
Abstract
Purpose
This investigation sought to elucidate the genetic underpinnings that connect obesity indicators, circulating blood lipid levels, adipokines levels and obstructive sleep apnea syndrome (OSAS), employing a bidirectional two-sample Mendelian randomization (MR) analysis that utilizes data derived from extensive genome-wide association studies (GWAS).
Methods
We harnessed genetic datasets of OSAS available from the FinnGen consortium and summary data of four obesity indices (including neck circumference), seven blood lipid (including triglycerides) and eleven adipokines (including leptin) from the IEU OpenGWAS database. We primarily utilized inverse variance weighted (IVW), weighted median, and MR-Egger methods, alongside MR-PRESSO and Cochran’s Q tests, to validate and assess the diversity and heterogeneity of our findings.
Results
After applying the Bonferroni correction, we identified significant correlations between OSAS and increased neck circumference (Odds Ratio [OR]: 3.472, 95% Confidence Interval [CI]: 1.954–6.169, P= 2.201E-05) and decreased high-density lipoprotein (HDL) cholesterol levels (OR: 0.904, 95% CI: 0.858–0.952, P= 1.251E-04). Concurrently, OSAS was linked to lower leptin levels (OR: 1.355, 95% CI: 1.069–1.718, P= 0.012) and leptin receptor levels (OR: 0.722, 95% CI: 0.530–0.996, P= 0.047). Sensitivity analyses revealed heterogeneity in HDL cholesterol and leptin indicators, but further multiplicative random effects IVW method analysis confirmed these correlations as significant (P< 0.05) without notable heterogeneity or horizontal pleiotropy in other instrumental variables.
Conclusion
This investigation compellingly supports the hypothesis that OSAS could be a genetic predisposition for elevated neck circumference, dyslipidemia, and adipokine imbalance. These findings unveil potential genetic interactions between OSAS and metabolic syndrome, providing new pathways for research in this domain. Future investigations should aim to delineate the specific biological pathways by which OSAS impacts metabolic syndrome. Understanding these mechanisms is critical for developing targeted prevention and therapeutic strategies.
Introduction
Obstructive sleep apnea syndrome (OSAS) represents a multifaceted disorder with intricate pathophysiological characteristics. It is principally marked by nocturnal sleep snoring with apnea and daytime somnolence. The pathogenesis of OSAS predominantly involves partial or complete obstruction of the upper airway during sleep, culminating in intermittent hypoxia (IH) and sleep fragmentation.Citation1 Concurrent with the global rise in obesity rates, the incidence of OSAS has escalated markedly, eliciting considerable public health concern. Empirical evidence suggests that obesity is a principal risk factor for OSAS, with its prevalence in obese cohorts reaching up to 30%, in stark contrast to the 2–4% in the general population. This prevalence escalates to an alarming 50–98% in severely obese individuals.Citation2 Furthermore, OSAS is intricately linked with increased sympathetic nervous activity, systemic inflammation, oxidative stress and endothelial dysfunction. These elements, in conjunction with obesity, synergistically contribute to the pathogenesis and progression of associated complications, including metabolic syndrome and cardiovascular diseases.Citation3,Citation4 Additionally, obesity-induced disturbances in adipokine metabolism, abnormalities in C-reactive protein (CRP) and an increase in other cardiovascular risk markers, are pivotal in the development and progression of OSAS and its complications. While clinical research has identified associations between obesity, dyslipidemia, adipokines and OSAS, these studies grapple with confounding factors and reverse causality, leading to contentious findings. To mitigate these issues, our study adopts a Mendelian randomization (MR) approach within epidemiological research, utilizing a spectrum of genetic variants as instrumental variables (IVs) for causal inference.Citation5 MR studies stand out for their potential to diminish confounding influences, thus shedding new light on the potential causal links between these metabolic indicators and OSAS.
The primary objective of this study is to delineate the causal associations between OSAS and obesity, circulating blood lipid concentrations and adipokine levels from a genetic standpoint, employing MR methodologies. Through this investigation, we aim to deepen our comprehension of the pathophysiological underpinnings of OSAS and furnish robust scientific evidence to inform the development of more efficacious prevention and treatment strategies.
Methods
Study Design
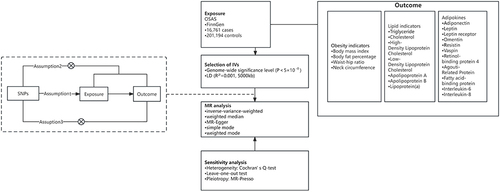
The aim of this study was to evaluate the causal interconnections between OSAS and factors such as obesity, blood lipid concentrations, and adipokine levels. This was achieved by performing bidirectional two-sample MR analysis on datasets sourced from genome-wide association studies (GWAS). The datasets utilized in this research are publicly accessible GWAS data, and the corresponding ethical approvals are detailed in the respective original studies. To ensure the robustness of our findings, sensitivity analyses were systematically conducted. The foundational assumptions of our MR analyses are threefold: (1) the IVs are strongly associated with the exposure factors; (2) the IVs are independent of any confounders that might influence the exposure and outcome relationship; (3) the IVs influence the outcome variables exclusively through these exposure factors. The specifics of the MR study design are depicted in . To mitigate the risk of false positives arising from multiple comparisons, this study implemented the Bonferroni correction method, setting the threshold for statistical significance at a P value less than 0.0023 (where P= 0.05/22). Results yielding a P value between 0.0023 and 0.05 were deemed as suggestive.
Figure 1 Graphical representation of the MR assumptions.
Data Sources and Instrumental Variables Selection
In the context of this study, we categorized obesity indicators into four primary measurements: body mass index (BMI), body fat percentage (BFP), neck circumference (NC), and waist-hip ratio (WHR). The serum lipid biomarkers under investigation encompass a broad spectrum, comprising triglycerides (TG), total cholesterol (TC), low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, lipoprotein A [Lp(a)], apolipoprotein A (ApoA) and apolipoprotein B (ApoB). Additionally, the study focuses on a range of adipokines, which are crucial in metabolic regulation. These include leptin, adiponectin, leptin receptor, resistin, vaspin, omentin, retinol-binding protein 4 (RBP4), interleukin-6 (IL-6), interleukin-8 (IL-8), agouti-related protein (AGRP) and fatty acid-binding protein (FABP). Each of these biomarkers plays a pivotal role in the metabolic pathways and is hypothesized to contribute to the pathophysiology of OSAS.
The GWAS summary datasets pertaining to obesity indicators, serum lipid biomarkers and adipokines were acquired from the OpenGWAS database, a resource developed by the MRC Integrative Epidemiology Unit (IEU) at the University of Bristol (https://gwas.mrcieu.ac.uk/). These datasets encompass over 450,000 individuals predominantly of European descent. To establish robust associations between genetic variants and the various lipid biomarkers, we meticulously selected genetic variants exceeding the genome-wide significance threshold (P<5×10−8) for our MR analysis. In instances where multiple GWAS datasets were available for a particular factor, preference was given to the dataset containing the largest number of validated genetic instruments. These approaches were adopted to ensure the highest level of precision and reliability in our analysis.
The summary-level data for OSAS were sourced from a recent GWAS. This study encompassed 16,761 OSAS patients and 201,194 control participants, drawn from the Finnish Genetics Study.Citation6 The diagnosis of OSAS in this cohort adhered to the criteria set forth in the International Classification of Diseases, 10th revision (ICD-10) and 9th revision (ICD-9), specifically under the codes ICD-10: G47.3 and ICD-9: 3472A. Diagnostic criteria were comprehensive, incorporating subjective symptom reports from patients, clinical examinations, and objective measures from sleep recordings. Notably, a threshold of at least five apnea-hypopnea indices or respiratory event indices per hour was employed as a diagnostic benchmark ().Citation7
Table 1 Characteristics of GWAS Consortiums Used for Each Variable
Instrumental Variable (IV)
In this investigation, we implemented a bifurcated approach to pinpoint IVs linked with OSAS. Initially, single nucleotide polymorphisms (SNPs) exhibiting significant associations with OSAS were identified at the gene level (P<5.0×10−8, R2<0.001, cluster window size = 5,000 kb), with a focus on ensuring these SNPs were not correlated with the study outcome. Subsequently, IVs of insufficient strength were excluded by calculating the F-statistic for each SNP, defined as F = beta2/se2, where beta denotes the estimate and se denotes the standard error of the allele impacting the exposure.Citation8 An elevated F-statistic implies that these analyses are less susceptible to weak instrumental bias.Citation9 Comprehensive details regarding the IVs utilized in this study are available in Supplementary Table S1.
Statistical Analysis
This study is dedicated to exploring the causal links between OSAS and a spectrum of health indicators, including obesity indicators, circulating blood lipid levels, and adipokines levels. To achieve this objective, a suite of methodological tools was employed, each selected for its distinct advantages in evaluating the accuracy and underlying assumptions of the relationship between genetic variants and health outcomes. These tools include inverse variance weighting (IVW), MR-Egger regression, weighted median estimation, simple mode, and weighted mode. The IVW method amalgamates the Wald estimate for each SNP to yield a comprehensive estimate through meta-analysis. This approach is particularly effective in scenarios devoid of horizontal pleiotropy, where genetic variants do not influence other factors, thus providing unbiased results.Citation10 The MR-Egger method offers dual benefits: it furnishes consistent estimates of causal effects under less stringent assumptions and identifies potential directional pleiotropy exerted by genetic variants.Citation11 Meanwhile, the weighted median estimation remains reliable even if up to 50% of the genetic variants deviate from MR assumptions.Citation12
To mitigate bias stemming from horizontal pleiotropy, we utilized MR-PRESSO and MR-Egger intercept regression for detecting significant horizontal pleiotropy across all outcomes.Citation13 Additionally, we performed leave-one-out analysis to evaluate the impact of individual SNPs on outcomes. The robustness of our results was further fortified by conducting heterogeneity tests, including Cochran’s Q statistic and multiplicative random effects IVW method (IVW-mre), on statistically significant findings, with a P value threshold of less than 0.05. In cases where heterogeneity, rather than horizontal pleiotropy, was observed, a random effects IVW MR analysis was deemed appropriate.
Furthermore, reverse MR analyses were conducted between OSAS and the aforementioned health indicators, adhering to a selection criterion of P < 5×10−8 for SNPs, utilizing the same methods and theoretical framework as in the forward MR analyses. All statistical procedures were executed using two-sample MR and MR-PRESSO within the R software environment.Citation13,Citation14
Results
In this investigation, we identified 102 SNPs significantly associated with OSAS as IVs from the GWAS dataset. SNPs that might introduce bias due to continuous imbalance were excluded (Supplementary Table S1). All selected SNPs demonstrated F values exceeding 10, underscoring the robustness of these IVs and mitigating the risk of bias from weak IVs.
Our analyses revealed associations of OSAS with various obesity indicators (notably NC), lipid levels (including TG, HDL cholesterol, LDL cholesterol and ApoB), and adipokines (such as leptin and leptin receptor) in at least one MR method. Specifically, the IVW method (, Supplementary Figure S1) indicated that OSAS is a risk factor for increased NC (Odds Ratio [OR]: 3.472, 95% Confidence Interval [CI]: 1.954–6.169, P= 2.201E-05), elevated TG levels (OR: 1.029, 95% CI: 1.003–1.056, P= 0.027), decreased HDL cholesterol levels (OR: 0.904, 95% CI: 0.858–0.952, P= 1.251E-04), decreased LDL cholesterol levels (OR: 0.962, 95% CI: 0.936–0.989, P= 6.667E-03), and decreased ApoB levels (OR: 0.987, 95% CI: 0.971–0.995, P= 4.245E-3), as well as increased leptin levels (OR: 1.355, 95% CI: 1.069–1.718, P= 0.012) and decreased leptin receptor levels (OR: 0.722, 95% CI: 0.530–0.996, P= 0.047). Furthermore, we employed MR-Egger regression, weighted median estimation and both unadjusted and adjusted models to validate these results. While the IVW method indicated a causal relationship between OSAS and variables such as TG, LDL cholesterol and ApoB, the MR-Egger method suggested a contrasting directionality, thus challenging the causal inference (Supplementary Figure S2). To evaluate the stability of these findings, multiple effects detection was performed using MR-PRESSO and MR-Egger intercept regression, which indicated no significant potential multiple effects. The robustness of our findings was corroborated by leave-one-out sensitivity analyses, demonstrating that no single genetic instrument drove the results (Supplementary Figure S3). Cochran’s Q statistic revealed no significant heterogeneity in the effects of SNPs on NC, TG, LDL cholesterol, ApoB and leptin receptor. However, some degree of heterogeneity was noted in HDL cholesterol and leptin, necessitating further analysis using the IVW-mre approach. Funnel plots supported the stability of our methodology (Supplementary Table S2-4 and Supplementary Figure S4).
Table 2 Bidirectional MR Results of Obesity Indicators, Lipid Indicators, Adipokines and OSAS
Multiple tests conducted on these results, applying the Bonferroni correction, affirmed that the occurrence of OSAS is significantly correlated with increased NC and decreased HDL cholesterol levels. While other biomarkers, such as TG, LDL cholesterol, ApoB, leptin and leptin receptor levels, exhibited trends (as indicated by their OR values), they did not reach statistical significance post-Bonferroni correction, with P values exceeding 0.0023. It is critical to note that while these changes in biomarkers may not achieve statistical significance, they could still bear biological or clinical relevance.
In the reverse analysis segment of our study, we explored the causal relationships between obesity metrics, lipid levels, adipokines and OSAS (Supplementary Table S5). Our study identified a significant correlation between elevated levels of BMI (OR: 2.133, 95% CI: 1.935–2.351, P= 2.378E-52), BFP (OR: 2.040, 95% CI: 1.773–2.346, P= 2.074E-23), and TG (OR: 1.077, 95% CI: 1.006–1.153, P= 0.033) and the heightened risk of OSAS. These findings underscore the significant impact of these factors in predicting the likelihood of developing OSAS. However, the application of MR-PRESSO and MR-Egger intercept regression for stability testing revealed potential multiple effects (Supplementary Table S6-8). This finding necessitates a cautious approach in interpreting these associations, particularly regarding their influence on the overall conclusions of our study. The presence of potential multiple effects underscores the complexity of the causal relationships in question and highlights the need for further investigation to fully understand the intricate interplay between these metabolic factors and OSAS.
Discussion
Previous observational studies have established correlations between OSAS and various metabolic parameters, including obesity, lipid levels and adipokine levels.Citation15–17 However, these studies have been limited in their ability to ascertain the precise nature of the causal relationships involved. To our knowledge, this is the inaugural study employing MR methods at the genetic level to investigate the causal linkage between OSAS and these metabolic factors. By utilizing a spectrum of MR approaches, we have significantly bolstered the stability and reliability of our results, thereby providing a more convincing level of causal evidence compared to traditional observational studies.
Our findings indicate that OSAS plays a substantial role in increasing NC and decreasing HDL cholesterol levels. Additionally, our results suggest potential impacts on the increase in leptin levels, and decrease in leptin receptor levels. These insights contribute to a deeper understanding of the complex interplay between OSAS and metabolic disturbances, potentially guiding future research and therapeutic strategies.
OSAS and Neck Circumference
This study corroborates the association between an increased risk of NC enlargement and OSAS, thereby aligning with the research conducted by Altan Onat et al and Viktória Molnár et al.Citation15,Citation18 Altan Onat et al undertook a comprehensive observational study involving 25 patients with severe OSAS (Apnea-Hypopnea Index [AHI] ≥ 30 events per hour) and 19 with non-severe OSAS (AHI < 30 events per hour). Their findings indicated a positive correlation between increased NC and the severity of OSAS.Citation15 Similarly, Viktória Molnár et al conducted an analysis utilizing magnetic resonance imaging (MRI) to examine the adipose tissue parameters of the upper airways in 36 non-OSA control subjects, 32 patients with mild OSAS, and 32 with moderately-severe OSAS.Citation18 By applying artificial intelligence techniques to these MRI data, they identified age, percentage of tongue fat, and NC as crucial predictors of OSAS. Their results demonstrated that an increase in NC was positively correlated with OSAS severity and served as an independent predictor of severe OSAS. These collective findings underscore the significance of NC as not only a marker for the presence of OSAS but also as an indicator of its severity. This highlights the importance of including NC measurements in the clinical assessment and risk stratification of patients suspected of having OSAS.
Recent findings have illuminated that increased NC offers greater specificity and sensitivity in diagnosing OSAS when compared to traditional obesity indicators such as BMI, BFP and WHR.Citation19 This enhanced diagnostic capability can be attributed to the direct correlation between NC and adipose tissue accumulation around the upper airway, which is intimately linked to the pathophysiological mechanisms underlying OSAS. The proliferation of subcutaneous and peripharyngeal fat in the upper airway results in the enlargement of soft tissues. This not only augments neck thickness, leading to increased NC, but also constricts the upper airway. This constriction affects the airway’s compliance and heightens the risk of airway collapse during sleep.Citation20
Furthermore, increased NC in OSAS patients may be indicative of diminished aerobic capacity, reduced physical activity and fluid retention.Citation21,Citation22 Prior research has established a connection between upper body subcutaneous fat (excluding abdominal fat) and aerobic capacity.Citation23 Hormonal fluctuations in OSAS patients, such as elevated cortisol levels, may contribute to fat accumulation in the neck and upper trunk, thereby influencing anthropometric indices.Citation24 Additionally, Stefania Redolfi et al have shown that increased NC may be a direct consequence of nocturnal fluid shifts from the lower limbs to the upper body in OSAS patients.Citation25 These insights underscore the significance of NC as a critical risk assessment tool for OSAS. NC is also associated with elevated levels of the prothrombotic factor plasminogen activator inhibitor-1 (PAI-1), which is closely related to the risk of cardiovascular diseases and the pathogenesis of atherosclerosis.Citation26 Future research may benefit from focusing on interventions aimed at reducing fat accumulation in the neck region, which could potentially mitigate the risk and severity of OSAS.
OSAS and Dyslipidemia
OSAS emerges as a significant risk factor for dyslipidemia. This investigation delineates a substantial association between attenuated HDL cholesterol levels and specific genetic variances, persisting post Bonferroni adjustment. These observations align with the research conducted by Dimitar Karkinski et al and Viseslav Popadic et al.Citation27,Citation28 Karkinski et al’s cross-sectional analysis demonstrated that individuals diagnosed with OSA and a BMI of ≤ 30 kg/m2 exhibit notably diminished HDL cholesterol levels in comparison to their OSA-negative counterparts.Citation27 In a retrospective cohort encompassing 328 subjects with OSAS, Popadic and colleagues discerned a heightened propensity for metabolic syndrome in patients with severe OSAS (AHI ≥30 events per hour), marked by significantly reduced HDL cholesterol.Citation28 Notably, HDL cholesterol levels were found to be inversely related to the severity of OSAS. Prevailing epidemiological studies have substantiated plasma HDL cholesterol concentration as a robust, independent prognosticator of coronary heart disease in the general populace.Citation28 The cardioprotective role of HDL is underscored by its diverse subfractions; notably, smaller subfractions such as LDL 3-7 and HDL 8-10 contribute to atherosclerotic developments in OSAS patients.Citation29 Furthermore, the antioxidative capacity of larger HDL subfractions may be compromised due to escalated high-density lipid peroxide (LPO) levels and a decline in serum paraoxonase-1 (PON1) activity, pivotal determinants of HDL’s antioxidative efficacy.Citation30 This phenomenon potentially elucidates the diminished cardioprotective effect of HDL in OSAS patients, including those with normative HDL concentrations.
The proposed pathogenesis of dyslipidemia in OSAS is intricately linked to oxidative stress and inflammatory responses. The fundamental pathophysiological change in OSAS is IH, a consequence of repeated airway obstruction and reopening. This cycle leads to ATP depletion and subsequent activation of xanthine oxidase, culminating in an overproduction of reactive oxygen species (ROS).Citation31 Among these, hydroxyl radicals (OH-)—the most potent ROS components—initiate lipid peroxidation upon interacting with susceptible lipids.Citation32 This process affects lipid membranes, lipoproteins and other lipid-containing molecules. The peroxidative decomposition of unsaturated fatty acids yields LPO end-products such as malondialdehyde (MDA). MDA imparts biological dysfunction to lipid molecules, potentially leading to cell membrane damage and dysfunction. Additionally, MDA can modify the conformation of proteins by reacting with lysine residues, thereby impacting the functionality of enzymes and transport proteins crucial for lipid transport and metabolism.Citation33,Citation34 Furthermore, MDA can react with proteins and lipids in LDL to form oxidized LDL (oxLDL). OxLDL is a key contributor to atherosclerosis, as it can be taken up by macrophages, transforming them into foam cells.Citation35
IH also upregulates key hepatic transcription factors (SREBP-1) and the regulatory enzyme SCD-1, which converts saturated fatty acids into monounsaturated fatty acids.Citation36 This process enhances the biosynthesis of cholesterol esters and TG, leading to a reduced clearance rate due to lipase activity inhibition and increased mobilization of free fatty acids from adipose tissue.Citation37 Furthermore, IH may disrupt lipid metabolism by impairing very low-density lipoprotein (VLDL) clearance.Citation38
Furthermore, IH in OSAS activates Hypoxia Inducible Factor-1 (HIF-1), a key transcription factor. HIF-1, in turn, initiates pro-inflammatory transcription factors such as nuclear factor kappa B (NF-kB) and activates the NF-kB signaling pathway. This activation leads to an increased mobilization of pro-inflammatory cytokines, including tumor necrosis factor-alpha (TNF-α), IL-6, IL-8, CRP and PAI-1. Simultaneously, there is a decrease in anti-inflammatory factors like IL-10 in adipose tissue. This shift towards a pro-inflammatory state alters the metabolic activity of adipose tissue, resulting in metabolic dysfunction.Citation39,Citation40
These insights into the inflammatory mechanisms of OSAS underscore a complex interplay between hypoxia, inflammation and metabolic disruption. Future research should delve deeper into these pathways, particularly focusing on how they influence the metabolism or transport of LDL and ApoB. Understanding these mechanisms could be pivotal in unravelling the pathophysiology of OSAS and may pave the way for novel targeted therapeutic strategies.
OSAS and Adipokines
The prevalent co-occurrence of obesity in patients with OSAS has directed researchers’ attention towards adipokines, bioactive substances secreted by adipose tissue, known for their intricate roles in endocrine and metabolic processes. Our study aligns with the findings of Shazia Jehan et al, Zuleyha Bingol et al, and a meta-analysis by Xiaoyan Li, showing that OSAS is associated with elevated leptin levels and reduced leptin receptor levels.Citation17,Citation41–43 Prior research has indicated that plasma leptin levels in OSAS patients increase progressively with the severity of the condition and correlate strongly with the AHI and nocturnal oxygen saturation.Citation43 It is posited that chronic IH augments leptin signaling in the carotid body, predominantly through the action on the leptin receptor, thereby promoting hypoxic ventilatory responses. This leads to increased minute ventilation, reduced mechanical load on the upper airway, and stimulated compensatory neuromuscular responses.Citation44
Elevated leptin levels in OSAS patients have been likened to the hyperleptinemia observed in obesity, marked by a decreased expression of leptin receptors and a blunted response to leptin, indicative of leptin resistance.Citation45 John Ciriello’s animal study confirmed that long-term exposure to IH results in increased leptin levels and decreased leptin receptor expression, which impairs leptin’s action on target cells, disrupts sleep architecture, alters sympathetic nerve activity, and diminishes control over the genioglossus and adjacent muscles, crucial in managing upper airway obstruction.Citation46 Clinical studies have demonstrated that continuous positive airway pressure (CPAP) treatment in OSAS patients with obesity significantly ameliorates metabolic disorders related to leptin resistance, enhancing the body’s sensitivity to leptin, decreasing pharyngeal load, and improving pharyngeal ventilation.Citation47 However, it has also been observed that leptin levels may not significantly differ between OSAS patients and control groups, suggesting that the interplay between OSAS and leptin levels is complex and influenced by multiple factors, warranting further in-depth investigation.Citation48
Although the precise biological mechanisms underlying the elevation of leptin levels in OSAS remain elusive, sleep deprivation and hypoxemia are widely acknowledged as critical contributors. Research indicates that IH can lead to increased expression of the suppressor of cytokine signaling 3 protein in the arcuate hypothalamic nucleus. This is accompanied by a decrease in the protein levels of extracellular signal-regulated kinase 1/2 and an increase in the phosphorylation of ERK1/2. These changes collectively inhibit the activation of the leptin receptor signaling cascade, thus impeding the activation of leptin-related pathways (such as pro-opiomelanocortin), culminating in the development of leptin resistance.Citation47 The intricacies of leptin resistance, particularly the signaling process of the leptin receptor post blood-brain barrier traversal, are yet to be fully elucidated.Citation49
Furthermore, the recurrent apneic episodes characteristic of OSAS exacerbate hypoxemia and carbon dioxide accumulation, leading to heightened sympathetic nerve activity and diminished parasympathetic function. This physiological alteration stimulates the renin-angiotensin axis, promoting leptin production and secretion.Citation46 The resultant systemic leptin resistance contributes to the emergence of obesity, insulin resistance, metabolic syndrome and cardiovascular diseases. Leptin orchestrates the activation of signaling cascades including JAK/STAT, MAPK, IRS/PI3K/Akt pathways, concurrently augmenting the expression of atherogenesis-related cytokines and chemokines, thereby fostering vascular wall inflammation and perturbations in cellular functionality—pivotal elements in the pathogenesis of atherosclerosis.Citation50 Notwithstanding the prospective advent of central leptin resistance within the milieu of obesity and diabetes, the vascular milieu retains a pronounced or even amplified responsiveness to leptin, culminating in vascular dysfunction and expedited atherogenic progression.Citation51 Future investigations should focus on unraveling the specific mechanisms behind leptin resistance, evaluating its presentation across diverse populations, and exploring the potential effects of therapeutic interventions in ameliorating leptin resistance in OSAS. Such investigative efforts are crucial for advancing a more holistic comprehension of the pathophysiological intricacies of OSAS and potentially augmenting the effectiveness of its therapeutic approaches.
This study stands out for several notable strengths that enhance its contribution to the existing body of research on OSAS. Firstly, it pioneers the exploration of the causal relationships between OSAS and key health indicators—obesity, lipid levels, and adipokine levels—at the genetic level. Employing a bidirectional MR approach, our study effectively circumvents the confounding factors and measurement biases that are often inherent in observational studies. Secondly, our selection of genetic variants for IVs were informed by the most comprehensive GWAS data available. The chosen IVs, each with an F value exceeding 10, demonstrate a strong association with the exposure, lending credence to the reliability of our estimates and ruling out the influence of weak IVs. Thirdly, the robustness of our findings is further bolstered by a series of sensitivity analyses and thorough assessments for potential pleiotropy. These additional measures were instrumental in minimizing any possible biases in our results. Consequently, our findings provide substantial evidence to support the conclusion that OSAS contributes to an increase in NC, dyslipidemia, and disruptions in adipokine levels. These insights not only advance our understanding of OSAS but also underscore the significance of employing advanced genetic methodologies to unravel the complex interplay between this condition and various metabolic disturbances.
While this study significantly contributes to understanding the genetic correlates of obesity and OSAS, it is crucial to acknowledge its limitations. First and foremost, the absence of extensive GWAS data restricted our ability to conduct subgroup analyses based on variables such as gender, geographical location, and age. This limitation curtails the broader applicability and generalizability of our conclusions. Secondly, the primary reliance on data from European populations limits the extrapolation of our findings to non-European groups, given the known variations in gene expression and genetic predisposition among different ethnicities. The correlation between genetic markers and OSAS could significantly vary across different ethnic groups. Additionally, our study faced constraints due to insufficient SNP data on plasma adipokine levels. This limitation hampered our ability to perform a comprehensive IVW-based MR method analysis or in-depth sensitivity analysis, potentially overlooking certain biases. To address these issues and enhance the robustness of our findings, future studies should incorporate diverse and comprehensive GWAS data that spans various demographics and ethnicities. Such studies would not only validate and broaden our findings but also allow for a more detailed examination of the interactions between genetic predispositions to OSAS and other significant health outcomes, such as cardiovascular diseases. Given recent evidence indicating that obesity significantly elevates cardiovascular risk compared to OSAS, our research underscores the influence of OSAS on obesity-related factors. However, elucidating the subsequent impacts on cardiovascular health and specific biological pathways remains a critical gap.Citation4 Future research is essential to intricately analyze these factors and their mechanisms to fully comprehend their contributions to cardiovascular risk.
Conclusion
In conclusion, our study, utilizing MR analysis, has provided compelling genetic evidence establishing a definitive association between OSAS and key metabolic disturbances—namely, increased NC, dyslipidemia, and adipokine imbalances. These findings illuminate the potential genetic interplay between OSAS and metabolic syndrome, offering new avenues for research in this field. The evidence points towards a complex interaction between OSAS and various aspects of metabolic health, underscoring the necessity for further research. Future studies should aim to unravel the specific biological pathways through which OSAS influences metabolic syndrome. A deeper understanding of these mechanisms is crucial for the development of targeted preventive measures and therapeutic strategies.
Ethics Statement
This study utilizes aggregated data rather than individual-level data. The data involved all originate from publicly published GWAS summary databases, which complies with the conditions for exemption from review as stated in the “Ethical Review Measures for Life Sciences and Medical Research Involving Humans”.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
Data Sharing Statement
The datasets underpinning the conclusions drawn in this article are accessible through the IEU OpenGwas project repository. Interested readers and researchers can access these datasets at (https://gwas.mrcieu.ac.uk/).
Additional information
Funding
References
- Framnes SN, Arble DM. The Bidirectional Relationship Between Obstructive Sleep Apnea and Metabolic Disease. Front Endocrinol. 2018;9:440. doi:10.3389/fendo.2018.00440
- Xu X, Xu J. Effects of different obesity-related adipokines on the occurrence of obstructive sleep apnea. Endocr J. 2020;67(5):485–500. doi:10.1507/endocrj.EJ20-0036
- Behnoush AH, Bahiraie P, Shokri Varniab Z, Foroutani L, Khalaji A. Composite lipid indices in patients with obstructive sleep apnea: a systematic review and meta-analysis. Lipids Health Dis. 2023;22(1):84. doi:10.1186/s12944-023-01859-3
- Carratù P, Di Ciaula A, Dragonieri S, et al. Relationships between Obstructive Sleep Apnea Syndrome and cardiovascular risk in a naïve population of southern Italy. Int J Clin Pract. 2021;75(12):e14952. doi:10.1111/ijcp.14952
- Emdin CA, Khera AV, Kathiresan S. Mendelian Randomization. JAMA. 2017;318(19):1925–1926. doi:10.1001/jama.2017.17219
- Strausz S, Ruotsalainen S, Ollila HM, et al. Genetic analysis of obstructive sleep apnoea discovers a strong association with cardiometabolic health. Eur Respir J. 2021;57(5):56 doi:10.1183/13993003.03091-2020
- Li Y, Leng Y, Tang H, et al. Assessment of the Causal Effects of Obstructive Sleep Apnea on Atrial Fibrillation: a Mendelian Randomization Study. Front Cardiovasc Med. 2022;9:843681. doi:10.3389/fcvm.2022.843681
- Bowden J, Del Greco MF, Minelli C, Davey Smith G, Sheehan NA, Thompson JR. Assessing the suitability of summary data for two-sample Mendelian randomization analyses using MR-Egger regression: the role of the I2 statistic. Int J Epidemiol. 2016;45(6):1961–1974. doi:10.1093/ije/dyw220
- Burgess S, Thompson SG. Bias in causal estimates from Mendelian randomization studies with weak instruments. Stat Med. 2011;30(11):1312–1323. doi:10.1002/sim.4197
- Burgess S, Dudbridge F, Thompson SG. Combining information on multiple instrumental variables in Mendelian randomization: comparison of allele score and summarized data methods. Stat Med. 2016;35(11):1880–1906. doi:10.1002/sim.6835
- Burgess S, Thompson SG. Interpreting findings from Mendelian randomization using the MR-Egger method. Eur J Epidemiol. 2017;32(5):377–389. doi:10.1007/s10654-017-0255-x
- Tan JS, Liu N, Guo TT, Hu S, Hua L, Qian Q. Genetic Predispositions Between COVID-19 and Three Cardio-Cerebrovascular Diseases. Front Genet. 2022;13:743905. doi:10.3389/fgene.2022.743905
- Verbanck M, Chen CY, Neale B, Do R. Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nat Genet. 2018;50(5):693–698. doi:10.1038/s41588-018-0099-7
- Hemani G, Zheng J, Elsworth B, et al. The MR-Base platform supports systematic causal inference across the human phenome. Elife. 2018;7:34408. doi:10.7554/eLife.34408
- Onat A, Hergenç G, Yüksel H, et al. Neck circumference as a measure of central obesity: associations with metabolic syndrome and obstructive sleep apnea syndrome beyond waist circumference. Clin Nutr. 2009;28(1):46–51. doi:10.1016/j.clnu.2008.10.006
- Popadic V, Brajkovic M, Klasnja S, et al. Correlation of Dyslipidemia and Inflammation With Obstructive Sleep Apnea Severity. Front Pharmacol. 2022;13:897279. doi:10.3389/fphar.2022.897279
- Li X, He J. The Association Between Serum/Plasma Leptin Levels and Obstructive Sleep Apnea Syndrome: a Meta-Analysis and Meta-Regression. Front Endocrinol. 2021;12:696418. doi:10.3389/fendo.2021.696418
- Molnár V, Lakner Z, Molnár A, et al. The Predictive Role of the Upper-Airway Adipose Tissue in the Pathogenesis of Obstructive Sleep Apnoea. Life. 2022;12(10):543. doi:10.3390/life12101543
- Ho ML, Brass SD. Obstructive sleep apnea. Neurol Int. 2011;3(3):e15. doi:10.4081/ni.2011.e15
- Morrell MJ. Controlling for Obesity in Obstructive Sleep Apnea. Results from Dynamic Magnetic Resonance Imaging. Am J Respir Crit Care Med. 2018;198(11):1365–1366. doi:10.1164/rccm.201807-1257ED
- Arias-Tellez MJ, Acosta FM, Migueles JH, et al. Higher Physical Activity Is Related to Lower Neck Adiposity in Young Men, but to Higher Neck Adiposity in Young Women: an Exploratory Study. Int J Sport Nutr Exerc Metab. 2021;31(3):250–258. doi:10.1123/ijsnem.2020-0193
- Ucok K, Aycicek A, Sezer M, et al. Resting metabolic rate and anthropometric measurements in male sleep apnea patients. Intern Med. 2011;50(8):833–838. doi:10.2169/internalmedicine.50.4779
- Ucok K, Aycicek A, Sezer M, et al. Aerobic and anaerobic exercise capacities in obstructive sleep apnea and associations with subcutaneous fat distributions. Lung. 2009;187(1):29–36. doi:10.1007/s00408-008-9128-0
- Feng XW, Kang J, Wang ZF, Wang QY, Yu RJ. Regulation of hypothalamus-pituitary-adrenal axis and growth hormone axis in obstructive sleep apnea-hypopnea syndrome patients. Zhonghua Jie He He Hu Xi Za Zhi. 2006;29(4):230–232.
- Redolfi S, Yumino D, Ruttanaumpawan P, et al. Relationship between overnight rostral fluid shift and Obstructive Sleep Apnea in nonobese men. Am J Respir Crit Care Med. 2009;179(3):241–246. doi:10.1164/rccm.200807-1076OC
- Borel AL, Coumes S, Reche F, et al. Waist, neck circumferences, waist-to-Hip ratio: which is the best cardiometabolic risk marker in women with severe obesity? The SOON cohort. PLoS One. 2018;13(11):e0206617. doi:10.1371/journal.pone.0206617
- Karkinski D, Georgievski O, Dzekova-Vidimliski P, Milenkovic T, Dokic D. Obstructive Sleep Apnea and Lipid Abnormalities. Open Access Maced J Med Sci. 2017;5(1):19–22. doi:10.3889/oamjms.2017.011
- Liu D. High-Density Lipoprotein: From Biological Functions to Clinical Perspectives. Apolipoproteins, Triglycerides and Cholesterol. IntechOpen; 2020.
- Kollar B, Siarnik P, Hluchanova A, et al. The impact of sleep apnea syndrome on the altered lipid metabolism and the redox balance. Lipids Health Dis. 2021;20(1):175. doi:10.1186/s12944-021-01604-8
- Yadav R, France M, Aghamohammadzadeh R, et al. Impairment of high-density lipoprotein resistance to lipid peroxidation and adipose tissue inflammation in obesity complicated by obstructive sleep apnea. J Clin Endocrinol Metab. 2014;99(9):3390–3398. doi:10.1210/jc.2013-3939
- Düger M, Seyhan EC, Günlüoğlu MZ, et al. Does ischemia-modified albumin level predict severity of obstructive sleep apnea? Sleep Breath. 2021;25(1):65–73. doi:10.1007/s11325-020-02038-9
- Lavie L. Oxidative stress in obstructive sleep apnea and intermittent hypoxia--revisited--The bad ugly and good: implications to the heart and brain. Sleep Med Rev. 2015;20:27–45. doi:10.1016/j.smrv.2014.07.003
- Demirci-çekiç S, Özkan G, Avan AN, Uzunboy S, Çapanoğlu E, Apak R. Biomarkers of Oxidative Stress and Antioxidant Defense. J Pharm Biomed Anal. 2022;209:114477. doi:10.1016/j.jpba.2021.114477
- Kattoor AJ, Pothineni NVK, Palagiri D, Mehta JL. Oxidative Stress in Atherosclerosis. Curr Atheroscler Rep. 2017;19(11):42. doi:10.1007/s11883-017-0678-6
- Aluganti Narasimhulu C, Parthasarathy S. Preparation of LDL, Oxidation, Methods of Detection, and Applications in Atherosclerosis Research. Methods Mol Biol. 2022;2419:213–246. doi:10.1007/978-1-0716-1924-7_13
- Li J, Nanayakkara A, Jun J, Savransky V, Polotsky VY. Effect of deficiency in SREBP cleavage-activating protein on lipid metabolism during intermittent hypoxia. Physiol Genomics. 2007;31(2):273–280. doi:10.1152/physiolgenomics.00082.2007
- Drager LF, Tavoni TM, Silva VM, et al. Obstructive sleep apnea and effects of continuous positive airway pressure on triglyceride-rich lipoprotein metabolism. J Lipid Res. 2018;59(6):1027–1033. doi:10.1194/jlr.M083436
- Drager LF, Jun JC, Polotsky VY. Metabolic consequences of intermittent hypoxia: relevance to obstructive sleep apnea. Best Pract Res Clin Endocrinol Metab. 2010;24(5):843–851. doi:10.1016/j.beem.2010.08.011
- Keefe KR, Patel PN, Levi JR. The shifting relationship between weight and pediatric obstructive sleep apnea: a historical review. Laryngoscope. 2019;129(10):2414–2419. doi:10.1002/lary.27606
- Yang X, Zhang X, Yang W, et al. Gut Microbiota in Adipose Tissue Dysfunction Induced Cardiovascular Disease: role as a Metabolic Organ. Front Endocrinol. 2021;12:749125. doi:10.3389/fendo.2021.749125
- Jehan S, Zizi F, Pandi-Perumal SR, et al. Obstructive Sleep Apnea and Obesity: implications for Public Health. Sleep Med Disord. 2017;1(4).
- Bingol Z, Karaayvaz EB, Telci A, Bilge AK, Okumus G, Kiyan E. Leptin and adiponectin levels in obstructive sleep apnea phenotypes. Biomarker Med. 2019;13(10):865–874. doi:10.2217/bmm-2018-0293
- Imayama I, Prasad B. Role of Leptin in Obstructive Sleep Apnea. Ann Am Thorac Soc. 2017;14(11):1607–1621. doi:10.1513/AnnalsATS.201702-181FR
- Caballero-Eraso C, Shin MK, Pho H, et al. Leptin acts in the carotid bodies to increase minute ventilation during wakefulness and sleep and augment the hypoxic ventilatory response. J Physiol. 2019;597(1):151–172. doi:10.1113/jp276900
- Berger S, Polotsky VY. Leptin and Leptin Resistance in the Pathogenesis of Obstructive Sleep Apnea: a Possible Link to Oxidative Stress and Cardiovascular Complications. Oxid Med Cell Longev. 2018;2018:5137947. doi:10.1155/2018/5137947
- Ciriello J, Moreau JM, Caverson MM, Moranis R. Leptin: a Potential Link Between Obstructive Sleep Apnea and Obesity. Front Physiol. 2021;12:767318. doi:10.3389/fphys.2021.767318
- Giampá SQC, Furlan SF, Freitas LS, et al. Effects of CPAP on Metabolic Syndrome in Patients With OSA: a Randomized Trial. Chest. 2022;161(5):1370–1381. doi:10.1016/j.chest.2021.12.669
- Chihara Y, Akamizu T, Azuma M, et al. Among Metabolic Factors, Significance of Fasting and Postprandial Increases in Acyl and Desacyl Ghrelin and the Acyl/Desacyl Ratio in Obstructive Sleep Apnea before and after Treatment. J Clin Sleep Med. 2015;11(8):895–905. doi:10.5664/jcsm.4942
- Butiaeva LI, Slutzki T, Swick HE, et al. Leptin receptor-expressing pericytes mediate access of hypothalamic feeding centers to circulating leptin. Cell Metab. 2021;33(7):1433–1448.e5. doi:10.1016/j.cmet.2021.05.017
- Raman P, Khanal S. Leptin in Atherosclerosis: focus on Macrophages, Endothelial and Smooth Muscle Cells. Int J Mol Sci. 2021;22(11):5446. doi:10.3390/ijms22115446
- Damiani MF, Zito A, Carratù P, et al. Obstructive Sleep Apnea, Hypertension, and Their Additive Effects on Atherosclerosis. Biochem Res Int. 2015;2015:984193. doi:10.1155/2015/984193