
Abstract
Background
The Temperament Evaluation of the Memphis, Pisa, Paris, and San Diego Auto-questionnaire (TEMPS-A) is a 110-item questionnaire that assesses five affective temperaments. However, a valid shortened version is desired for large-scale investigations to enhance the compliance of respondents.
Methods
A confirmatory factor analysis was conducted among 320 psychiatric patients and 61 general adults. The participants completed the Japanese 39-item short version of the TEMPS-A, and a portion of the participants completed the 110-item version. An exploratory factor analysis with the principal factor method and varimax rotation was conducted to identify a more suitable model of the short version of the TEMPS-A.
Results
The confirmatory factor analysis revealed that the 39-item version exhibited a poor model fit. However, we found that the 18-item version exhibited a firm five-factor structure based on the exploratory factor analysis, and this model exhibited an acceptable model fit. It had good or acceptable internal consistency (Cronbach’s αs: 0.672–0.819).
Limitations
The majority of the subjects in the present study were patients, and the temperament data may have been affected by psychiatric symptoms.
Conclusion
A firm five-factor structure was not found in the 39-item short version of the Japanese TEMPS-A. Therefore, an 18-item version was proposed. This new 18-item version of the TEMPS-A might be useful for clinical applications and large-scale investigations.
Introduction
Mood disorders are subdivided into depressive and bipolar disorders. They are characterized by one or more mood episodes, depressive or (hypo)manic, and often show very long-term symptoms. In these disorders, symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.Citation1 Several affective temperaments have been considered to be antecedents or subsyndromal manifestations of mood disorders, particularly bipolar disorder.Citation2
The items of the Temperament Evaluation of the Memphis, Pisa, Paris, and San Diego Auto-questionnaire (TEMPS-A) were formulated based on the diagnostic criteria for affective temperaments and were divided into the following five groups: cyclothymic, depressive, irritable, and hyperthymic groups, based on the subscales that represent the Kraepelinian temperaments, and anxious group, based on a subscale that was developed secondarily by Akiskal et alCitation2–Citation4 and Hantouche et alCitation5 Affective temperaments have been reported to exert important pathoplastic actions on a wide range of diseases that extend far beyond the field of affective illness.Citation6 Because the cyclothymic and hyperthymic temperaments predict drug responses to lithium and antidepressants, initial evaluations of affective temperaments may be useful for selecting treatment regimens for depressed patients.Citation7 Although the original scale (110 items) of the TEMPS-A exhibited satisfactory results, the number of shortened versions that are more suitable for large-scale investigations and potentially enhance the compliance of respondents is increasing.Citation4,Citation8–Citation13
The original 39-item short version of the TEMPS-A was extracted from the full English version and developed by Akiskal et al and translated into French, Italian, and Chinese.Citation4,Citation9,Citation10,Citation13 The subscales of the full and short versions of the TEMPS-A provide unique profiles of major depressive disorder and bipolar disorder and are very useful in clinical practice, particularly for bipolar spectrum diagnoses.Citation7,Citation14–Citation16 Variants of the short version with different numbers of items have also been developed in other languages.Citation8,Citation11,Citation12 The Japanese version of the TEMPS-A was translated and validated by Matsumoto et alCitation14 and Akiyama et al.Citation17. The 39-item Japanese short version has also been used clinically, but has not yet been validated.Citation18
The five-factor structures of the English and Italian short versions of the TEMPS-A have been demonstrated by exploratory factor analysis (EFA) and confirmed by confirmatory factor analysis (CFA) in a few studies.Citation4,Citation10,Citation19,Citation20 In two CFA studies of the 39-item short TEMPS-A, the five-factor structure was confirmed, but the models did not exhibit good fits; among the goodness-of-fit indices, the root mean square errors of approximation (RMSEAs) were good, but the comparative fit indices (CFIs) were poor.Citation19,Citation20 CFA is essential for testing the goodness of fit of the expected factor structure in clinical research involving questionnaires.
This study conducted CFA of the short version (39 items) of the TEMPS-A, which was translated from English to Japanese, to confirm the expected five-factor model with structural equation modeling. We proposed a new short version of the Japanese TEMPS-A, which exhibited a good fit to the model as determined by EFA using the principal factor method, varimax rotation, and subsequent CFA.
Subjects and methods
Subjects
This research was conducted among 506 psychiatric patients and 120 general adults because the original short version of TEMPS-A was extracted in a mixed population of healthy controls and psychiatric patients.Citation4 Among the 506 patients with mental disorders, 293 new outpatients and 213 inpatients of the Department of Psychiatry of Hokkaido University Hospital were consecutively included in the study from February 2008 to March 2011 and from April 2010 to November 2013, respectively. Complete responses to the questionnaires were provided by 158 of the 293 outpatients (53.2%) and 162 of the 213 inpatients (76.1%). Of the 120 general adult volunteers, 61 subjects (50.8%) provided complete responses to the questionnaires. Overall, the investigated subjects included 320 psychiatric patients and 61 nonclinical general adults.
This study was performed according to the Declaration of Helsinki and was approved by the institutional review board of Hokkaido University Hospital. Written informed consent was obtained from all subjects.
Psychiatric evaluations
The Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) diagnoses of mental disorders in patients were made by trained psychiatrists using the Quick Reference to the Diagnostic Criteria from DSM-IV-TR, which contains the classification, diagnosis criteria, and a listing of the most important conditions to be considered in the differential diagnosis for each category; the demographic and clinical data were also recorded. The average interview duration was 60 minutes.
The nonclinical general adult volunteers completed a questionnaire to provide demographic and clinical data in addition to the TEMPS-A. None of these participants had previous histories of psychiatric disorders.
Temperament Evaluation of the Memphis, Pisa, Paris, and San Diego Auto-questionnaire
The TEMPS-A is a self-rated questionnaire consisting of 110 items (109 items for males, 110 items for females) that are rated as true (=2) or false (=1). It was designed to assess the following affective temperament dimensions: cyclothymic, depressive, irritable, hyperthymic, and anxious.Citation2 Participants completed the Japanese 39-item version, which was extracted from the Japanese standardized full version (110 items) of the TEMPS-A based on the original English short version.Citation4–Citation14 The score for each temperament subscale is the mean score on the items that comprise that subscale.
The nonclinical general adults (n=61) completed the 39-item short version of the TEMPS-A first and then completed the 110-item version of the TEMPS-A after an interval of at least 1 month.
Statistical analysis
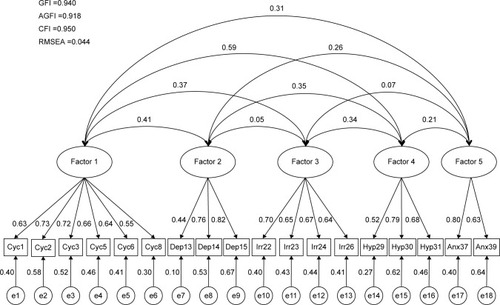
According to the original 39-item English version of the TEMPS-A, we designed a structural equation model to perform the CFA (). Each latent variable for each temperament consisted of 3–12 observed variables. We used AMOS 20.0 (SPSS Inc., Chicago, IL, USA) to perform this CFA. We performed a maximum likelihood covariance estimation to analyze the model. For the inferential statistical evaluation of the structural equation modeling, we calculated the goodness-of-fit indices, which included the goodness-of-fit index (GFI), adjusted GFI (AGFI), CFI, and RMSEA. According to the conventional criteria, a GFI greater than 0.90, an AGFI greater than 0.85, a CFI greater than 0.95, and a RMSEA less than 0.08 indicated an acceptable fit, and a GFI greater than 0.95, an AGFI greater than 0.90, a CFI greater than 0.97, and a RMSEA less than 0.05 indicated a good fit.Citation21 It is recommended that several indices should be simultaneously evaluated because the indices represent different classes of goodness-of-fit criteria.Citation21 We standardized and indicated all of the coefficients (to a maximum of 1 and a minimum of −1) for the covariance structure analysis.
Figure 1 CFA of the 39-item TEMPS-A by structural equation modeling in mental disorder patients and general adults.
A factor analysis with the principal factor method and varimax rotation was performed to evaluate the conceptual validity of the 39-item TEMPS-A and to perform the EFA.
The internal consistency of each subscale of the TEMPS-A was measured with Cronbach’s α.
Statistical analyses were performed using IBM SPSS for Windows 20 and IBM SPSS AMOS 20.0 (SPSS Inc.).
Differences were considered statistically significant at P<0.05.
Results
Demographic and clinical data
The demographic and clinical data of the subjects are shown in . Excluding the mood disorder patients, the patients’ (n=89) diagnoses consisted of nine cases of organic mood disorder, 13 cases of schizophrenia, two cases of a schizoaffective disorder, ten cases of a panic disorder, two cases of a social anxiety disorder, two cases of a pain disorder, two cases of an obsessive compulsive disorder, four cases of an eating disorder, ten cases of an adjustment disorder, eight cases of insomnia, and 27 other types of cases.
Table 1 Demographic characteristics and the 39-item TEMPS-A data of subjects
Factorial structure of the Japanese short version of the TEMPS-A
To evaluate the conceptual validity of the 39-item TEMPS-A, we performed a CFA with the five original subscales (ie, temperament scales) with AMOS 20.0. This model exhibited a poor model fit: RMSEA =0.052, GFI =0.838, AGFI =0.818, and CFI =0.809 ().
An EFA was then performed to examine the factor structure of the Japanese 39-item version of the TEMPS-A. A factor analysis with the principal factor method and varimax rotation was performed with the five original subscales. The items were assigned to each subscale if they loaded on a specific factor at greater than 0.50. The best model (), which consisted of 18 items, was extracted from the 39-item TEMPS-A. The first factor was defined by items 1, 2, 3, 5, 6, and 8 and interpreted as the cyclothymic temperament. The second factor was defined by items 29, 30, and 31 and interpreted as the hyperthymic temperament. The third factor was defined by items 13, 14, and 15 and interpreted as the depressive temperament. The fourth factor was defined by items 22, 23, 24, and 26 and interpreted as the irritable temperament. The fifth factor was defined by items 37 and 39 and interpreted as the anxious temperament.
Table 2 Principal factor analysis with varimax rotation of the 39-item TEMPS-A
Using the 18-item version of the TEMPS-A, which was statistically extracted as already described (), we performed a CFA with the five latent variables that corresponded to the temperament subscales. This model exhibited an acceptable model fit: RMSEA =0.044, GFI =0.940, AGFI =0.918, and CFI =0.950 ().
Figure 2 CFA by structural equation modeling of the 18-item TEMPS-A, which was extracted from the 39-item TEMPS-A by EFA in mental disorder patients and general adults.
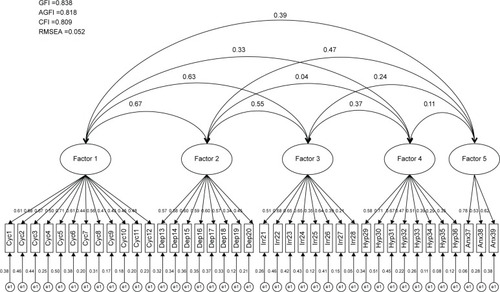
Table 3 Principal factor analysis with varimax rotation of the 39-item TEMPS-A
Internal consistency of the Japanese 18-item version of the TEMPS-A
The internal consistencies of the temperament subscales (ie, cyclothymic, depressive, irritable, hyperthymic, and anxious) of the 18-item version of the TEMPS-A were examined. The Cronbach’s αs were 0.819 for the cyclothymic, 0.697 for the depressive, 0.758 for the irritable, 0.692 for the hyperthymic, and 0.672 for the anxious temperament (). These values indicated that the Japanese 18-item version of the TEMPS-A exhibited good or acceptable internal consistency.
Table 4 Internal consistency of temperament subscales of the 18-item TEMPS-A in all subjects (N=381)
Discussion
The five-factor structure of the Japanese 39-item version of the TEMPS-A, which was extracted from the Japanese full version of the TEMPS-A, was investigated with CFA in the present study. However, due to the poor model fit, we were unable to confirm the expected five-factor structure of the 39-item version. Thus, we extracted 18 items from the 39-item version of the TEMPS-A by EFA. This 18-item version of the TEMPS-A exhibited favorable goodness-of-fit indices for the five-factor model. Thus, the results of this study indicate a limitation of the use of the 39-item Japanese version of the TEMPS-A in clinical research and practice. For these purposes, it is better to use the 18-item Japanese version of the TEMPS-A because this version has a firm five-factor structure.
The 110-item full version of the TEMPS-A has been translated into over 25 languages that have been used in clinical research and practice.Citation7,Citation22–Citation29 A shorter version of the TEMPS-A is needed for research applications with large samples for severe patients because the 110-time version of the TEMPS-A requires a long time for completion. As noted in the introduction, the short 39-item version of the TEMPS-A has been developed and reported in only four languages. Although the French and Italian versions have been reported to exhibit five-factor structures based on CFA, the goodness-of-fit levels were good in terms of the RMSEAs but insufficient in terms of the CFIs, which were below 0.95 in two studies.Citation19,Citation20 The present study also found that the RMSEAs were sufficient, but the other three indices were insufficient for explaining this five-factor structure in the 39-item Japanese version of the TEMPS-A. It is recommended that several indices that represent different classes of goodness-of-fit criteria should be simultaneously evaluated.Citation21 From this perspective, this model fits for the 39-item versions in three languages, including Japanese, were not good in terms of CFA.
By applying EFA to the Japanese short version of the 39-item TEMPS-A, we further extracted 18 items. CFA confirmed the five-factor structure of the 18-item TEMPS-A; all the four goodness-of-fit indices indicated acceptable or good fits.Citation21 Therefore, at least regarding the Japanese short versions of the TEMPS-A, the 18-item version extracted from the 39-item version is recommended for clinical and research use. Because the smallest item number of the shortened version that had been previously reported was 35 in the German version, the smaller number of 18 items reported here is attractive and promising for clinical and research use.Citation8
The limitation of this study is that the majority of the subjects of the present study were patients with mood disorders or other disorders, and the temperament data might have been affected by the psychiatric symptoms of these patients. In contrast, the majority of studies that have developed short versions of the TEMPS-A have been conducted on university students, whereas the original short version by Akiskal et al investigated mood disorder patients and healthy volunteers, similar to the present study.Citation4,Citation8,Citation10,Citation12 Measurement invariance across different age groups and across patients and healthy volunteers is important for a questionnaire in terms of the comparability of the results and should be confirmed.Citation20
Conclusion
In conclusion, this study confirmed the firm five-factor structure of the 18-item but not the 39-item Japanese version of the TEMPS-A by CFA, indicating that the 18-item version is more suitable as a Japanese short version of the TEMPS-A than the 39-item version. Additional studies on the short TEMPS-A version should be performed using different age groups, and the five-factor structure should be confirmed by CFA in large populations that include patients and healthy subjects.
Disclosure
The authors report no conflicts of interest in this work.
References
- American Psychiatric AssociationDiagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR)Washington, DCAmerican Psychiatric Publishing2000
- AkiskalHSAkiskalKKHaykalRFTEMPS-A: progress towards validation of a self-rated clinical version of the Temperament Evaluation of the Memphis, Pisa, Paris, and San Diego AutoquestionnaireJ Affect Disord20058531615780671
- AkiskalHSToward a definition of generalized anxiety disorder as an anxious temperament typeActa Psychiatr Scand19983936673
- AkiskalHSMendlowiczMVJean-LouisGTEMPS-A: validation of a short version of a self-rated instrument designed to measure variations in temperamentJ Affect Disord200585455215780675
- HantoucheEGAkiskalHSToward a validation of a tripartite concept of a putative anxious temperament: psychometric data from a French national general medical practice studyJ Affect Disord200585374315780674
- RovaiLMaremmaniAGRuganiFDo Akiskal & Mallya’s affective temperaments belong to the domain of pathology or to that of normality?Eur Rev Med Pharmacol Sci2013172065207923884828
- GotoSTeraoTHoakiNCyclothymic and hyperthymic temperaments may predict bipolarity in major depressive disorder: a supportive evidence for bipolar II1/2 and IVJ Affect Disord2011129343820699193
- ErfurthAGerlachALHellwegIStudies on a German (Münster) version of the temperament auto-questionnaire TEMPS-A: construction and validation of the brief TEMPS-MJ Affect Disord200585536915780676
- KrebsMOKazesMOlieJPThe French version of the validated short TEMPS-A: the temperament evaluation of Memphis, Pisa, Paris and San DiegoJ Affect Disord20069627127317123631
- PretiAVellanteMZuccaGThe Italian version of the validated short TEMPS-A: the temperament evaluation of Memphis, Pisa, Paris and San DiegoJ Affect Disord201012020721219327844
- Ristic-IgnjatovicDHinicDBessonovDTowards validation of the short TEMPS-A in non-clinical adult population in SerbiaJ Affect Disord2014164434924856552
- WoodruffEGenaroLTLandeira-FernandezJValidation of the Brazilian brief version of the temperament auto-questionnaire TEMPS-A: the brief TEMPS-Rio de JaneiroJ Affect Disord2011134657621782248
- YuanCHuangJGaoKValidation of the Chinese version of the short TEMPS-A and its application in patients with mood disordersJ Affect Disord201517017818425243747
- MatsumotoSAkiyamaTTsudaHReliability and validity of TEMPS-A in a Japanese non-clinical population: application to unipolar and bipolar depressivesJ Affect Disord200585859215780679
- MendlowiczMVAkiskalHSKelsoeJRTemperament in the clinical differentiation of depressed bipolar and unipolar major depressive patientsJ Affect Disord20058421922315708419
- AkiskalHSPintoOThe evolving bipolar spectrum: prototypes I, II, III and IVPsychiatr Clin North Am19992251753410550853
- AkiyamaTTsudaHMatsumotoSThe proposed factor structure of temperament and personality in Japan: combining traits from TEMPS-A and MPTJ Affect Disord2005859310015780680
- KodaMKondoTTEMPS-A/MPT as a quick finder for individualized treatments, including those targeting soft bipolarityClin Neuropsychopharmacol Ther201011623
- MorvanYTibaouiFBourdelMCConfirmation of the factorial structure of temperamental autoquestionnaire TEMPS-A in non-clinical young adults and relation to current state of anxiety, depression and to schizotypal traitsJ Affect Disord2011131374421333358
- PretiAVellanteMGabbrielliMConfirmatory factor analysis and measurement invariance by gender, age and levels of psychological distress of the short TEMPS-AJ Affect Disord2013151995100224054919
- Schermelleh-EngelKMoosbruggerHMüllerHEvaluating the fit of structural equation models: tests of significance and descriptive goodness-of-fit measuresMethods Psychol Res Online200382374
- AguiarFAVasconcelosAGNevesFSAffective temperaments: familiarity and clinical use in mood disordersJ Affect Disord2013148535623245466
- AguiarFAVasconcelosAGNevesFSAffective temperaments and antidepressant response in the clinical management of mood disordersJ Affect Disord201415513814124215897
- IlicetoPPompiliMCandileraGSuicide risk and psychopathology in immigrants: a multi-group confirmatory factor analysisSoc Psychiatry Psychiatr Epidemiol2013481105111423096150
- KesebirSVahipSAkdenizFAffective temperaments as measured by TEMPS-A in patients with bipolar I disorder and their first-degree relatives: a controlled studyJ Affect Disord20058512713315780683
- PompiliMRihmerZAkiskalHTemperaments mediate suicide risk and psychopathology among patients with bipolar disordersCompr Psychiatry20125328028521641589
- PompiliMInnamoratiMGondaXAffective temperaments and hopelessness as predictors of health and social functioning in mood disorder patients: a prospective follow-up studyJ Affect Disord201315021622223684516
- PompiliMInnamoratiMGondaXCharacterization of patients with mood disorders for their prevalent temperament and level of hopelessnessJ Affect Disord201416628529125012443
- RybakowskiJKDembinskaDKliwickiSTEMPS-A and long-term lithium response: positive correlation with hyperthymic temperamentJ Affect Disord201314518718922939170