Abstract
Purpose
Pediatric, clinical, and research data suggest that insufficient sleep causes tiredness and daytime difficulties in terms of attention-focusing, learning, and impulse modulation in children with attention deficit hyperactivity disorder (ADHD) or in those with ADHD and primary sleep disorders. The aim of the present study was to examine whether sleep duration was associated with ADHD-like symptoms in healthy, well-developing school-aged children.
Patients and methods
Thirty-five healthy children (20 boys, 15 girls), aged 7–11 years participated in the present study. Each child wore an actigraphic device on their nondominant wrist for two nights prior to use of polysomnography to assess their typical sleep periods. On the third night, sleep was recorded via ambulatory assessment of sleep architecture in the child’s natural sleep environment employing portable polysomnography equipment. Teachers were asked to report symptoms of inattention and hyperactivity/impulsivity on the revised Conners Teacher Rating Scale.
Results
Shorter sleep duration was associated with higher levels of teacher-reported ADHD-like symptoms in the domains of cognitive problems and inattention. No significant association between sleep duration and hyperactivity symptoms was evident.
Conclusion
Short sleep duration was found to be related to teacher-derived reports of ADHD-like symptoms of inattention and cognitive functioning in healthy children.
Introduction
A considerable proportion of elementary school-aged children sleep for less than the recommended 10–11 hours.Citation1 For example, a study conducted in 2004 found that 43% of boys aged 10–11 years slept for less than 9 hours per night.Citation2 Decreases in sleep time combined with increasingly delayed bedtimes suggest that sleep restriction is emerging as a preadolescent problem. A poll conducted by the National Sleep Foundation found that adolescents (6th–12th grade) averaged 0.5–2 hours less than the recommended amount of sleep each night.Citation3 This finding is a major problem, given the negative impact of restricted sleep on the mental and physical health of children and adolescents.
Mounting evidence indicates that sleep has beneficial effects on learning, memory, attention, emotional regulation, and academic success. Conversely, fatigue and insufficient sleep can negatively affect academic performance, self-regulation, and attention, all of which are necessary for success in school (for a review see Gruber et al).Citation4 The aspects of human behavior most affected by fatigue and insufficient sleep are the executive functions, learning, and memory; these are also the key functional domains required for academic success. Sleep loss impairs performance on tasks requiring abstract thinking, creativity, integration, and planning,Citation5 and is associated with a decrease in the efficiency of learning and memory.Citation6–Citation13
Furthermore, pediatric, clinical, and research data suggest that insufficient sleep causes tiredness and daytime difficulties in terms of attention-focusing and impulse modulation.Citation14–Citation17 In 1991, Dahl et alCitation18 observed that such difficulties were very similar to the core symptoms of attention deficit hyperactivity disorder (ADHD), the most commonly diagnosed neuropsychological disorder in children. Subsequently, several researchers have studied the association between sleep and neurobehavioral functioning in children with ADHD with or without sleep-disordered breathing and in children with both ADHD and restless leg syndrome/periodic leg movement disorder.Citation14,Citation19–Citation22 The cited studies consistently demonstrated that, in such populations, sleep disruption was associated with hyperactivity and inattention.Citation22
Although the cited works provide convincing evidence that sleep and attention interact in children with ADHD, or in those with ADHD and any or all of sleep apnea, sleep-disordered breathing, restless leg syndrome, and periodic leg movement disorder, it is not clear whether this is true of typically developing children that do not suffer from any such problems. The few survey- or actigraphy-based studies that have examined the association between short sleep duration and ADHD-like symptoms in typically developing children have yielded conflicting results.Citation23–Citation28 Inconsistent data were evident in both types of studies, with some reports finding associations between short sleep duration and inattentionCitation23,Citation24,Citation26,Citation29,Citation30 and hyperactivity,Citation25,Citation27,Citation28 whereas others did not.Citation23–Citation25,Citation31,Citation32 Reasons for such inconsistencies could be related to methodological differences in the way that sleep was measured. Polysomnography (PSG) was not employed, and no study employed an objective measure of breathing symptoms, and no prior study has measured restless leg syndrome or periodic leg movement disorder using either objective or subjective measures. Breathing symptoms, restless leg syndrome, and periodic leg movement disorder are common conditions, but relatively underdiagnosed in pediatric populationsCitation33 and have been frequently associated with inattention and hyperactivity.Citation34–Citation38
Therefore, the presence of such comorbidities may have confounded prior study results, contributing to inconsistent findings. It is therefore impossible to draw firm conclusions in terms of an association between short sleep duration and symptoms of inattention and hyperactivity/impulsivity in healthy children based on the data of the cited works. This is important because if short sleep duration is indeed associated with ADHD-like symptoms in typically developing children who do not have primary sleep disorders, identification of such an association would support the use of interventions aimed at reducing sleep deprivation. These interventions could therefore help otherwise healthy children to fulfill their potential.
The goal of the present study was to determine whether shorter sleep duration was related to symptoms of inattention and hyperactivity/impulsivity, which are commonly used in the diagnosis of ADHD, in typically developing children. It was hypothesized that shorter sleep duration would be associated with higher teacher ratings of inattention and hyperactivity/impulsivity.
Material and methods
Participants
Thirty-five children (20 boys, 15 girls) aged 7–11 years (mean 8.60 years; standard deviation [SD] 1.12 years) participated in the present study. Psychiatric status was assessed using the Diagnostic Interview Schedule for Children;Citation39 which was administered to parents. Medical information was obtained via a detailed health screening form. Participants were excluded if they had an intelligence quotient (IQ) <;80 (measured using the Wechsler Intelligence Scale for Children, 4th editionCitation40), or any medical or psychiatric conditions. In addition, children with a saturation nadir lower than 90%, with paradoxical breathing, or with periodic limb movements associated with five or more leg movements per hour of sleep were excluded from the study.
Participants were recruited from elementary schools located in districts of middle socioeconomic status. The study was approved by the Research Ethics Board of the Douglas Mental Health University Institute. All enrolled children completed the study. Each child received compensation of CAD75. Parents signed consent forms permitting research team members to contact teachers. In addition, parents sent teachers information on the study, and informed them that team members would be in contact seeking completion of questionnaires. All teachers were contacted by a research assistant and subsequently completed the revised Conners Teacher Rating Scale (CTRS-R).Citation41
Procedure
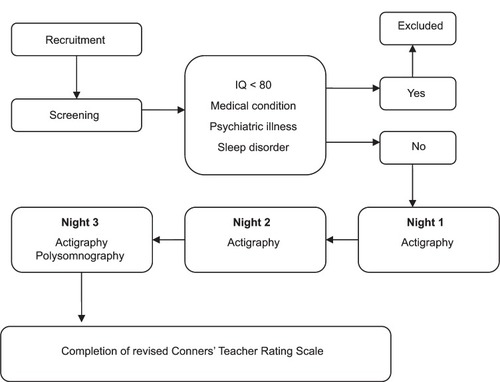
Children were first screened for eligibility. During initial contact, over-the-phone assessment was conducted using the Pediatric Sleep QuestionnaireCitation42 which assesses sleep-disordered breathing, snoring, and sleepiness. In addition, the Chervin and Hedger tool,Citation43 which investigates leg restlessness, experience of growing pains in bed, insomnia, and morning headache, was administered to exclude those with restless leg syndrome. Children scoring 0.33 or higher (ie, replying positively to 33% or more of the 22 questions of either scale) were excluded. Health-related conditions and use of medication were assessed using a health screening form that included a detailed list of questions about each child’s health status. Children who passed over-the-phone screening next visited the laboratory, where both IQ and potential psychological diagnoses were evaluated in a quiet room. After initial screening, children meeting inclusion criteria were invited to participate in the study and their parents received a package that included a sleep assessment battery, a demographic questionnaire, and a consent form. Sleep assessment included use of the morningness–eveningness questionnaire,Citation44 actigraphy, and a sleep log. Parents were asked to complete and return the questionnaire. Teachers were requested to complete the CTRS-RCitation41 based on the week of sleep evaluation. Each child wore an actigraphic device on their nondominant wrist for a period of two nights prior to use of PSG, to assess their usual sleep period. On the third night, sleep was recorded using ambulatory assessment of sleep architecture employing portable PSG equipment. On the scheduled night, a sleep technician arrived at each child’s home 1.5 hours prior to habitual bedtime and connected the sleep recording apparatus. Recording commenced at the child’s habitual bedtime. Sleep pattern and architecture were recorded in the natural home environment because such data afford greater ecological validity than do records logged in sleep laboratories.Citation45–Citation47 For a visual representation of the study design, please see .
Figure 1 Study design.
Measures
Questionnaires/scales for neurobehavioral assessment
ADHD-like symptoms were evaluated using the CTRS-R, a well-validated and reliable instrument used to screen for ADHD in children.Citation41 The CTRS-R has internal consistency ratings of 0.86–0.95 and high test-retest reliability.Citation41 Teachers rated several behaviors on a scale from zero (not true at all) to three (very true), yielding four indices; data from the hyperactivity-impulsivity and cognitive problems/inattention domains were focused on.
The Full Scale IQ score of the Wechsler Intelligence Scale for Children, 4th editionCitation40 was used to estimate general cognitive functioning.
Sleep assessment PSG
An in-home recording procedure was used to assess child sleep architecture, to allow children to sleep in their natural environment. PSG recordings were performed in the children’s homes using a digital ambulatory sleep recorder (Vitaport-3; TEMEC Instruments BV, Kerkrade, the Netherlands), measuring electroencephalography, submental electromyography, electrooculography, and finger pulse oximetry. Electroencephalography electrodes were placed bilaterally along the anteroposterior axes at locations F3, F4, C3, C4, P3, P4, O1, and O2. To assess respiration, two respiratory belts, measuring both chest and abdominal movement, were fitted to detect hypopnea and apneas, respectively, and pulse oximetry was used to measure oxygen saturation. The decision not to use cannula was based on the fact that, whereas the electrooculography, electromyography, and electroencephalography electrodes could be easily twisted together and attached to the recording equipment located close to the child’s head, the use of nasal cannula would interfere with the child’s sleep and would impact the ecological validity of the study.
Electromyography leg electrodes were used to identify leg-movements. Sleep stages were scored visually onscreen (LUNA; Stellate Systems, Montreal, Canada) using the C3 derivation (referential derivation: linked ears) according to standard criteria,Citation48 but employing 20-second epochs.
Various PSG sleep measures were analyzed, but, in the present study, sleep duration was focused on.
Actigraphic measurements
Actigraphs (Actiwatch® 64; Mini Mitter Company Inc, Bend, OR) were used to assess sleep patterns in the natural home environment. These computerized wristwatch-like devices collect data generated by movement. Their use is minimally invasive and the devices therefore allow sleep to be reliably recorded without interfering with family routine. Each actigraphic sleep interval was manually marked with sleep log bedtime and rising time. For each 1-minute epoch, a total activity count was computed. If a threshold value was attained, then the epoch was considered to be wakefulness. If the value fell below that threshold, then the epoch was considered to be sleep. Actigraphic data were analyzed using Actiwatch 64 sleep software (Mini Mitter). The actigraphic parameter of interest was sleep period, representing the amount of time between sleep commencement and wakening. Sleep start and sleep end were automatically determined as the first and last 5-minute periods, respectively, in which no more than a single epoch was scored as mobile.
Circadian preference measure
The Children’s Morningness–Eveningness Preferences Scale,Citation49 a ten-item multiple-choice scale adapted from the Horne–Ostberg morningness–eveningness questionnaire,Citation44 was used to determine circadian preference. The scale ranges from ten (extreme evening preference) to 42 (extreme morning preference).
General evaluation and confounders
To characterize the profiles of the children and reconfirm that the psychological profiles of the study children were within the normal range, the Child Behavior Checklist was used, a frequently utilized dimensional measure of child psychopathology.Citation50,Citation51 Numerous studies have confirmed the stability of the instrument in terms of psychometric properties; the test shows good reliability and validity in both clinical and nonclinical populations.Citation52,Citation53
Body mass index was calculated by dividing weight in kilograms by height in meters squared.
Statistical analyses
Descriptive statistics on demographics, physical, and intellectual characteristics of participants were computed. To determine whether sleep duration on the PSG night was similar to those on the weeknights preceding PSG, Student’s t-test for related samples was used to compare the mean time in bed obtained in the two consecutive nights prior to PSG to the time spent in bed in the PSG night. Multiple linear regression analyses, adjusted for age, IQ, body mass index, and circadian tendency, were used to assess the strength of potential relationships between teacher reports of inattention/cognitive problems or hyperactivity (dependent variables) and total sleep duration as measured by PSG (independent variable). All analyses were performed using IBM SPSS (v 15.0 for Windows; SPSS Inc, Chicago, IL). P <; 0.05 was considered significant.
Results
Demographic and sleep characteristics of all enrolled participants are presented in . The age range was 7–11 years (mean 8.60 years, SD 1.12 years). Twenty (57%) of the children were male. Caucasian children represented 68.6% of enrolled participants, 2.9% had an African-American background, 8.6% were Asian, and 8.6% of mixed race. The average total score on the Child Behavior ChecklistCitation50–Citation53 was 49.77 (SD 9.2), thus confirming that all participants were within the normal range (T score <; 60) on all subscales pertaining to child behavior. All of the participants who were included in the study were below the cutoff score on the Pediatric Sleep Questionnaire,Citation42 had no indication of desaturation, and no paradoxical breathing at the thoracic and abdominal channels ().
Table 1 Sleep, demographic, and clinical characteristics (frequency or mean ± standard deviation) of the sample (n = 35)
The average time slept in bed on the first two nights of actigraphic measurement was 539.64 minutes (SD 59.96 minutes) and 533.54 minutes (SD 59.65 minutes) on the PSG night. Sleep duration measured by PSG was 528 minutes (SD 54.69 minutes). No gender or racial difference was evident in average sleep period or average sleep duration.
No significant difference between the sleep period in the two nights preceding PSG evaluation and the sleep period of the PSG night measured by PSG (t [27] = −0.16; P >; 0.05) was evident. In addition, significant correlation between sleep period, as measured by actigraphy on the PSG night, and sleep duration measured by PSG was found (r = 0.74, P <; 0.005).
To explore whether sleep duration contributed to ADHD-like symptoms in healthy well-developing children, multiple linear regression analyses were performed (). Multiple linear regression analysis revealed that the addition of sleep duration, percentage of sleep stages, and sleep efficacy to the model significantly increased the R2 value, contributing 27% to the explained variance (R2 = 0.65; P <; 0.05) (∆R2 = 0.27) (Fchange [1,29] = 3; P <; 0.05) after controlling for body mass index, circadian tendency, and IQ in predicting cognitive problems/inattention. Sleep duration was found to be a significant predictor in the model predicting scores on teacher-reported cognitive problems and inattention; individuals with shorter sleep duration received higher scores on this scale.
Table 2 Results of regression analyses studying main effects of sleep duration on cognitive problems/inattention and hyperactivity-impulsivity on the revised Conners Teacher Rating Scale
Sleep variables measured by PSG did not contribute significantly to the prediction of teacher-derived data on hyperactivity.
Discussion
The aim of the present study was to explore whether objective measures of sleep duration are associated with teacher ratings of inattention and hyperactivity/impulsivity in healthy, well-developing preadolescent school-aged children who do not suffer from sleep-disordered breathing, restless leg syndrome, or periodic leg movement disorder. The results showed that shorter sleep duration was associated with higher levels of teacher ratings of cognitive problems and inattention. Specifically, short sleep duration, objectively measured using PSG, was significantly related to teacher reports of difficulties in the realms of learning or memory, in organizational skills, and the ability to be attentive when required. However, no significant association between sleep duration and hyperactivity symptoms was evident.
Several previous reports have found that short sleep duration was related to poorer academic performance when measures such as the Standard Achievement Test scores or school grades were employed (for reviews, see Gruber et al,Citation4 Dewald et al,Citation54 and Wolfson and CarskadonCitation55,Citation56). The present findings add to such data by demonstrating a strong association between sleep duration and the day-to-day functioning of children in the school environment, as reported by te achers, who were blind to the sleep status of participants. Both lines of investigation converge to show that shorter sleep is associated with the manifestation of inattention and poorer school-related outcomes. However, the mechanisms underlying these associations remain unclear, which is an important question that needs to be addressed in future research.
The findings are consistent with previous data from studies conducted in healthy adults, which found that deficits resulting from sleep deprivation resemble those seen in patients with prefrontal cortex damage.Citation57 The prefrontal cortex plays a significant role in executive functions,Citation58,Citation59 and sleep loss preferentially impairs functions governed by the prefrontal cortex. Considering that a deficit in executive functions and prefrontal cortex activity is a core feature associated with ADHD,Citation60–Citation64 it is not surprising that short sleep duration in healthy children is associated with ADHD-like symptoms. However, because the present study was correlational in nature, the causes and effects were unable to be determined.
In contrast to the conclusions of previous reports,Citation27,Citation28 short sleep duration was not associated with the manifestation of higher levels of hyperactivity in the present sample of typically developing, non-ADHD school-aged children. Although this is not consistent with previous suggestions regarding the potential impact of sleep deprivation on self-regulation,Citation65–Citation67 the data are in line with those of recent studies showing that different functional domains are differentially affected by sleep deprivation.Citation68 The variations in the association between sleep duration and ADHD-like symptoms emphasize the need to better explore these relationships, as well as to better understand the underlying mechanisms.Citation68
Sleep duration contributed 27% to the explained variance in inattention and cognitive problems even after IQ was considered. If sleep duration is so significantly associated with the manifestation of such ADHD-like symptoms in otherwise healthy children, it is possible that increasing sleep duration might offer an effective and inexpensive opportunity to optimize the school functioning of healthy children. Sleep does not cost money and does not have any negative side effects. A potential practical path to this end is to incorporate sleep education into the practice of health care providers and pediatricians, and into the health curricula of elementary schools, similar to Cain et al’s efforts at establishing motivational school-based interventions.Citation69 In addition, it is critical to educate parents, students, educators, and clinicians on the importance of sleep and to develop tools aimed at preventing sleep deprivation.
The present study extends prior research in various ways. First, sleep was objectively assessed and an ecologically-based measure of ADHD-like symptoms at school was employed. In addition, healthy school-aged children were studied, excluding those with symptoms of primary sleep disorders or ADHD. Further, sleep parameters were measured at home, increasing the ecological validity of the results.
Limitations
Some limitations of this work are apparent. First, the participants were below the cutoff score on the Pediatric Sleep Questionnaire, had no indication of desaturation, and no paradoxical breathing at the thoracic and abdominal channels; however, the presence of sleep-disordered breathing cannot be completely excluded because of the lack of nasal cannula or thermistor. Second, even if a statistical power analysis indicated that the sample size was sufficient for detection of significant effects, the sample size was still relatively small and the results are thus preliminary in nature.
The data support an association between sleep duration and school cognitive performance; however, the mechanisms and potential causes and effects of such association require further exploration. Although sleep duration explained 27% of variance, there are, clearly, additional variables that affect inattention and cognition in healthy children. Future studies are needed to further identify such variables.
Sleep is also affected by the physical and emotional environment of the child/adolescent. Exposure to light or to an uncomfortable temperature in the evening, a high level of stimulation around bedtime, and a noisy environment have all been shown to compromise the ability to obtain sufficient sleep. In addition to physical features, the emotional environment, affected principally by family interactions (eg, marital conflict), also has a significant impact on sleep processes.Citation70 In the present study, interference with regular sleep habits and the sleep environment was minimized by using at-home measurement of sleep parameters. However, environmental factors that might impact child sleep were not able to be identified. Future studies should further delimit the physical and environmental factors contributing to shortening of preadolescent sleep duration.
Conclusion
The findings suggest that short sleep duration is related to teacher-derived reports of ADHD-like symptoms of inattention and cognitive functioning in healthy children. The negative impact of sleep deprivation emphasizes the need to provide children and their parents with education on healthy sleep and tools that assist in achieving such sleep.
Acknowledgments
This study was supported by grants to Dr Gruber from the Canadian Institutes of Health Research (CIHR; grant number 153139) and the Fonds de la recherche en santé du Québec (FRSQ; grant number 10091).
Disclosure
The authors report no conflicts of interest in this work.
References
- HeusslerHSCommon causes of sleep disruption and daytime sleepiness: childhood sleep disorders IIMed J Aust2005182948448915865596
- SpilsburyJCStorfer-IsserADrotarDSleep behavior in an urban US sample of school-aged childrenArch Pediatr Adolesc Med20041581098899415466688
- National Sleep Foundation2006 teens and sleep: sleep in America poll2006 Available from: http://www.sleepfoundation.org/article/sleep-america-polls/2006-teens-and-sleepAccessed July 20, 2010
- GruberRWiebeSTWellsSACassoffJMonsonESleep and academic success: mechanisms, empirical evidence, and interventional strategiesAdolesc Med State Art Rev201021352254121302859
- DahlREThe regulation of sleep and arousal: development and psychopathologyDev Psychopathol199681327
- CurcioGFerraraMDe GennaroLSleep loss, learning capacity and academic performanceSleep Med Rev200610532333716564189
- MaquetPLaureysSPeigneuxPExperience-dependent changes in cerebral activation during human REM sleepNat Neurosci20003883183610903578
- MarshallLBornJThe contribution of sleep to hippocampus-dependent memory consolidationTrends Cogn Sci2007111044245017905642
- OfenNKaoYCSokol-HessnerPKimHWhitfield-GabrieliSGabrieliJDDevelopment of the declarative memory system in the human brainNat Neurosci20071091198120517676059
- RibeiroSNicolelisMAReverberation, storage, and postsynaptic propagation of memories during sleepLearn Mem200411668669615576886
- SchabusMGruberGParapaticsSSleep spindles and their significance for declarative memory consolidationSleep20042781479148515683137
- StickgoldRSleep-dependent memory consolidationNature200543770631272127816251952
- WilsonMAMcNaughtonBLReactivation of hippocampal ensemble memories during sleepScience199426551726766798036517
- ChervinRDDillonJEBassettiCGanoczyDAPituchKJSymptoms of sleep disorders, inattention, and hyperactivity in childrenSleep19972012118511929493930
- CorkumPMoldofskyHHogg-JohnsonSHumphriesTTannockRSleep problems in children with attention-deficit/hyperactivity disorder: impact of subtype, comorbidity, and stimulant medicationJ Am Acad Child Adolesc Psychiatry199938101285129310517062
- O’BrienLMMervisCBHolbrookCRNeurobehavioral correlates of sleep-disordered breathing in childrenJ Sleep Res200413216517215175097
- SteinMAUnravelling sleep problems in treated and untreated children with ADHDJ Child Adolesc Psychopharmacol19999315716810521009
- DahlREPelhamWEWiersonMThe role of sleep disturbances in attention deficit disorder symptoms: a case studyJ Pediatr Psychol19911622292392061790
- ArchboldKHGiordaniBRuzickaDLChervinRDCognitive executive dysfunction in children with mild sleep-disordered breathingBiol Res Nurs20045316817614737917
- BassJLCorwinMGozalDThe effect of chronic or intermittent hypoxia on cognition in childhood: a review of the evidencePediatrics2004114380581615342857
- BeebeDWGozalDObstructive sleep apnea and the prefrontal cortex: towards a comprehensive model linking nocturnal upper airway obstruction to daytime cognitive and behavioral deficitsJ Sleep Res200211111611869421
- MelendresMCLutzJMRubinEDMarcusCLDaytime sleepiness and hyperactivity in children with suspected sleep-disordered breathingPediatrics2004114376877515342852
- FalloneGAceboCArnedtJTSeiferRCarskadonMAEffects of acute sleep restriction on behavior, sustained attention, and response inhibition in childrenPercept Mot Skills200193121322911693688
- FalloneGAceboCSeiferRCarskadonMAExperimental restriction of sleep opportunity in children: effects on teacher ratingsSleep200528121561156716408416
- GauSSKesslerRCTsengWLAssociation between sleep problems and symptoms of attention-deficit/hyperactivity disorder in young adultsSleep200730219520117326545
- PaavonenEJPorkka-HeiskanenTLahikainenARSleep quality, duration and behavioral symptoms among 5–6-year-old childrenEur Child Adolesc Psychiatry2009181274775419466475
- PaavonenEJRaikkonenKLahtiJShort sleep duration and behavioral symptoms of attention-deficit/hyperactivity disorder in healthy 7- to 8-year-old childrenPediatrics20091235e857e86419403479
- TouchetteÉPetitDSéguinJRBoivinMTremblayREMontplaisirJYAssociations between sleep duration patterns and behavioral/cognitive functioning at school entrySleep20073091213121917910393
- AronenETPaavonenEJFjallbergMSoininenMTorronenJSleep and psychiatric symptoms in school-age childrenJ Am Acad Child Adolesc Psychiatry200039450250810761353
- EpsteinRChillagNLaviePStarting times of school: effects on daytime functioning of fifth-grade children in IsraelSleep19982132502569595603
- NixonGMThompsonJMHanDYShort sleep duration in middle childhood: risk factors and consequencesSleep2008311717818220080
- TrabelsiSGuillotSRitaccoHBoueFLangevinDNano structures of colloidal complexes formed in oppositely charged polyelectrolyte/surfactant dilute aqueous solutionsEur Phys J E Soft Matter200723330531117687512
- LumengJCChervinRDEpidemiology of pediatric obstructive sleep apneaProc Am Thorac Soc20085224225218250218
- BeebeDWNeurobehavioral morbidity associated with disordered breathing during sleep in children: a comprehensive reviewSleep20062991115113417040000
- ChervinRDRuzickaDLGiordaniBJSleep-disordered breathing, behavior, and cognition in children before and after adenotonsillectomyPediatrics20061174e769e77816585288
- CorteseSKonofalEYatemanNMourenMCLecendreuxMSleep and alertness in children with attention-deficit/hyperactivity disorder: a systematic review of the literatureSleep200629450451116676784
- GozalDKheirandish-GozalLNeurocognitive and behavioral morbidity in children with sleep disordersCurr Opin Pulm Med200713650550917901756
- WaltersASMandelbaumDELewinDSKuglerSEnglandSJMillerMDopaminergic therapy in children with restless legs/periodic limb movements in sleep and ADHDPediatr Neurol200022318218610734247
- ShafferDFisherPLucasCPDulcanMKSchwab-StoneMENIMH Diagnostic Interview Schedule for Children Version IV (NIMH DISC-IV): description, differences from previous versions, and reliability of some common diagnosesJ Am Acad Child Adolesc Psychiatry2000391283810638065
- WechslerDThe Wechsler Intelligence Scale for Children4th edLondonPearson Assessment2004
- ConnersCKSitareniosGParkerJDEpsteinJNRevision and restandardization of the Conners Teacher Rating Scale (CTRS-R): factor structure, reliability, and criterion validityJ Abnorm Child Psychol19982642792919700520
- ChervinRDHedgerKDillonJEPituchKJPediatric Sleep Questionnaire (PSQ): validity and reliability of scales for sleep-disordered breathing, snoring, sleepiness, and behavioral problemsSleep Med200011213210733617
- ChervinRDHedgerKMClinical prediction of periodic leg movements during sleep in childrenSleep Med20012650151014592265
- HorneJAOstbergOA self-assessment questionnaire to de termine morningness-eveningness in human circadian rhythmsInt J Chronobiol197642971101027738
- IberCRedlineSKaplan GilpinAMPolysomnography performed in the unattended home versus the attended laboratory setting – Sleep Heart Health Study methodologySleep200427353654015164911
- QuanSFGriswoldMEIberCShort-term variability of respiration and sleep during unattended nonlaboratory polysomnography – the Sleep Heart Health StudySleep200225884384912489889
- QuanSFHowardBVIberCThe Sleep Heart Health Study: design, rationale, and methodsSleep19972012107710859493915
- RechtschaffenAKalesAA Manual of Standardized Terminology, Techniques and Scoring System of Sleep Scoring Stages of Human SubjectsWashington, DCPublic Health Service, US Government Printing Office1968
- CarskadonMAFeiferRAceboCReliability of six scales in a sleep questionnaire for adolescentsSleep Res199120421
- AchenbachTMHowellCTQuayHCConnersCKNational survey of problems and competencies among four- to sixteen-year-olds: parents’ reports for normative and clinical samplesMonogr Soc Res Child Dev199156311311770964
- BirdHREpidemiology of childhood disorders in a cross-cultural contextJ Child Psychol Psychiatry199637135498655657
- JensenPSWatanabeHKRichtersJEScales, diagnoses, and child psychopathology: II. Comparing the CBCL and the DISC against external validatorsJ Abnorm Child Psychol19962421511688743242
- SchmeckKPoustkaFDopfnerMDiscriminant validity of the child behaviour checklist CBCL-4/18 in German samplesEur Child Adolesc Psychiatry200110424024711794549
- DewaldJFMeijerAMOortFJKerkhofGABogelsSMThe influence of sleep quality, sleep duration and sleepiness on school performance in children and adolescents: a meta-analytic reviewSleep Med Rev201014317918920093054
- WolfsonARCarskadonMAUnderstanding adolescents’ sleep pa tterns and school performance: a critical appraisalSleep Med Rev20037649150615018092
- WolfsonARCarskadonMASleep schedules and daytime functioning in adolescentsChild Dev19986948758879768476
- HorneJAHuman sleep, sleep loss and behaviour. Implications for the prefrontal cortex and psychiatric disorderBr J Psychiatry19931624134198453439
- KaneMJEngleRWThe role of prefrontal cortex in working-memory capacity, executive attention, and general fluid intelligence: an individual-differences perspectivePsychon Bull Rev20029463767112613671
- RobbinsTWDissociating executive functions of the prefrontal cortexPhilos Trans R Soc Lond B Biol Sci19963511346146314708941958
- ArnstenAFToward a new understanding of attention-deficit hyperactivity disorder pathophysiology: an important role for prefrontal cortex dysfunctionCNS Drugs200923Suppl 1334119621976
- BarkleyRAGenetics of childhood disorders: XVII. ADHD, Part 1: the executive functions and ADHDJ Am Acad Child Adolesc Psychiatry20003981064106810939238
- BerlinLBohlinGNybergLJanolsLOHow well do measures of inhibition and other executive functions discriminate between children with ADHD and controls?Child Neuropsychol200410111314977511
- BrennanARArnstenAFNeuronal mechanisms underlying attention deficit hyperactivity disorder: the influence of arousal on prefrontal cortical functionAnn N Y Acad Sci2008112923624518591484
- WodkaELMostofskySHPrahmeCProcess ex amination of executive function in ADHD: sex and subtype effectsClin Neuropsychol200822582684118609314
- DahlRESleeplessness and aggression in youthJ Adolesc Health200638664164216730589
- IrelandJLCulpinVThe relationship between sleeping problems and aggression, anger, and impulsivity in a population of juvenile and young offendersJ Adolesc Health200638664965516730591
- UmlaufMGBollandJMLianBESleep disturbance and risk behaviors among inner-city African-American adolescentsJ Urban Health20118861130114221638116
- TuckerAMWhitneyPBelenkyGHinsonJMVan DongenHPEffects of sleep deprivation on dissociated components of executive functioningSleep2010331475720120620
- CainNGradisarMMoseleyLA motivational school-based intervention for adolescent sleep problemsSleep Med201112324625121292553
- El-SheikhMSleep and Development: Familial and Socio-cultural ConsiderationsNew YorkOxford University Press2011