematically searched from January 2000 to December 2022 for population-based observational studies, case-control or cohort studies of recurrent stroke involving adults aged 18 years and above in sub-Saharan Africa (SSA). We assessed the quality of the eligible studies using the Critical Appraisal Skills Program (CASP) checklist for observational studies.
Results
Six studies met the inclusion criteria and were included in this study. Stroke recurrence rates in SSA ranged from 9.4% to 25%. Majority of the studies were conducted from Western Africa and showed that stroke recurrence rates are high within sub-Saharan Africa ranging from 2% to 25%. The known stroke risk factors such as hypertension, chronic alcohol consumption, etc., remained the leading causes of stroke recurrence. The studies reported a higher mortality rate ranging from 20.5 −23% among those with recurrent strokes compared to primary strokes.
Conclusion
This systematic review is an update and summary of the available literature on stroke recurrence within sub-Saharan Africa. Further studies are warranted to assess the outcomes and burden of stroke recurrence in SSA.
Introduction
Stroke remained a leading cause of death and ranked the second most common disease worldwide in 2019.Citation1 Most literature indicates that modifiable risk factors such as hypertension, dyslipidemia, diabetes, cardiac disorders, sickle cell disease, high fat diet, sleep apnea, obesity, tobacco smoking, migraines, alcohol and drug abuse, oral contraceptive use, and lack of exercise are responsible for majority of the strokes.Citation2–4
In 2011, a global meta-analysis estimated that 11% of individuals will have a recurrence within a year of their first stroke and 26% within 5 years.Citation5 Secondary stroke prevention measures such as antithrombotic, statin, and antihypertensive therapies can reduce the risk of secondary vascular events by 20% to 30%.Citation6–9
Recent studies show that nearly 30% of strokes are recurrent events, and these recurrent strokes are more likely to result in disability or death.Citation10 In addition to premature mortality, recurrent strokes are associated with physical and cognitive disability and significant social and financial impact. In particular, patients with lacunar infarcts are 4 to 12 times more likely to be diagnosed with dementia than the average population, with recurrent lacunar strokes causing subcortical dementiaCitation11,Citation12 and cardioembolic stroke is the most important predictor of mortality.Citation13
Generally, the predictive and significant risk factors of stroke are well known.Citation3,Citation14 However, in Sub-Saharan Africa (SSA), risk factors for stroke recurrence are less well understood.Citation15 Studies indicate that sub-Saharan Africa has high indices of stroke burden compared to the rest of the world.Citation16–18 Estimations of the annual incidence rate of up to 316 per 100,000, with a prevalence of up to 1,460 per 100,000 and a 3-year fatality rate greater than 80%, have been made over the past decade in SSA.Citation16,Citation18–20 The majority of these strokes occur within the fourth to sixth decades of life, leading to severe family and societal implications as this impacts the socioeconomic productivity of individuals in SSA.
Understanding relevant risk factors of stroke recurrence among individuals from SSA may help develop strategies and interventions to address this burden. The aim of this systematic literature review was to identify stroke recurrence rates and risk factors for recurrent strokes identified in studies conducted in SSA over the last two decades. Findings have the potential to inform care approaches and health policy decisions.
Materials and Methods
Our investigations targeted two foci, all focused on manuscripts published from 2000 to April 2022 to ensure contemporary relevance: 1) a survey of original reports on stroke recurrence rate with emphasis from ONLY sub-Saharan Africa and 2) focus on original reports that addressed both stroke recurrence rates AND risk factors or if they included either recurrent rates or risk factors of stroke recurrence in SSA.
Literature Review and Search Strategy
Using the PICO guidelines, we set out to answer the study question below; What are the reported recurrent stroke rates and their risk factors among adults within sub-Saharan Africa?
PubMed, EMBASE, WHO Africa-African Index Medicus and Google Scholar were systematically searched for relevant articles. Gray literature sources such as ProQuest and conference registries were also searched to identify unpublished relevant articles. Reference lists of eligible studies were manually searched for additional unindexed pertinent references. The search was limited to human studies that were published from January 2000 until April 2022. Articles published in English language were considered.
Search terms used were stroke*stroke recurrence*stroke risk factors*stroke incidence*Africa*and sub-Saharan Africa; (*) was used as a wildcard to include several forms of the terms. A second search was done using EMBASE using the keywords; (“stroke recurrence” [MeSH Terms] OR “stroke recurrence rates” [All Fields]) AND (“incidence” [MeSH Terms] OR (“prevalence” [All Fields] AND “risk factors” [All Fields]) OR “stroke risk factors” [All Fields] AND (“Africa” [MeSH Terms] OR “Africa” [All Fields]).
Critical Appraisal and Assessment of Bias
All authors considered the risk of bias in the individual studies and across studies during full text reading using the Critical Appraisal Skills Program (CASP) checklist for observational studies. See Table S1 for the che cklist and Table S2 for the critical appraisal.
Inclusion and Exclusion Criteria Considered for Selection of Studies
The search was intended to determine the distribution of research studies on stroke recurrence and risk factors in sub-Saharan Africa.Citation21 Inclusion criteria were: 1) observational or experimental studies on stroke recurrence and risk factors, original research (randomized controlled trials, prospective non-randomized controlled and uncontrolled interventional studies), and publications in English.
A reference search of reviews on stroke recurrence and risk factors from SSA was used to identify additional studies potentially missed in the initial search. We excluded articles that were case reports, other literature reviews, stroke attributed to sickle cell disease and other hematological abnormalities and COVID-19, and stroke recurrence reports in children from sub-Saharan Africa.
Selection of Publications
All abstracts were prescreened for relevance by one reviewer (SNM) based on title and abstract information. Abstracts were then assessed by a three-member review team (SNM, M.K., MNK) to ensure consistent application of inclusion and exclusion criteria. Discrepancies were discussed until a consensus was reached. Once the inclusion and exclusion criteria were finalized, all abstracts were reviewed by two independent reviewers (SNM, MK) to determine suitability for further in-depth review.
Data Collection, Synthesis, and Reporting
Reviewers used a structured data extraction form modelled on other systematic reviews and recommendations.Citation22,Citation23 Reports were also assessed to see whether they included 1) stroke recurrence rates, 2) risk factors, and 3) a focus on adults.
Results
Search Findings
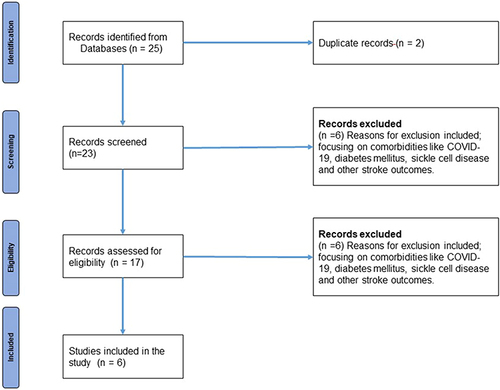
A total of 25 records were identified from the search of databases and indexing services. Accordingly, 19 studies were retrieved in PubMed/Medline, four from WHO Africa–African Index Medicus, and two were retrieved in Google Scholar databases. Two duplicates were removed, and titles and abstracts screened 21 articles. From this, six articles were excluded, and the retained 17 full-text articles were assessed for eligibility. Out of this, six articles were excluded for reasons such as lack of relevance and no stroke recurrence rates, and six studies were included for the final analysis ().
Figure 1 Papers screened.
Study Characteristics
The six studies included in the systematic review had 6285 participants. Out of these, a total of 3481 (55.4%) patients are reported to have suffered an initial ischemic stroke, while 1679 (26.7%) patients had a hemorrhagic stroke, while the rest were unclassified. The sample size of the included studies ranged from 100 to 3553.Citation24–29 Of the total studies, the majority (5 studies) were conducted in Western Africa, with half coming from Cameroon.Citation27–29 shows the summary of the articles included in the review.
Table 1 Summary of the Articles Included in the Review
Quality of Studies
All the studies included were either prospective observational cohort studies (2 studies), retrospective registry studies (2 studies) or case–control studies (3 studies). One study had an initial retrospective part and a cross-sectional part. The mean age at index stroke ranged from 29.6 to 66.5 years. The adapted Newcastle–Ottawa Scale (NOS) ratings for three studies ranged from a low of 6 to a high of 8. One study had a sample size of only 100,Citation27 two studies had between 200 and 300 study participants,Citation18,Citation24 and the rest had more than 500 study participants.Citation25,Citation28
The Reported Prevalence of Stroke Recurrence
The reported prevalence of stroke recurrence in the studies was 14.2%, 14.5% and 25% in studies conducted in Cameroon by Mbonda et al, Lekoubou et al and Kamgang, respectively.Citation27–29 In a study from Burkina Faso by Dabilgou et al, forty-four patients were hospitalized due to recurrent stroke of which 13.9% were admitted for a second stroke, while 2.6% were admitted for a third stroke.Citation24 While in Ghana and Nigeria, 9.4% had recurrent strokes,Citation25 and in a community study in Tanzania, 1.99% had stroke recurrence.Citation18
The mean interval between the index and second stroke was 24±24.34 months (3 months – 10 years); 1–2 years in 37.8%, >3 years in 28.4% and 14.9% within six months; 16.0 months (95% CI = 3.36–28.64).Citation24 Most of the patients had their strokes after 12 months.Citation24
Recurrent Stroke According to Subtypes
In all the reported studies, stroke diagnosis was based on clinical evaluation and brain C.T. neuroimaging. The etiological subtypes of strokes were defined using the A-S-C-O-D classification as A – Atherosclerosis, S – Small vessel occlusion, C-cardiac pathology, O – Other causes and D – dissection.Citation30 One study utilized the ASCOD classification for ischemic strokes,Citation29 while another used both the ASCOD classification for ischemic strokes, and Structural, Medication-related, Amyloid angiopathy, Systemic/other diseases, Hypertension and Undetermined causes (SMASH-U) was used for hemorrhagic strokes.Citation25,Citation31 Ischemic strokes were the commonest in all studies, ranging from 43.6% to 81%, while 9% to 20.1% were hemorrhagic; one study reported that 40.7% were unclassified.Citation28 Most ischemic strokes were within the MCA territory, while most hemorrhagic strokes were in the temporal-parietal region.
Risk Factors and Predictors for Stroke Recurrence
Risk factors associated with stroke recurrence were reported in 5 studies.Citation24,Citation25,Citation27–29 Four studies reported using odds ratios for some known risk factors,Citation25–27,Citation29 while 2 reported with percentages.Citation24,Citation28 See showing weighted risk factors for stroke recurrence in SSA. A history of hypertension or untreated hypertension was the most common vascular risk factor for recurrent strokes, ranging from 81.8%; to 90.7% in all the studies except for one study which described stroke risk factors for incident strokes. Stroke recurrence was also associated with current alcohol consumption in 3 studies, ranging between 10.51% and 45.5%. The other two studies did not report alcohol consumption among recurrent stroke patients. Three studies reported that patients with recurrent strokes were less likely to consume tobacco or smoke than those with incident strokes. None of the studies reported that tobacco smoking or consumption was associated with recurrent strokes.
Table 2 Weighted Risk Factors for Stroke Recurrence in SSA Studies. Odds Ratio; 95% (Confidence Interval)
Diabetes mellitus was associated with recurrent strokes in two studies,Citation25,Citation28 while three studies reported that diabetes mellitus was not associated with stroke recurrence.Citation24,Citation27,Citation29 Though one study noted that casual blood glucose was statistically associated with recurrence.Citation27
Other factors reported as independent factors for stroke recurrence were female sex and non-compliance with therapy after the first stroke, right-handedness, congestive heart disease, gout, facial palsy, dysarthria andCitation27 dyslipidemia;Citation25,Citation29 however, one study noted no associations with medication adherence to various risk factors.Citation27
One study reported congestive heart failure OR, 3.45 95% CI = 1.16–10.28; gout OR, 4.44; 95% CI = 1.09–18.09; dyslipidemia adj OR, 2.78; 95% CI = 1.25–6.18; family history of CVD adj OR, 2.1; 95% CI = 1.1–4.2 as risk factors for recurrent strokes.Citation27 Another study reported older age as a risk factor; patients with recurrent strokes were older, with a median age of 65.0 years.Citation28 Atrial fibrillation (A.F.) was also reported as an independent risk factor for stroke recurrence.Citation28
Stroke Mortality Among Stroke Recurrence Patients
Stroke mortality is reported in three studies ranging from 20.5% to 23%.Citation25,Citation28,Citation29 In general, mortality was higher for patients with recurrent stroke than those with incident strokes in these studies. Akpalu et al reported an in-patient mortality of 20.5% among those with recurrent strokes compared to 21.4% of those with first-time strokes.Citation25 Lekoubou et al reported that 14.5% of participants with recurrent stroke died and stroke recurrence increased the risk of death by 43% after adjustment for age, sex, and residency.Citation28 The known risk factors such as diabetes, history of hypertension, Glasgow coma scale and time to admission did not alter the association. In this study, the in-hospital mortality rate was 20.6%, which was higher than that of participants with first-ever stroke (19.6%). Mbonda et al reported a 23% death rate among those with stroke recurrence;Citation29 other studies did not report mortality rates.Citation18,Citation24,Citation27
Discussion
This review had three significant findings: (1) Stroke recurrence rates are high within sub-Saharan Africa; (2) the known stroke risk factors remain the main associated factors for stroke recurrence; (3) mortality associated with stroke recurrence is high compared to primary strokes.
This review found that hypertension, current alcohol consumption, diabetes mellitus, female gender, non-adherent to treatment after incident stroke, and cardiac causes (congestive heart failure and atrial fibrillation) were independent risk factors of recurrent stroke. These findings are similar to the conclusions drawn from the INTERSTROKE study, which was a landmark case–control study which confirmed that nine modifiable risk factors account for nearly 90% of the population’s attributable risk for stroke in all regions of the world, including SSA such as hypertension, diabetes mellitus, poor diet, physical inactivity, unfavorable psychosocial factors, alcohol abuse and cardiac diseases.Citation3
Of the top 4 risk factors for stroke identified in this sample of studies, 3 are potentially modifiable, hypertension, medication non-adherence and alcohol use. Hypertension is a major modifiable driver of the stroke burden and recurrent strokes in SSA. Nearly half of the people in Africa aged 25 years and above are estimated to be hypertensive, which constitutes the highest burden of hypertension in the world, according to the WHO, and about half were not receiving treatment after diagnosis.Citation29
Adherence to medications that can reduce stroke recurrence has potential to reduce stroke recurrent. Lack of adherence to medications for hypertension and regularly attending stroke follow-up clinics have been reported to lead to high levels of uncontrolled blood pressure levels in stroke survivors.Citation29 Reasons for non-adherence reported are lack of knowledge about hypertension being a chronic condition, costs for medications and lack of physical assistance to reach health care facilities and alcohol abuse.Citation32,Citation33 Poor knowledge among stroke survivors has been reported; nearly 42% of the stroke survivors or their caretakers in one study were unaware that stroke could recur.Citation34 This lack of knowledge leads to delays in timely health-seeking in stroke recurrences and adherence to medications. The utilization of recurrent stroke prophylaxis and adherence to statins, antiplatelets, antihypertensives, attendance to follow up clinics and physiotherapy services have been reported. Patient and caregiver education needs to be emphasized, including counselling stroke patients and their caretakers on adverse outcomes of stroke-like recurrence and death.
Use of substances is another potentially modifiable factor in recurrent stroke risk. Alcohol usage among stroke survivors was reported to be associated with stroke recurrence in three studies. Earlier studies from high-income countries reported that nearly half of stroke survivors with a history of heavy alcohol use had a recurrent brain infarction within 5 years compared with 22% of those without heavy alcohol use.Citation35,Citation36 However, this may be due to incident stroke survivors who use/abused alcohol before their strokes ceasing drinking alcohol after developing a debilitating disease. In contrast, for others, stroke could have been associated with mental health issues like depression that precipitated increased alcohol consumption and stroke recurrences. Few studies have explored the role of alcohol and stroke recurrences in sub-Saharan Africa.
Two studies have reported that diabetes mellitus was associated with recurrent stroke, while one reported casual high blood sugar levels.Citation25,Citation27,Citation28 This is consistent with these studies from elsewhere which have reported a significant association between diabetes mellitus and stroke recurrence.Citation37,Citation38
Limitations
While this systematic review provides an update on available data on recurrent strokes in sub-Saharan Africa, we note possible limitations in our review. First, we may be subject to publication bias as only the electronic databases and references were considered for this review. Secondly, other limitations pertain to the quality of the evidence provided by the included studies. Thirdly, most of the publications were conducted from single hospital studies in urban centers; therefore, generalizability to rural settings or whole countries may be limited. Therefore, national, or regional prospective observational studies on stroke recurrence in sub-Saharan African countries are still needed. Three of the studies (half our article sample) were from Cameroon, a west African country and the preponderance of data from a single country might skew the findings. The lack of data from many African countries is also a limitation and highlights the urgent need to establish systems of routine and reliable data monitoring across this continent. Another limitation was the selection bias as we included only papers in English language.
Conclusion
This systematic review is an update and summary of the available literature on stroke recurrence within sub-Saharan Africa. Stroke recurrence and mortality rates remain unacceptably high among stroke survivors in sub-Saharan Africa. Further studies are warranted to assess the outcomes and burden of stroke recurrence and escalation of secondary prevention measures in SSA.
Disclosure
Professor Martha Sajatovic reports grants from Merck, Otsuka, Alkermes, International Society for Bipolar Disorders (ISBD), National Institutes of Health (NIH), Centers for Disease Control and Prevention (CDC), Patient-Centered Outcomes Research Institute (PCORI); personal fees from Alkermes, Otsuka, Janssen, Lundbeck, Teva, Neurelis; royalties from Springer Press, Johns Hopkins University Press, Oxford Press, UpToDate; compensation for preparation of/participation in continuing medical education activities from American Physician’s Institute (CMEtoGo), Psychopharmacology Institute, American Epilepsy Society, Clinical Care Options, American Academy of Child and Adolescent Psychiatry, Neurocrine, outside the submitted work. The authors report no other conflicts of interest in this work.
Acknowledgment
Research reported in this publication was supported by the National Institute of Neurological Disorders and Stroke of the National Institutes of Health under Award Number R01NS118544. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.” Prior to issuing a press release concerning the outcome of this research, please notify the NIH awarding I.C. in advance to allow for coordination.
References
- World Health Organisation. The top 10 causes of death; 2020.
- Fm OMAAA, Ogbera AO, Laarje A. Dyslipidaemia as a risk factor in the occurrence of stroke in Nigeria: prevalence and patterns. Pan Afr Med J. 2016;25:75. doi:10.11604/pamj.2016.25.75.8797
- O’Donnell MJ, Chin SL, Rangarajan S, et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): a case-control study. Lancet. 2016;388(10046):761–775. doi:10.1016/S0140-6736(16)30506-2
- Maredza M, Bertram MY, Gomez-Olive XF, Tollman SM. Burden of stroke attributable to selected lifestyle risk factors in rural South Africa. BMC Public Health. 2016;16(1):143. doi:10.1186/s12889-016-2805-7
- Mohan KM, Wolfe CD, Rudd AG, Heuschmann PU, Kolominsky-Rabas PL, Grieve AP. Risk and cumulative risk of stroke recurrence: a systematic review and meta-analysis. Stroke. 2011;42(5):1489–1494.
- Collaboration AT; Antithrombotic Trialists’ Collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. J Bmj. 2002;324(7329):71–86. doi:10.1136/bmj.324.7329.71
- Lakhan SE, Sapko MT. Blood pressure lowering treatment for preventing stroke recurrence: a systematic review and meta-analysis. Int Arch Med. 2009;2(1):30. doi:10.1186/1755-7682-2-30
- Sandercock PA, Counsell C, Kane EJ. Anticoagulants for acute ischaemic stroke. Cochrane Database Syst Rev. 2015;2015(3):CD000024. doi:10.1002/14651858.CD000024.pub4
- Ni Chroinin D, Asplund K, Asberg S, et al. Statin therapy and outcome after ischemic stroke: systematic review and meta-analysis of observational studies and randomized trials. Stroke. 2013;44(2):448–456. doi:10.1161/STROKEAHA.112.668277
- Sacco RL, Kasner SE, Broderick JP, et al. An updated definition of stroke for the 21st century: a statement for healthcare professionals from the American heart association/American stroke association. Stroke. 2013;44(7):2064–2089. doi:10.1161/STR.0b013e318296aeca
- Arboix A, Massons J, Garcia-Eroles L, et al. Nineteen-year trends in risk factors, clinical characteristics and prognosis in lacunar infarcts. Neuroepidemiology. 2010;35(3):231–236. doi:10.1159/000319460
- Loeb C, Gandolfo C, Croce R, Conti M. Dementia associated with lacunar infarction. Stroke. 1992;23(9):1225–1229. doi:10.1161/01.STR.23.9.1225
- Arboix A, Oliveres M, Massons J, Pujades R, Garcia-Eroles L. Early differentiation of cardioembolic from atherothrombotic cerebral infarction: a multivariate analysis. Eur J Neurol. 1999;6(6):677–683. doi:10.1046/j.1468-1331.1999.660677.x
- Feigin VL, Forouzanfar MH, Krishnamurthi R, et al. Global and regional burden of stroke during 1990–2010: findings from the global burden of disease study. Lancet. 2014;383(9913):245–254. doi:10.1016/S0140-6736(13)61953-4
- Adoukonou T, Kossi O, Fotso Mefo P, et al. Stroke case fatality in sub-Saharan Africa: systematic review and meta-analysis. Int J Stroke. 2021;16(8):902–916. doi:10.1177/1747493021990945
- Owolabi MO, Akarolo-Anthony S, Akinyemi R, et al. The burden of stroke in Africa: a glance at the present and a glimpse into the future. Cardiovasc J Afr. 2015;26(2 Suppl 1):S27–38. doi:10.5830/CVJA-2015-038
- Akinyemi RO, Owolabi MO, Ihara M, et al. Stroke, cerebrovascular diseases and vascular cognitive impairment in Africa. Brain Res Bull. 2019;145:97–108. doi:10.1016/j.brainresbull.2018.05.018
- Walker R, Whiting D, Unwin N, et al. Stroke incidence in rural and urban Tanzania: a prospective, community-based study. Lancet Neurol. 2010;9(8):786–792. doi:10.1016/S1474-4422(10)70144-7
- Lekoubou A, Nkoke C, Dzudie A, Kengne AP. Stroke admission and case-fatality in an urban medical unit in sub-Saharan Africa: a fourteen year trend study from 1999 to 2012. J Neurol Sci. 2015;350(1–2):24–32. doi:10.1016/j.jns.2015.02.002
- Akinyemi RO, Ovbiagele B, Adeniji OA, et al. Stroke in Africa: profile, progress, prospects and priorities. Nat Rev Neurol. 2021;17(10):634–656. doi:10.1038/s41582-021-00542-4
- None N. Sub-Saharan Africa. Glob Heart. 2018;13(3):171–175. doi:10.1016/j.gheart.2018.09.514
- Furlan AD, Malmivaara A, Chou R, et al. Updated method guideline for systematic reviews in the Cochrane back and neck group. Spine. 2015;40(21):1660–1673. doi:10.1097/BRS.0000000000001061
- Li T, Vedula SS, Hadar N, Parkin C, Lau J, Dickersin K. Innovations in data collection, management, and archiving for systematic reviews. Ann Intern Med. 2015;162(4):287–294. doi:10.7326/M14-1603
- Dabilgou AA, Drave A, Kyelem JMA, et al. Frequency of recurrent stroke in Burkina Faso: an observational hospital based study of 6 months. Pan Afr Med J. 2021;40:108. doi:10.11604/pamj.2021.40.108.23098
- Akpalu A, Sarfo FS, Akinyemi J, et al. Frequency & factors associated with recurrent stroke in Ghana and Nigeria. J Neurol Sci. 2022;439:120303. doi:10.1016/j.jns.2022.120303
- Walker RW, Jusabani A, Aris E, et al. Stroke risk factors in an incident population in urban and rural Tanzania: a prospective, community-based, case-control study. Lancet Glob Health. 2013;1(5):e282–8. doi:10.1016/S2214-109X(13)70068-8
- Kamgang J, Tetinou F, Zolo Y, et al. Recurrent ischemic and hemorrhagic stroke in Cameroon: a case-control study. Neurol Res Int. 2021;2021:9948990. doi:10.1155/2021/9948990
- Lekoubou A, Nkoke C, Dzudie A, Kengne AP. Recurrent stroke and early mortality in an urban medical unit in Cameroon. J Stroke Cerebrovasc Dis. 2017;26(8):1689–1694. doi:10.1016/j.jstrokecerebrovasdis.2017.03.031
- Mbonda PC, Mafo D, Doumbe J, Kuate C. Recurrence of strokes and associated factors at laquintinie hospital in douala. Clinical Neur Neuro sci. 2021;5:3. doi:10.11648/j.cnn.20210503.12
- Amarenco P, Bogousslavsky J, Caplan LR, Donnan GA, Wolf ME, Hennerici MG. The ASCOD phenotyping of ischemic stroke (Updated ASCO Phenotyping). Cerebrovasc Dis. 2013;36(1):1–5. doi:10.1159/000352050
- Meretoja A, Strbian D, Putaala J, et al. SMASH-U: a proposal for etiologic classification of intracerebral hemorrhage. Stroke. 2012;43(10):2592–2597. doi:10.1161/STROKEAHA.112.661603
- Thorogood M, Connor M, Lewando-Hundt G, Tollman S, Ngoma B. Team SPJBotWHO. Secon Preven Stroke. 2004;82(7):503.
- Wasserman S, De Villiers L, Ajsamj B. Community-based care of stroke patients in a rural African setting. South Afric Med J. 2009;99(8):579–583.
- Tessua KK, Munseri P, SSJPo M. Outcomes within a year following first ever stroke in Tanzania. PLoS One. 2021;16(2):e0246492. doi:10.1371/journal.pone.0246492
- Sacco RL, Shi T, Zamanillo MC, Kargman DE. Predictors of mortality and recurrence after hospitalized cerebral infarction in an urban community: the Northern Manhattan Stroke Study. Neurology. 1994;44(4):626–634. doi:10.1212/WNL.44.4.626
- Han J, Mao W, Ni J, et al. Rate and determinants of recurrence at 1 year and 5 years after stroke in a low-income population in rural China. Front Neurol. 2020;11:2. doi:10.3389/fneur.2020.00002
- Kissela BM, Khoury J, Kleindorfer D, et al. Epidemiology of ischemic stroke in patients with diabetes: the greater Cincinnati/Northern Kentucky Stroke Study. Diabetes Care. 2005;28(2):355–359. doi:10.2337/diacare.28.2.355
- Callahan A. Risk of stroke and cardiovascular events after ischemic stroke or transient ischemic attack in patients with type 2 diabetes or metabolic syndrome: secondary analysis of the stroke prevention by aggressive reduction in cholesterol levels (SPARCL) trial. Arch Neurol. 2011;68(10):1245–1251. doi:10.1001/archneurol.2011.146