
Abstract
Objective
To investigate the influence of obstructive sleep apnea (OSA) severity and weight on blood pressure (BP) during nighttime sleep in children.
Methods
Habitually snoring children who were 3–14 years old and from Beijing Children’s Hospital between 1 January 2018 and 31 December 2020 were recruited. All participants completed polysomnography (PSG) and BP monitoring during different sleep stages using pulse transit time analysis. Subjects were divided into three groups based on the obstructive apnea–hypopnea index (OAHI), ie, primary snoring (PS), mild-to-moderate OSA, and severe OSA group.
Results
Totally, 284 habitually snoring children were enrolled, including 85 with PS, 152 with mild-to-moderate OSA, and 47 with severe OSA. The differences of age and sex ratio among groups were not statistically significant (all P>0.05). For the normal weight group, compared with those in the PS group, children in the severe OSA group had higher BP, mainly in N2 and R stages, and children in the mild-to-moderate OSA group had lower BP in all sleep and wake stages (all P<0.01). For the overweight/obese group, compared with the PS group, children in the severe OSA group had higher BP in all sleep and wake stages, and children in the mild-to-moderate group had higher BP mainly in sleep stages (all P<0.01). Compared with normal weight children, those who were overweight/obese and had OSA had higher BP in all sleep and wake stages (all P<0.01). There was a synergistic effect of OSA and weight status on BP (P<0.01).
Conclusion
The influence of OSA on both systolic and diastolic pediatric BP differs between children with normal weight and overweight/obese status. Overweight/obese status synergistically worsens nocturnal blood pressure in children with OSA. Early diagnosis and risk stratification are more important in overweight/obese children with OSA to achieve timely initiation of treatment.
Introduction
Obstructive sleep apnea (OSA) is a disorder of breathing during sleep, which is mainly characterized by repeated complete or partial obstruction of the upper airway during nighttime, leading to disruption of normal sleep patterns and ventilation during sleep.Citation1 The prevalence of pediatric OSA was 1.2–5.7%. Without effective intervention, OSA can lead to a series of serious complications, such as neurocognitive, behavioral, cardiovascular, and metabolic dysfunctions.Citation1 Cardiovascular complications of OSA include systemic hypertension, endothelial dysfunction, autonomic dysfunction, ventricular remodeling, biventricular dysfunction, and accelerated atherogenesis.Citation2
Various investigations were used to monitor blood pressure (BP) in patients with OSA, including in-office BP measurement, 24-h BP monitoring and continuous BP recordings from polysomnography (PSG).Citation3–Citation6 Children with OSA are at risk of developing high BP levels during both wakefulness and sleep. Many studies in children, including those who are overweight and/or obese, have found that OSA had significant effects on the cardiovascular system, including increased BP, heart rate, and impaired autonomic cardiovascular control.Citation7 Obesity is one of the most important risk factors for disease severity in children with obstructive sleep apnea,Citation8 and children with both disorders are at a greater risk of adverse outcomes across all organ systems. For instance, Walter et al reported that children with both overweight/obesity and OSA are more likely to have arterial stiffness than normal-weight children with OSA and children who do not snore.Citation9 Another two studies found that OSA and obesity affect BP independently and synergistically.Citation10,Citation11
Children with hypertension are more likely to develop a range of cardiometabolic risks,Citation12 and childhood blood pressure is a good predictor of adult blood pressure.Citation13,Citation14 Previous studies have shown that OSA-related variables improved and blood pressure levels decreased in children with OSA after adenotonsillectomy.Citation15–Citation17 Therefore, timely diagnosis and interventions targeting risk factors for adverse cardiovascular outcomes in childhood can prevent more severe cardiovascular complications and reduce medical burdens in adulthood.
However, the influence of OSA severity and weight status on nighttime BP in children has not been fully elucidated. Therefore, we hypothesized that the severity of OSA and overweight/obese status independently affect BP; and OSA and overweight/obese status have a synergistic effect on BP.
Materials and Methods
Subjects
Habitually snoring children who were 3–14 years old and from Beijing Children’s Hospital sleep center between 1 January 2018 and 31 December 2020 were included. Children with diseases such as heart disease, kidney disease that can cause high BP, a history of upper airway surgery, craniofacial malformations, neuromuscular disorders, and various syndromes were excluded. Children who took medications that affect sleep, breathing and BP were also excluded.
Body Measurements
Height was measured with a wall-mounted measuring instrument, and the result was accurate to 0.1cm. Weight was measured with a digital scale, and the result is accurate to 0.1 kg. Body mass index (BMI) is defined as weight divided by height squared. According to the growth curve of Chinese children adjusted for age and sex, BMI >85th and 95th percentiles were considered overweight and obese, respectively.Citation18
Polysomnography (PSG)
The PSG examinations were performed using the SOMNO screen Plus PSG+ V5 system (SOMNO medics GmbH, Germany). The PSG recorded electroencephalogram, electrooculogram, electromyogram, electrocardiogram, pressure and thermal nasal airflow, chest and abdominal motion and oxygen saturation. Sleep stages and respiratory events were scored according to the American Academy of Sleep Medicine manual.Citation19 The obstructive apnea–hypopnea index (OAHI) meant the number of apnea (obstructive and mixed) and hypopnea per hour. Oxygen desaturation index (ODI) and arousal index (ArI) referred to the number of oxygen desaturation≥3% and the number of arousal per hour, respectively. T90 meant the proportion of total sleep time spent with oxygen saturation <90%. The OAHI cut-off value for mild, moderate, and moderate OSA were 1, 5, and 10, respectively. Children with OAHI ≤1 were classified as having primary snoring.Citation1
BP Measurement by Pulse Transit Time Analysis
BP was measured by pulse transit time (PTT) analysis built-into PSG. An electrocardiography was used to monitor the electrical activity of the heart and a fingertip pulse oximeter was used to monitor changes in pulse waves. PTT is defined as the time required to transmit the pulse pressure wave from the left ventricle, ie, the peak of the electrocardiogram R wave, to the predetermined peripheral site, ie, the peak of the pulse wave. As the distance from the left ventricle to the fingertip is positively correlated with body height, BP values related to pulse can be derived and calculated according to PTT and body height. BP value can be obtained for each beat.Citation20 Since the sleep stage score is based on 30 seconds, BP values are obtained every 30 seconds in this study, which is the average of the time, to monitor the BP changes in each sleep stage.
Statistical Analysis
We performed the statistical analysis by using SPSS 23.0 (IBM, Armonk, NY, USA). The normality of data distribution was determined using the Kolmogorov–Smirnov test. Continuous variables were represented by mean ± standard deviation if they conformed to normal distribution, and by median (25th percentile, 75th percentile) if they did not conform to skewness distribution. Differences among groups were tested using Wilcoxon signed-rank test for skewed distributed continuous data, and one-way analysis of variance with least significant difference post hoc testing for normally distributed continuous data. Categorical variables were expressed in terms of number of cases and percentage, and chi-square test was used for comparison between groups. Student t test was used to analyze blood pressure differences between normal weight group and overweight/obese group. Multivariate analysis of variance was used to analyze the main and interactive effects of OSA severity and body weight status on BP. Double-tailed P<0.05 was considered statistically significant.
Results
Demographic and Clinical Information
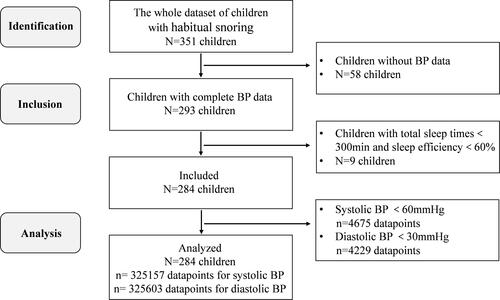
A total of 351 children with habitual snoring were included. Fifty-eight patients were not eligible because of incomplete BP data. Among the 293 eligible patients, four with total sleep time <300 min and five with sleep efficiency <60% were excluded. In total, 284 children were analyzed. According to clinical experience, we removed data points with systolic BP <60 mmHg and diastolic BP <30 mmHg; in total 325,157 systolic BP data points and 325,603 diastolic BP data points were analyzed ().
Figure 1 The flow diagram of the study participants.
The demographic and clinical information of all children are shown in . There were 85 children in the PS group, 152 in the mild-to-moderate OSA group, and 47 in the severe OSA group. One hundred and eighty-four (64.8%) were boys and 109 (38.4%) were overweight/obese. The mean age was 7.7±2.3 years. The median OAHI and BMI was 2.3 events/h and 15.9kg/m2, respectively. The differences of age and sex ratio among the three groups were not statistically significant (all P>0.05). There were significant expected differences in PSG outcomes in the OSA group compared to the PS group, including higher respiratory event index, worse oxygen saturation, and higher arousal index.
Table 1 Differences of Demographic and Polysomnographic Parameters Among the Three Groups
The effects of sleep-disordered breathing (SDB) severity on nighttime BP in different weight status are shown in . For the normal weight status group, compared with those in the PS group, children in the severe OSA group had higher systolic BP in the N2 and R stages and lower systolic BP in the N1, N3, and wake stages; children in the mild-to-moderate OSA group had lower systolic BP in all sleep stages and the wake stage (all P<0.05). In terms of diastolic BP, compared with the PS group, children in the severe OSA group had higher diastolic BP in the N1, N2, and R stages and lower diastolic BP in the N3 and wake stages; children in the mild-to-moderate OSA group had lower diastolic BP in all sleep stages and in the wake stage (all P<0.01). For the overweight or obese status group, compared with the PS group, children in the severe OSA group had higher systolic and diastolic BP in all sleep stages and in the wake stage (all P<0.01); children in the mild-to-moderate group had higher systolic BP in all sleep stages and higher diastolic BP in the N2, N3, and R stage, with lower diastolic BP in the wake stage (all P<0.01).
Table 2 Differences of Nighttime BP Value Among SDB Children in Different Weight Status
The effects of weight status on nighttime BP in different severity of SDB group are shown in . Compared with normal weight status children, those who were overweight/obese and had OSA had higher systolic BP and diastolic BP for all sleep stages and the wake stage; those who were overweight/obese and had PS had higher systolic BP in the N1 and wake stages; lower systolic BP in the N2, N3, and R stages; higher diastolic BP in the N1 and wake stages; and lower diastolic BP in the N3 and R stages (all P<0.01).
Table 3 Differences of Nighttime BP Value Between Normal Weight and Overweight/Obese Group in SDB Children
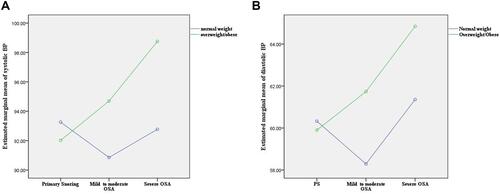
shows the trends in systolic and diastolic BP throughout the night in normal weight and overweight/obese children. shows the results of multivariate analysis of variance and there was a synergistic effect of OSA and weight status on BP (P<0.01).
Figure 2 Trends of blood pressure throughout the night in normal-weight and overweight/obese children. (A) Systolic blood pressure in normal-weight children; (B) Systolic blood pressure in overweight/obese children; (C) Diastolic blood pressure in normal-weight children; (D) Diastolic blood pressure in overweight/obese children.
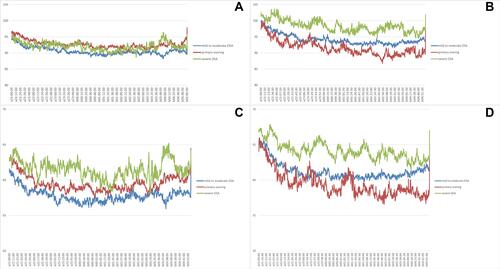
Figure 3 Skeleton map for the effect of OSA and weight status on systolic blood pressure (A) and diastolic blood pressure (B).
Discussion
This study found that the influence of OSA on both systolic and diastolic pediatric BP, is different between children with normal weight and those with overweight/obese status. There was a synergistic effect of OSA and weight status on BP.
In the current study, we found that for children with normal weight, only those in the severe OSA group had higher BP than those in the PS group, which occurred mainly in the N2 and R stages, suggesting that abnormal BP caused by OSA appeared early during sleep, especially in the N2 and R stages. This may be because N2 and R stages are characterized by more respiratory events accompanied by more intermittent hypoxia and pathophysiological changes in sleep fragmentation than the N3 stage.Citation21 For children with overweight/obese status, those in the mild-to-moderate OSA and severe OSA groups had higher BP in almost all sleep stages than those in the PS group. The main finding of our study was the synergistic effect of overweight/obese status on BP in children with OSA; this can also be seen from the BP trend chart for the whole night and confirmed using multivariate analysis of variance. Another noteworthy point is that when compared with children of normal weight status in the PS group, those with overweight/obese status in the PS group had higher BP in N1 and W stages and lower BP in relatively deep sleep, suggesting that abnormal BP caused by weight status mainly appeared during wakefulness.
A number of studies have explored the relationship between OSA and BP in children, however, conclusions from different studies are inconsistent. This study may provide some theoretical basis for the inconsistent results of previous studies. When weight was not subdivided, Leung et alCitation6 found that children with OSA (AHI >5) had higher 24-hour systolic and sleep diastolic blood pressure than the controls. Amin et alCitation22 also showed that children with OSA had a significantly higher 24-h BP. However, there was no positive correlation between OAHI and BP after regression analysis.Citation10,Citation11,Citation23,Citation24 Many studies did not have very large samples, and we believe that this lack of correlation may be due to the counteracting of BP-related effects in children with mild-to-moderate OSA and severe OSA, giving an overall result of OAHI that is not significantly associated with BP in regression models. The association between OSA and BP could be found significantly when the sample size is sufficiently large and there is a sufficient proportion of participants with severe OSA and obesity. One study with a total of 550 children reported that there was an independent correlation between AHI and systolic BP variability during night.Citation25 In view of the inconsistent influence of OSA of varying severity on BP, subgroup analysis can also explain the relationship between OSA and BP more clearly. For example, Chuang et alCitation11 reported that, when OSA was divided into severe and non-severe OSA and incorporated into the logistic model, the risk of hypertension in children with severe OSA was significantly higher than that in the non-severe OSA group. Malakasioti et alCitation26 found that systolic hypertension could predict moderate-to-severe OSA, which is consistent with the findings of Chuang.
Obesity is a risk factor for hypertension in children.Citation12,Citation27 We found that children in the overweight/obese group had a much higher BP than those in the normal weight group, which suggests that obesity can synergistically aggravate cardiovascular system damage in children with OSA. OSA is a chronic disease with long-term cumulative effects on health.Citation28 The interplay between obesity and OSA could worsen disease itself or comorbidities over time.Citation10 As a previous study suggested,Citation28 our findings support the notion that early diagnosis and risk stratification are more important in overweight/obese children with OSA to achieve timely initiation of treatment.
The mechanisms of OSA leading to elevated BP mainly include oxidative stress, inflammation, sympathetic activation and endothelial dysfunction.Citation29 Obesity, which is an independent risk factor for elevated blood pressure, could cause a biological pathway similar to obstructive sleep apnea.Citation30 Clinical and animal studies have shown that repeated oxygen desaturation can induce oxidative stress and sympathetic hyperactivity, resulting in hemodynamic changes and dysfunction of vascular endothelial cells.Citation28,Citation31 Therefore, intermittent hypoxia and obesity may have more severe negative effects on blood pressure when they co-exist.
Adenotonsillectomy is the first line of treatment for OSA even in obese children. In addition, we think that weight control should be undertaken in overweight/obese children with OSA. Weight control cannot be overemphasized, because overweight/obese status can significantly worsen the cardiovascular outcomes of children with OSA. This is important because 75% obese children turn out to be obese adults.Citation32 Several studies have also explored changes in BP after treatment of OSA. One study concluded that children with hypertension experienced a significant reduction in blood pressure variability after adenotonsillectomy.Citation33 A meta-analysis found that there were significant improvements in several factors after adenotonsillectomy in children with OSA, including pulmonary hypertension and left ventricular diastolic function.Citation34 Although it is unclear whether these improvements could predict better long-term cardiovascular outcomes, there is a reason to believe that early diagnosis of OSA would allow earlier treatment and prevent the long-term progression of cardiovascular disease. However, there are very few studies on the effectiveness of weight control alone or weight control combined with other treatments on the improvement of cardiovascular complications in children with OSA.
In addition to the abovementioned clinical significance, the BP measurement method used in this study is also worth pointing out. We used the PTT analysis built into the PSG to measure BP rather than 24-h ambulatory BP monitoring, which has become the most widely used BP monitoring method in recent years.Citation35 PTT is the time it takes for a pulse pressure wave to travel from the left ventricle to a predetermined peripheral location. PTT is influenced by two factors, namely mean arterial blood pressure and the distance between the two sites.Citation20 An important advantage of PTT is that it is a non-invasive and continuous technique that can collect multiple BP values and better reflect BP values during night.Citation36 In addition, the BP value collected by PTT method can correspond to the sleep stage in real time very well.
There are some limitations of this study. First, because of its cross-sectional design, we could not assess whether BP in these children improved after various treatments such as weight control, surgery, or non-invasive ventilation. More follow-up or cohort studies are needed, especially well-designed ones that examine the independent and synergistic effects of improving OSA and obesity. Second, our study lacked a healthy control group of children who did not snore. So, we do not know whether the BP of children with PS is higher than the controls. In the future, we plan to include the healthy children in order to further explore the relationship between BP and sleep-disordered breathing. Third, the PSG conducted did not include CO2 pressure measurements, so that it is not possible to explore whether hypercapnia is associated with elevated BP. Fourth, even though PSG pulse transit time is used as an indirect measure of BP, there are very limited number of pediatric studies validating PTT against blood pressure measurements.
Conclusions
This study found that the influence of OSA on pediatric BP, including systolic and diastolic BP, is different depending on whether the child is normal weight or overweight/obese. Overweight/obese status synergistically worsens nocturnal blood pressure in children with OSA. Early diagnosis and risk stratification are more important in overweight/obese children with OSA to achieve timely initiation of treatment. Although adenotonsillectomy remains the first line of treatment for OSA even in obese children, weight control weight loss should not be ignored.
Abbreviations
ArI, arousal index; BMI, body mass index; BP, blood pressure; N1%, percentage of non-REM sleep stage 1 of total sleep time; N2%, percentage of non-REM sleep stage 2 of total sleep time; N3%, percentage of non-REM sleep stage 3 of total sleep time; OAHI, obstructive apnea–hypopnea index; OSA, obstructive sleep apnea; ODI, oxygen desaturation index; PS, primary snoring; PSG, polysomnography; PTT, pulse transit time; R%, percentage of REM sleep stage of total sleep time; SDB, sleep-disordered breathing; SpO2, oxygen saturation; T90, proportion of total sleep time with oxygen saturation <90%.
Data Sharing Statement
The datasets generated and analysed during the current study are available from the corresponding author (Prof. Zhifei Xu) on reasonable request.
Ethics Approval and Informed Consent
This study complies with the Declaration of Helsinki. Ethical approval for this study was granted by the Ethics Committee of Beijing Children’s Hospital. Written informed consent was obtained from the children or their parents. This study was registered at clinical trials (website: https://clinicaltrials.gov/) and the number is NCT02447614.
Acknowledgments
We are very grateful to the technicians at the Sleep Center in Beijing Children’s Hospital for doing the sleep and associated events scoring. We also conducted a study on the children who participated in this study.
Disclosure
The authors declare that they have no competing interests.
Additional information
Funding
References
- Working Group of Chinese Guideline for the Diagnosis and Treatment of Childhood OSA; Subspecialty Group of Pediatrics, Society of Otorhinolaryngology Head and Neck Surgery, Chinese Medical Association; Subspecialty Group of Respiratory Diseases, Society of Pediatrics, Chinese Medical Association. Chinese guideline for the diagnosis and treatment of childhood obstructive sleep apnea (2020). Pediatr Investig. 2021;5):167–187.
- Gallucci M, Gessaroli M, Bronzetti G, et al. Cardiovascular issues in obstructive sleep apnoea in children: a brief review. Paediatr Respir Rev. 2021;38:45–50. doi:10.1016/j.prrv.2020.05.007
- Nisbet LC, Yiallourou SR, Nixon GM, et al. Characterization of the acute pulse transit time response to obstructive apneas and hypopneas in preschool children with sleep-disordered breathing. Sleep Med. 2013;14(11):1123–1131. doi:10.1016/j.sleep.2013.06.010
- Li AM, Au CT, Sung RY, et al. Ambulatory blood pressure in children with obstructive sleep apnoea: a community based study. Thorax. 2008;63(9):803–809. doi:10.1136/thx.2007.091132
- Kang K-T, Chiu S-N, Weng W-C, et al. Comparisons of office and 24-hour ambulatory blood pressure monitoring in children with obstructive sleep apnea. J Pediatr. 2017;182:177–183. doi:10.1016/j.jpeds.2016.11.032
- Leung LC, Ng DK, Lau MW, et al. Twenty-four-hour ambulatory BP in snoring children with obstructive sleep apnea syndrome. Chest. 2006;130(4):1009–1017. doi:10.1016/S0012-3692(15)51134-3
- Nisbet LC, Yiallourou SR, Walter LM, et al. Blood pressure regulation, autonomic control and sleep disordered breathing in children. Sleep Med Rev. 2014;18(2):179–189. doi:10.1016/j.smrv.2013.04.006
- Kang KT, Lee PL, Weng WC, et al. Body weight status and obstructive sleep apnea in children. Int J Obes. 2012;36(7):920–924. doi:10.1038/ijo.2012.5
- Walter LM, Tamanyan K, Limawan AP, et al. Overweight and obese children with sleep disordered breathing have elevated arterial stiffness. Sleep Med. 2018;48:187–193. doi:10.1016/j.sleep.2018.05.007
- Horne R, Shandler G, Tamanyan K, et al. The impact of sleep disordered breathing on cardiovascular health in overweight children. Sleep Med. 2018;41:58–68. doi:10.1016/j.sleep.2017.09.012
- Chuang HH, Hsu JF, Wang CY, et al. Hypertension in children with obstructive sleep apnea syndrome-age, weight status, and disease severity. Int J Environ Res Public Health. 2021;18(18):9602. doi:10.3390/ijerph18189602
- Wuhl E. Hypertension in childhood obesity. Acta Paediatr. 2019;108(1):37–43. doi:10.1111/apa.14551
- Rao G. Diagnosis, epidemiology, and management of hypertension in children. Pediatrics. 2016;138. doi:10.1186/s12887-016-0669-8
- Flynn JT, Kaelber DC, Baker-Smith CM, et al. Clinical practice guideline for screening and management of high blood pressure in children and adolescents. Pediatrics. 2017;140:e20171904.
- Vlahandonis A, Yiallourou SR, Sands SA, et al. Long-term changes in heart rate variability in elementary school-aged children with sleep-disordered breathing. Sleep Med. 2014;15(1):76–82. doi:10.1016/j.sleep.2013.06.023
- Lee CH, Kang KT, Chiu SN, et al. Association of adenotonsillectomy with blood pressure among hypertensive and nonhypertensive children with obstructive sleep apnea. JAMA Otolaryngol Head Neck Surg. 2018;144(4):300–307. doi:10.1001/jamaoto.2017.3127
- Ng DK, Wong JC, Chan CH, et al. Ambulatory blood pressure before and after adenotonsillectomy in children with obstructive sleep apnea. Sleep Med. 2010;11(7):721–725. doi:10.1016/j.sleep.2009.10.007
- Zong XN, Li H. Construction of a new growth references for China based on urban Chinese children: comparison with the WHO growth standards. PLoS One. 2013;8(3):e59569. doi:10.1371/journal.pone.0059569
- Berry RB, Quan SF, Abreu AR, et al.; for the American Academy of Sleep Medicine. The AASM manual for the scoring of sleep and associated events: rules, terminology and technical specifications. Version 2.6. Darien, IL: American Academy of Sleep Medicine; 2020.
- Mukkamala R, Hahn JO, Inan OT, et al. Toward ubiquitous blood pressure monitoring via pulse transit time: theory and practice. IEEE Trans Biomed Eng. 2015;62(8):1879–1901. doi:10.1109/TBME.2015.2441951
- Wu B, Cai J, Yao Y, et al. [Relationship between sleep architecture and severity of obstructive sleep apnea]. Zhejiang Da Xue Xue Bao Yi Xue Ban. 2020;49(4):455–461. Chinese. doi:10.3785/j.issn.1008-9292.2020.08.02
- Amin R, Somers VK, McConnell K, et al. Activity-adjusted 24-hour ambulatory blood pressure and cardiac remodeling in children with sleep disordered breathing. Hypertension. 2008;51(1):84–91. doi:10.1161/HYPERTENSIONAHA.107.099762
- Khan MA, Mathur K, Barraza G, et al. The relationship of hypertension with obesity and obstructive sleep apnea in adolescents. Pediatr Pulmonol. 2020;55(4):1020–1027. doi:10.1002/ppul.24693
- Fraire JA, Deltetto NM, Catalani F, et al. Prevalence of sleep-disordered breathing among adolescents and its association with the presence of obesity and hypertension. Arch Argent Pediatr. 2021;119(4):245–250. doi:10.5546/aap.2021.eng.245
- Kang KT, Chiu SN, Weng WC, et al. 24-Hour ambulatory blood pressure variability in children with obstructive sleep apnea. Laryngoscope. 2021;131(9):2126–2132. doi:10.1002/lary.29455
- Malakasioti G, Alexopoulos EI, Batziou N, et al. Frequency of moderate-to-severe obstructive sleep apnea syndrome among children with snoring and blood pressure in the hypertensive range. Pediatr Nephrol. 2020;35(8):1491–1498. doi:10.1007/s00467-020-04544-0
- Hsu CY, Lin RH, Lin YC, et al. Are body composition parameters better than conventional anthropometric measures in predicting pediatric hypertension? Int J Environ Res Public Health. 2020;17(16):5771. doi:10.3390/ijerph17165771
- Horne R. Endothelial damage in children with sleep-disordered breathing. Am J Respir Crit Care Med. 2020;202(11):1497–1499. doi:10.1164/rccm.202007-2690ED
- Bhattacharjee R, Kheirandish-Gozal L, Pillar G, et al. Cardiovascular complications of obstructive sleep apnea syndrome: evidence from children. Prog Cardiovasc Dis. 2009;51(5):416–433. doi:10.1016/j.pcad.2008.03.002
- Pack AI, Gislason T. Obstructive sleep apnea and cardiovascular disease: a perspective and future directions. Prog Cardiovasc Dis. 2009;51(5):434–451. doi:10.1016/j.pcad.2009.01.002
- Kimura H, Ota H, Kimura Y, et al. Effects of intermittent hypoxia on pulmonary vascular and systemic diseases. Int J Environ Res Public Health. 2019;16(17):3101. doi:10.3390/ijerph16173101
- Guo SS, Wu W, Chumlea WC, et al. Predicting overweight and obesity in adulthood from body mass index values in childhood and adolescence. Am J Clin Nutr. 2002;76(3):653–658. doi:10.1093/ajcn/76.3.653
- Kang KT, Chiu SN, Weng WC, et al. Ambulatory blood pressure variability after adenotonsillectomy in childhood sleep apnea. Laryngoscope. 2022. doi:10.1002/lary.30058
- Ehsan Z, Ishman SL, Kimball TR, et al. Longitudinal cardiovascular outcomes of sleep disordered breathing in children: a meta-analysis and systematic review. Sleep. 2017;40(3). doi:10.1093/sleep/zsx015.
- Smith LA, Dawes PJ, Galland BC. The use of pulse transit time in pediatric sleep studies: a systematic review. Sleep Med Rev. 2018;37:4–13. doi:10.1016/j.smrv.2016.11.006
- Foo JY, Wilson SJ. Clinical applications of pulse transit time in paediatric critical care. J Med Eng Technol. 2009;33(1):79–86. doi:10.1080/03091900701860210