
Abstract
Background
Multiple sclerosis (MS) is a disease of the nervous system that has profound effects on everyday functioning and quality of life of not only the person who is diagnosed, but also her/his family and acquaintances. Despite this, the uncertainties of the actual etiological basis of MS make it difficult to reach a conclusive statement about the optimal therapeutic management of the disease, which may differ depending on the given case and phase of illness. This has led to an interest in potential novel therapeutic avenues, including percutaneous transluminal angioplasty (PTA). Yet, evidence in support of PTA in the management of MS is scarce and contradictory. The aim of the present study was to provide a preliminary assessment as to whether PTA may impact subjective quality of life and cognitive functioning in severe MS.
Method
Ninety-five MS outpatients were followed-up for 24 months on a scheduled basis using the Milan Overall Dementia Assessment and the short-form 36-item scales, and were clinically evaluated by an appointed neurologist and psychiatrist.
Results
At end point (month 24), only a minority of patients were still active in the study (n=33 or 34.74%). Among other measures, those who remained in the study until completion showed a significantly better Expanded Disability Status Scale and Milan Overall Dementia Assessment autonomy profile at study entrance compared to those patients who did not remain in the study until completion. Limitations were: a lack of any active control group; small sample size; Berkson’s bias; and selection by indication biases.
Conclusion
Given the burden of MS and its high attrition rate, additional studies, including bigger samples, active control groups, and Cox’s regression and survival analysis in case of randomization, should shed further light on the actual usefulness of PTA for the most severe cases of MS.
Introduction
Multiple sclerosis (MS) is a severe, chronic, and often debilitating disease affecting the central nervous system (CNS), leading to damage of the myelin sheath resulting in a progressive alteration of neuronal transmission. Despite the intense research efforts made within the past decades, the etiology and optimal therapeutic intervention for MS are far from achieving a satisfactory understanding.Citation1,Citation2 MS symptoms depend upon the involvement of multiple central nervous system areas, which accounts for intra- and interindividual variability of the clinical pictures and therapeutic outcomes. Specifically, besides the motor and sensory impairments, cognitive impairments (memory, concentration, judgment, and reasoning skills) significantly affect the critical thinking and judgment abilities as well as the willingness of the sufferer to accept his/her own condition, which, in turn, significantly affects willingness to seek (additional) medical support and/or to adhere to chronic treatment plans, especially in cases of invasive surgical procedures.Citation3,Citation4 Concerning MS etiopathogenesis, self-immunity is undoubtedly a core mechanism in the disease.Citation5 Yet, the potential involvement of chronic cerebrospinal venous insufficiency (CCSVI) in MS has also been identified, albeit by a restricted number of clinicians, and represents a matter of vivid debate.Citation6,Citation7 Authors advocating a causative relationship between MS and CCSVI propose that, at least in some MS subjects at more advanced clinical stages of the disease, CCSVI may contribute to a reflux and cerebral venous stasis, leading to reduction of oxygen levels as well as neuronal and tissue damage that are thought to determine the harmful reaction of the immune system towards the body.Citation8 Ideally, based on this hypothesis, jugular vein percutaneous transluminal angioplasty (PTA) for the management of CCSVICitation9,Citation10 should enhance the psychological functioning and subjective perception of quality of life (QoL) in MS patients.
Therefore, the aim of the present study was to assess the perception of QoL in MS patients before and after PTA intervention within a 24-month follow-up in relation to neurocognitive functioning.
Materials and methods
Study participants
One hundred and two Italian Caucasian MS patients of both sexes aged 18–75 years with an education level of ≥12th grade (high school diploma or higher) were referred to our outpatient facility by their own clinical neurologists (74% from Sardinia, 11% from Emilia-Romagna, 6% from Sicily; 9% from elsewhere). Disability due to MS was evaluated according to the Expanded Disability Status Scale (EDSS) scoreCitation11 by a clinical neurologist. Patients providing a valid informed consent for this study were screened and followed-up at the SC Transplant and Vascular Surgery Unit of the University of Catania, Italy between July 2011 and April 2014 after procedures had been fully explained by the reference surgeon and the psychiatrists involved in this longitudinal study. The local ethical committee approved study procedures in accordance to the Ethical Principles for Medical Research Involving Human Subjects indicated by the 2004 World Medical Association Declaration of Helsinki.Citation12 The cognitive functioning and subjective perception of QoL by the patients were assessed by means of the Milan Overall Dementia Assessment (MODA) – including a specific scoring for MSCitation13 – and the short-form 36-item (SF-36),Citation14 respectively. A liaison psychiatrist (CDP) with an extensive experience with MS patients ruled out any axis II or axis I psychiatric diagnosis. Any concomitant medications (for any reason) – including recent use (<1 month prior) of immunosuppressant drugs or illegal substance use, presence of any relevant medical comorbidity, or refusal to provide a valid informed consent – were considered as exclusion criteria.
Neuropsychological functioning and QoL assessment
The EDSS steps 1.0–4.5 refer to people with MS who are fully ambulatory. EDSS steps 5.0–9.5 indicate impairment to ambulation. The EDSS could range from zero (normal neurological exam) to ten (dead due to MS).
The MODA includes three sections: the first section (score range: 0–35) tests temporal, spatial orientation, and personal semantic memory (eg, date and place of birth, personal address); the second section (range: 0–15) covers the degree of autonomy of the patient; and the third section (range: 0–50) examines cognitive abilities (attention, verbal intelligence, verbal memory, language, visual–perceptual abilities, and constructional apraxia). Each section has its own score; the grand score (range: 0–100) is the sum of the partial scores adjusted for age and educational level. Higher scores on the MODA indicate better functioning.
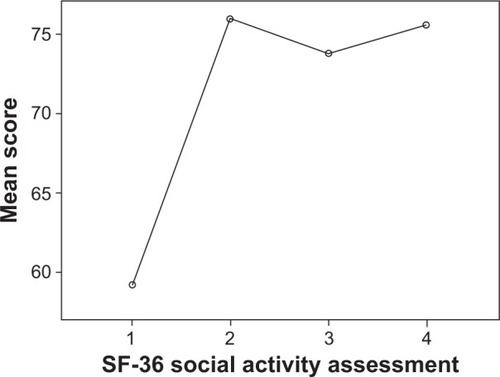
Both the MODA and the SF-36 (which detects three different indices related to the health and psychological–emotional status through investigation of physical activity, physical role, physical pain, global well-being, vitality, social activities, emotional role, and mental status) were submitted before PTA intervention and 6, 12, and 24 months thereafter. Higher scores on the SF-36 also indicate a better level of subjective well-being. For additional information about the PTA procedure, please refer to Schaller.Citation15
Statistical analysis
The Kolmogorov–Smirnov test ascertained normal distribution of data. Parametric tests included χ2, independent samples t-test for baseline comparisons among those going to complete the study at month 24 versus those dropping out earlier (either at month 6 or month 12 for any reasons), and one-way repeated measure analysis of variance (using the Mauchly’s test to assess the assumption of sphericity). Pearson’s R correlation test and binary logistic regression regarded only clinically suggestive selected measures. Finally, all comparisons were two-tailed.
Results
Baseline demographic and clinical features
Of the 102 outpatients screened, 95 provided a valid informed consent to participate in the study; five patients did not attend the baseline appointment, while two patients/their legal guardians refused to sign the informed consent. Baseline patients included 58 (61.1%) females and 37 (38.9%) males. Mean age of the patients at presentation was 44.60±10.48 (range 20–70) years; patient-declared age at MS diagnosis was 30.79±9.33 (range: 10–60) years; mean years lapsed since MS diagnosis was 12.84±8.62 (range: 1–40) years; and average education level was 11.71±3.21 (range: 5–19) years. Mean EDSS score at study entrance was 5.10±2.18 (range 1–8), indicating a severe MS condition on average.
Dropouts across the study were as follows: at month 6, n=11 (11.58%); at month 12, n=34 (35.79%); and at month 24 (study endpoint), n=17 (17.9%). Cumulative dropouts within the study were as much as n=62 (65.26%), or study completers, n=33 (34.74%). Higher EDSS score at study entrance correctly predicted attrition, with a relevant binary logistic regression model correctly classifying 21 out of 33 (69%) of study completers (Exp(B) =0.753; P=0.011). provides a detailed comparison of baseline demographic and clinical features between study completers (endpoint =24 months) versus non-completers.
Table 1 Baseline clinical features of study completers versus non-completers at 24-month follow-up
Neurocognitive functioning and subjective QoL
Selected Pearson’s correlations (P≤0.005 or P≤0.001) included the following: MODA total score at baseline and EDSS score (R=−0.292); months 6–12–24 MODA total scores and reference EDSS score, P=ns (not significant); and years elapsed since MS diagnosis and EDSS score (R=0.288). Neuropsychological functioning assessed with MODA correlated with physical activity measured by the SF-36 at baseline (R=0.339), month 6 (R=0.275), month 12 (R=0.412), and month 24 (R=0.47). Neuropsychological functioning also correlated with mental health (as measured by SF-36) at baseline (R=0.34), month 6 (R=0.233), month 12 (R=0.427), and month 24 (R=0.628). Neuropsychological functioning significantly correlated with social activity (as measured by SF-36) at month 24 (R=0.455) but not at month 6 or 12, as it was for somatic pain perception (as measured by SF-36) at month 24, R=0.385, but not at baseline, month 6 or 12. Interestingly, neuropsychological functioning assessed with MODA showed a trend of increasingly significant correlation coefficients with attention and prose memory (MODA’s domains) across different times of evaluation (respectively: baseline, R=0.360 and R=0.638; month 6, R=0.280 and R=0.620; month 12, R=0.422 and R=0.699; month 24, R=0.643 and R=ns). One-way repeated measures analysis of variance for selected MODA and SF-36 measures have been reported in –.
Figure 1 MODA neuropsychological functioning test trend in patients followed-up for 24 months (four observations).
Abbreviations: MODA, Milan Overall Dementia Assessment; PTA, percutaneous transluminal angioplasty.
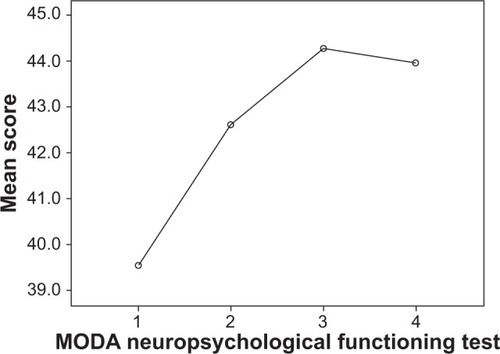
Figure 2 MODA attention test trend in patients followed-up for 24 months (four observations).
Abbreviations: MODA, Milan Overall Dementia Assessment; PTA, percutaneous transluminal angioplasty.
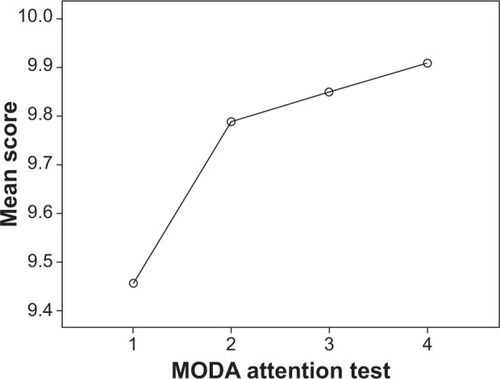
Figure 3 MODA prose memory test trend in patients followed-up for 24 months (four observations).
Abbreviations: MODA, Milan Overall Dementia Assessment; PTA, percutaneous transluminal angioplasty.
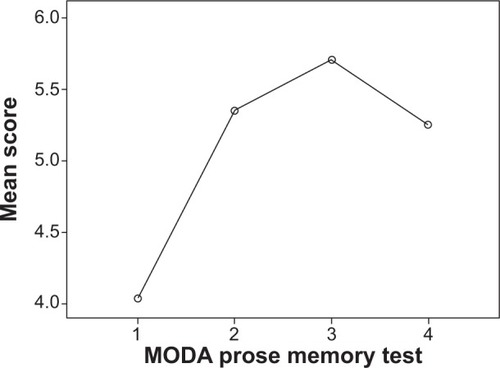
Figure 4 MODA autonomy test trend in patients followed-up for 24 months (four observations).
Abbreviations: MODA, Milan Overall Dementia Assessment; PTA, percutaneous transluminal angioplasty.
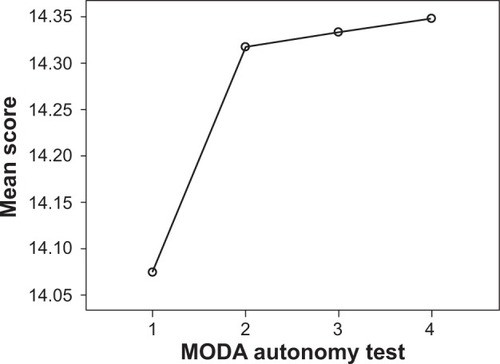
Figure 5 SF-36 physical activity assessment trend in patients followed-up for 24 months (four observations).
Abbreviations: PTA, percutaneous transluminal angioplasty; SF-36, short-form 36-item.
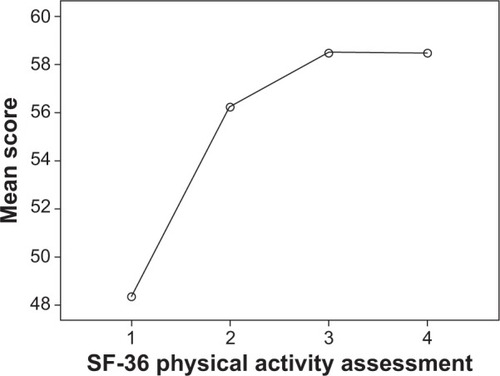
Figure 6 SF-36 somatic pain assessment trend in patients followed-up for 24 months (four observations).
Abbreviations: PTA, percutaneous transluminal angioplasty; SF-36, short-form 36-item.
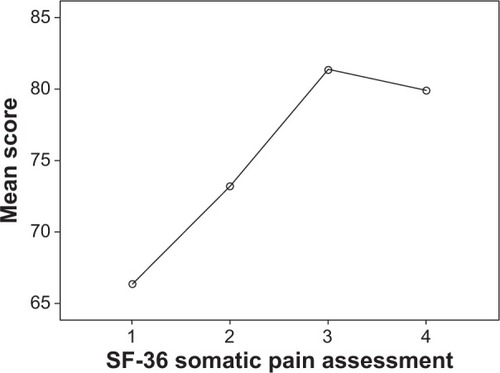
Figure 7 SF-36 mental health assessment trend in patients followed-up for 24 months (four observations).
Abbreviations: PTA, percutaneous transluminal angioplasty; SF-36, short-form 36-item.
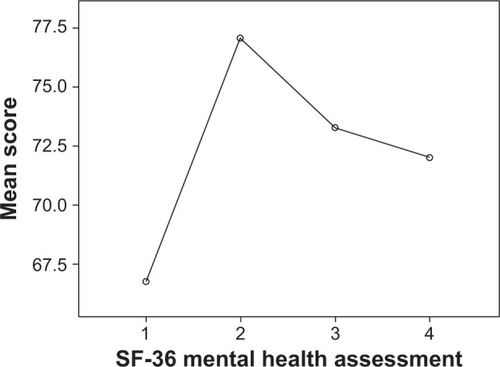
Figure 8 SF-36 social activity assessment trend in patients followed-up for 24 months (four observations).
Abbreviations: PTA, percutaneous transluminal angioplasty; SF-36, short-form 36-item.
Discussion
Overview and limitations of the study
To the best of our knowledge, this is the first explorative report including a systematic neuropsychological assessment of subjective QoL in MS outpatients undergoing PTA across a 24-month follow-up. Nonetheless, a number of limitations should be accounted for in the interpretation of the present preliminary findings.
Specifically, the sample size of the study was relatively small. Moreover, the lack of a control group is a major issue in this study, making the current results merely indicative; yet these results are serve as a prompt for additional studies, allowing for between-group(s) comparisons (eg, Cox’s regression model) or, ideally, a randomized control group on active medication(s) to be studied with survival techniques and stratification according to baseline EDSS severity score. Also, the inclusion of severe MS cases highlights the chance of a recall bias in MS patients, potentially characterized by a more pronounced cognitive decline (though the presence of caregivers as an anamnestic source should have counterbalanced this).
The present preliminary findings may suggest a beneficial effect of PTA in those severe MS cases being followed-up for 24 months. While some measures on the MODA and SF-36 tests showed a slight reduction of efficacy by month 12 to month 24, it should be acknowledged that MS is characterized by a chronic degenerative course of the disease itself. Therefore, these findings should further solicit a control group replication study on the matter. Additional issues may also be addressed, such as the possibility of selection bias due to the inclusion of more motivated and financially wealthy patients who were able to attend all the post-baseline visits, even if living far away from our facility (this issue may also contribute to an explanation of the high rate of drop-outs by month 6).
Apart from the improvement in MODA neuropsychological functioning, attention, autonomy, and prose memory tests, as well as SF-36 physical and social activities, mental health, and somatic pain (–), a suggestive finding of the present study is that physical disability (according to MODA test and the EDSS assessment) inversely correlated with cognitive disability (as assessed by MODA). Paradoxically, from the subjective perspective of the patient, a worsening of the cognitive profile may inversely correlate with perceived QoL, possibly due to a worsening of the critical judgment skills of the patient towards his/her own motor and functional autonomy.
Ultimately, since perceived QoL represents a very sensitive issue in the long-term management of most severe cases of MS with CCSVI, the presented preliminary findings should encourage more methodologically rigorous replications of studies on this topic.
Author contributions
CDP conceived the study and enrolled patients with MLP. MV, AG, and PV were involved in surgical procedures and referred patients to the outpatient psychiatric unit. MF assisted in manuscript drafting and data analysis and interpretation. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
- ZimmermannAFPizzichiniMMUpdate on etiopathogenesis of systemic sclerosisRev Bras Reumatol2013536516524 Portuguese24477730
- McCoydMUpdate on therapeutic options for multiple sclerosisNeurol Clin201331382784523896508
- MungoSFornaroMAdherence to Chronic Therapies in Psychiatry: From Treatment to Cure. The Relevance of Therapeutic RelationshipJ Psychol Psychother20133003
- DibrivnaiaKAEnikolopovaEVZubkovaIuVBoĭkoANCharacteristics of coping strategies in patients with multiple sclerosis (review)Zh Nevrol Psikhiatr Im S S Korsakova20131132 Pt 24852 Russian23675605
- HartungHPAktasOMengeTKieseierBCImmune regulation of multiple sclerosisHandb Clin Neurol201412231424507511
- MorovicSZamboniPCCSVI is associated with multiple sclerosisNeurol Res201234877077922971467
- LeoneCD AmicoECiliaSNicolettiADi PinoLPattiFCognitive impairment and “invisible symptoms” are not associated with CCSVI in MSBMC Neurol20131319723889853
- ZamboniPGaleottiRThe chronic cerebrospinal venous insufficiency syndromePhlebology201025626927921106999
- ZamboniPGaleottiRMenegattiEA prospective open-label study of endovascular treatment of chronic cerebrospinal venous insufficiencyJ Vasc Surg20095061348135819958985
- VerouxPGiaquintaAPerriconeDInternal jugular veins out flow in patients with multiple sclerosis: a catheter venography studyJ Vasc Interv Radiol201324121790179724409471
- PedersenEA rating system for neurological impairment in multiple sclerosisActa Neurol Scand Suppl196513Pt 25575585214334
- World Medical Association General AssemblyWorld Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjectsJ Int Bioethique200415112412915835069
- BrazzelliMCapitaniEDella SalaSSpinnlerHZuffiMA neuropsychological instrument adding to the description of patients with suspected cortical dementia: the Milan overall dementia assessmentJ Neurol Neurosurg Psychiatry19945712151015177798982
- ApoloneGMosconiPThe Italian SF-36 Health Survey: translation, validation and normingJ Clin Epidemiol19985111102510369817120
- SchallerBPhysiology of cerebral venous blood flow: from experimental data in animals to normal function in humansBrain Res Brain Res Rev200446324326015571768