
Abstract
Purpose
For knife-related injuries (KRI), a comprehensive understanding of the incidence, mechanism, and pattern of injury is required for the development of prevention strategies. Unfortunately, reliable data on knife-related injuries are difficult to obtain. In Egypt, there is no national routine surveillance system for all knife injuries. The aim was to examine the epidemiologic characteristics of knife-related injuries at the Ain Shams University Hospital (ASUH) emergency department (ED).
Patients and Methods
A cross-sectional study was conducted on 140 patients who presented with knife injuries at the ASUH ED. Data collection was done during a randomly selected period of seven days each month from October 2018 to September 2019. The sociodemographic characteristics, injury-related variables, and outcomes of the injury were recorded on a structured worksheet.
Results
Knife-related injuries represented 22.9% of all injury cases that presented to the ED. Majority of the knife-related injuries (87.86%) were accidental, 7.9% were assault, and 4.3% were self-inflicted. Home was the most reported place of injury. Most of the victims were discharged from the ED (87.1%), and 84.3% recovered completely. The mean hospital stay was 3.6 ± 1.3 days.
Conclusion
Majority of the knife-related injuries were accidental, and the most common pattern was isolated chest injury with contusions. Cases that were not severe and had favorable prognosis (ie, complete recovery) comprised the largest proportion. Recommendations include development of a surveillance system may result in the effective control and prevention of this growing problem of knife-related injuries.
Introduction
Injuries comprise the sixth leading cause of mortality globally and account for 9% of world deaths.Citation1 In low- to middle-income countries, about 90% of injury-related deaths are secondary to trauma.Citation2 Globally, emergency departments (EDs) have reported a rising incidence of knife-related injuries, both accidental and self-inflicted.Citation3,Citation4 In the UK, in 2011, knife injuries represented a quarter of all cases of major trauma and 94.1% of cases of major penetrating trauma. Other studies in the UK reported that assault knife injuries represented 10.3% of all trauma cases; this percentage increased to 12.9% between 2015 and 2018.Citation4,Citation5 About 80% of the injury-related deaths had been attributed to unintentional injuries, one of the leading causes of which was knife-related.Citation4,Citation6 Although assaults with sharp objects were relatively few, compared with the frequency of other intentional injuries, they represent a significant part of violent crime.Citation5,Citation7 Extensive availability of knives enables their frequent use in violent interpersonal conflicts. Compared with unintentional injuries, intentional or self-inflicted sharp-related injuries usually have different outcomes in terms of mortality and morbidity.Citation4,Citation8
Formulation of national policies and development of effective injury prevention strategies depend on a reliable, well-designed, and detailed trauma registry of the incidence and pattern of injury. Such data are available from the vital statistics registry and health-care records of developed countries, but these are usually unavailable or incomplete in developing countries.Citation9–Citation11 In Egypt, there is no national registry system for knife-related injuries. We carried out this study to define the epidemiologic characteristics of knife-related injuries at the ED of one of the major tertiary referral hospitals in Cairo, Egypt. This would be the bases for a national registry of knife related injuries.
Materials and Methods
Study Setting and Participants
The study was conducted from 2018 to 2019 at the ED of Ain Shams University Hospital (ASUH), which is one of the main tertiary hospitals in Cairo (the capital of Egypt and the most populated city of the country with around 10 million inhabitants). ASUH includes 2300 beds and is being operated by 9700 health professionals. As a teaching hospital, ASUH employs health professionals at all levels and in different specialties. Annually, ASUH caters to approximately 775,000 outpatient clinic visits and around 262,000 emergency cases. According to the Central Agency for Public Mobilization and Statistics (CAPMAS) health data in 2019, the annual number of the patients presenting to the ED of government hospital in Cairo Governorate was 837,446 patients. Thus, ASUH is receiving about one-third of the emergency cases on Cairo (31%).Citation12 Although it is one center study, it should represent Cairo which is the Capital and most populated city in Egypt.
This cross-sectional study included random selection of all knife-related injuries presented at the ASUH ED from October 1, 2018, to September 30, 2019. For logistic reasons, it was difficult to carry out 24/7 (24 hours for all the days of the month) observations of the ER. Moreover, collecting all patients with the high flow of cases in the ED will get too many cases beyond those required for the study. So, we decided to get 25% of the days of the year which ended up as 7 days per month. Data collection for the study period was done during a selected period of seven days in each month. Seven days were selected by simple random sample. Seven days per month represents 25% of the days of the month so our sample is 25% of the year.
Data were collected from the medical records of the patients except place of injury and method of transportation to the ASUH ED was collected from the patients as they were missing in the records. All cases were followed-up until discharge. The sample size was calculated based on the primary objective of estimating the prevalence of knife injuries among all trauma patients; this prevalence was assumed to be 25% based on previous studies. The 308 sample size of the trauma cases was calculated to estimate the expected prevalence with 5% margin of error, resulting in a 95% CI of 20–30%. From our experience at the ED, the daily rate of trauma cases was expected to be higher, compared with the estimated sample size during the defined period of data collection.
Data Collection Tools
A structured data collection sheet was designed to include three sections. Section 1 included the sociodemographic characteristics (ie, age, sex, education, occupation, and marital status) of the study participants. Section 2 included injury-related variables, such as time, place, mechanism, and pattern of injury; time of presentation to the ED; method of transportation to the hospital; associated injuries; and whether the injury was penetrating or vascular. Section 3 included the injury outcomes, such as disposition from the ED, stay in the ED, hospital stay in the inpatient ward, and long-term outcome. The data were collected from the records of the patients except place of injury and method of transportation to the ASUH ED were collected from the patients or their relatives as they were missing in the records. Data for sections 1 and 2 were obtained on admission, whereas those for section 3 were completed on discharge.
Statistical Analysis
Using SPSS version 24, the collected data were revised, entered into a spreadsheet, cleaned, and analyzed. Quantitative data were presented as mean and standard deviation with range. One-way ANOVA was used to compare the means of the groups. Categorical data were presented as number and the appropriate proportion. Chi-square test was used to compare the proportions of the groups. P value of ≤0.05 was considered statistically significant.
Results
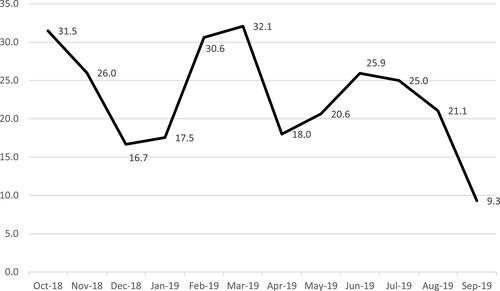
Of the 611 ASUH ED trauma cases that were reported in the sampled days, 140 (22.9%, 95% CI 19.6% to 26.2%) were knife-related injuries (KRI). As shown in , the proportion of KRI to all types of injuries varied significantly among the months, with the highest proportion in October, February, and March and the lowest in September. Eighty-two cases (58.6%) presented between 8:00 AM and 5:00 PM. The age range was 2–64 years, with mean of 30.0 ± 13.3 years. More than half of the victims (63.6%) were men. Married victims represented 54.3% (63/116), and 89.4% (118/132) had formal education.
Figure 1 Monthly proportion of knife injuries during the study period.
shows the basic characteristics of the KRI victims by the mechanism of injury. The three groups of accidental, assault, and self-inflicted injuries had no significant differences in the basic characteristics and month of occurrence or diurnal variation. The mean duration of transport from the accident site to the ED was 35.8 ± 16.5 mins (range, 10–90 mins). The majority were transported to the ED by private car or a taxi, and half were injured at home. Isolated chest injury was the pattern in more than half of the victims (52.9%). Penetrating injuries were reported in two patients, whereas four patients had major vascular injuries ().
Table 1 Baseline Characteristics by Mechanism of Knife Injury
Table 2 Description of Certain Aspects of the Knife Injury Among the Victims
Most of the victims (87.1%) were discharged from the ED. The patients were admitted to the operation theater (n = 7), inpatient ward (n = 3), or ICU (n = 1). The mean length of ED stay was 65.8 ± 39.0 mins (range, 15 mins to 5 hrs.). Majority of the victims (84.3%) recovered completely. Recovery with disability was recorded in 14 patients (10%), and only 1 patient died. The mean hospital stay for the admitted cases was 3.6 ± 1.3 days (range, 2–5 days) ().
Table 3 Clinical Outcome of the Victims of Knife Injury
Discussion
KRIs have become a growing public health problem.Citation3,Citation4 We examined the epidemiology of KRI at the ED of ASUH, which is one of the major referral hospitals in Cairo. In this one-year study, the case load of KRI at the ASUH ED was more than one-fifth (22.9%) of all 611 trauma cases. This rate was similar with the findings of Pallett et al in the UK in 2014 but was higher, compared with the results of another study by Malik et al in the region in 2020.Citation5 This can be explained by the fact that the latter included only violence-related KRI cases.
In this study, the highest proportion of cases occurred in October, February, and March. On the other hand, comparable studies in Ghana and Germany determined the highest mean incidence in December and July, respectively.Citation13,Citation14 This difference may be attributed to different geographical and cultural factors. Consistent with several studies that were conducted in Ghana, South Africa, Germany, UK, USA, and Korea,Citation13–Citation18 our study revealed that most of the patients were men. Moreover, the mean age of our study population was similar with those of previously published studies on penetrating trauma in the USA.Citation17,Citation19–Citation21 Most of our KRI cases were reported to be accidental, similar to the results of the previous study in China by Yin et al, who showed that 95.1% of the reported injuries were unintentional.Citation22 However, these results were much higher, compared with those of a comparable study in the UK, where only 52% of the KRIs were unintentional.Citation4 This difference may have been secondary to the different knife carrying habits and the marked increase in knife-related crimes in the UK.Citation23 In addition, in the USA and Italy, most of the sharp force injuries were intentional.Citation20,Citation21 The latter two studies analyzed fatal injuries that were secondary to only sharp force, whereas our study included all types of injuries with different severities. Also, the nature of the interpersonal violence between the Egyptian people is always using sticks and the knife is not the main tool used through the violence. However, the knife may be used by persons within the quarrel not intentionally aiming to kill the other people but to scare them and try to end the quarrel. So, the majority of the knife injuries were accidental and of a cut pattern within the chest not penetrating pattern. Also, the associated injuries were contusions, and this is due to the use of the sticks in the quarrel. This nature is different from the violence in other western countries as knife and gun shots are used frequently with higher probabilities of killing the others. So, the main pattern is of penetrating pattern and assault nature.
Similar to one study in India,Citation9 the present study showed that 58.6% of the cases presented to the ED between 8:00 AM and 5:00 PM. Moreover, home was the most common place of injury, similar to the observation in Korea, Romania, UK, and USA.Citation5,Citation8,Citation17,Citation24 Similar findings were reported in a community-based survey that involved 27 Egyptian governorates and included all injuries not only KRIs.Citation25 The most observed injury site was an isolated area in the chest, which was also observed in recent studies in Korea, Italy and USA.Citation15,Citation17,Citation21 In our study, most of the victims were discharged from the ED and the mean length of stay at the ED was similar to those reported in the UK and USA.Citation15,Citation17 The case fatality rate of 0.7% in this study was similar with those in Britain and Ghana.Citation4,Citation13 Moreover, the duration of hospital stay among our patients was similar with those in studies that were conducted in Korea and USA.Citation8,Citation17,Citation26
KRI comprises a considerable portion of the trauma load. Therefore, keeping a record system and development of a national surveillance system are important tools in the prevention and control of this problem. Important questions regarding the external, cultural, and geographical circumstances of the incidence of knife injuries all over Egypt remain unanswered. Therefore, it would be crucial to conduct a nationwide survey. In addition, this study did not analyze the prehospital deaths from KRIs. Further investigation is required to better understand the epidemiology of KRIs in Egypt.
The strength of our study was that it was conducted in a tertiary-level teaching hospital that served as a huge catchment area in Cairo. However, the study had some limitations. Data analyses from a referral hospital may have missed a considerable portion of cases that were managed at home, primary health care centers, and prevernal hospitals. In addition, data collection on the possible confounding factors, such as alcohol intoxication, drug abuse, and psychiatric illness, were not allowed by the administration for medicolegal reasons.
Conclusion
Our study demonstrated that more than one-fifth of the trauma load at the ED was accounted for by KRI, majority of which was accidental. Isolated chest and associated contusions comprised the most common pattern of injury. Most of the cases were not severe and had favorable prognosis of complete recovery.
Recommendations
We recommend conducting a multicenter survey in order to allow better representation of the epidemiology of KRI all over the country. On the other hand, the laws in Egypt should consider increasing the penalties for carrying of knifes to minimize the KRI.
Abbreviations
KRI, knife-related injuries; ASUH, the Ain Shams University Hospital; ED, emergency department.
Data Sharing Statement
Raw data are available from the corresponding author (Manar M. Ellaban) upon request.
Ethics Approval and Informed Consent
The institutional review boards of Ain Shams University, Cairo, Egypt (Date: September 17, 2017; Reference: 00006379) and the University of Maryland, Baltimore (Date: October 23, 2017; Reference: HP-00077613) approved this study. Data about place of injury and method of transportation to the ASUH ED were collected from the patients after obtaining an oral consent from the patients or their relatives. The verbal informed consent was approved by the institutional review boards, and that this study was conducted in accordance with the Declaration of Helsinki. The privacy rights of the patients were maintained.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Acknowledgments
The authors thank the managers of ASUH ED for enabling the research work and the support provided. We are also grateful to all the patients for their cooperation.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- WHO. Injuries and violence: the facts 2014; 2014. Available from: https://www.who.int/violence_injury_prevention/media/news/2015/Injury_violence_facts_2014/en/. Acssesed June 21, 2018.
- Wesson HKH, Boikhutso N, Bachani AM, Hofman KJ, Hyder AA. The cost of injury and trauma care in low- and middle-income countries: a review of economic evidence. Health Policy Plan. 2014;29(6):795–808. doi:10.1093/heapol/czt064
- Smith GA. Knife-related injuries treated in United States emergency departments, 1990–2008. J Emerg Med. 2013;45(3):315–323. Elsevier. doi:10.1016/j.jemermed.2012.11.092
- Pallett JR, Sutherland E, Glucksman E, Tunnicliff M, Keep JW. A cross-sectional study of knife injuries at a London major trauma centre. Ann R Coll Surg Engl. 2014;96(1):23–26. doi:10.1308/003588414X13824511649616
- Malik NS, Munoz B, de Courcey C, et al. Violence-related knife injuries in a UK city; epidemiology and impact on secondary care resources. EClinicalMedicine. 2020;20:100296. doi:10.1016/j.eclinm.2020.100296
- Bhuvaneswari N, Prasuna JG, Goel MK, Rasania SK. An epidemiological study on home injuries among children of 0–14 years in South Delhi. Indian J Public Health. 2018;62(1):4–9. doi:10.4103/ijph.IJPH_428_16
- Nair MS, Uzzaman MM, Al-Zuhir N, Jadeja A, Navaratnam R. Changing trends in the pattern and outcome of stab injuries at a North London hospital. J Emerg Trauma Shock. 2011;4(4):455–460. doi:10.4103/0974-2700.86628
- Ahn S, Kim DJ, Paik KY, et al. A comparison of self-inflicted stab wounds versus assault-induced stab wounds. Trauma Mon. 2016;21(5):e25304. doi:10.5812/traumamon.25304
- Swarnkar M, Singh PK, Dwivedi S. Pattern of trauma in central India: an epidemiological study with special reference to mode of injury. Internet J Epidemiol. 2010;9(1):1–7.
- Albabtain I, Alfehaid O, Alghunaim M, et al. Epidemiology of pediatric trauma at a tertiary hospital in Riyadh, Saudi Arabia. Int J Med Res Health Sci. 2019;8(11):101–107.
- Schreyer N, Carron PN, Demartines N, Yersin B. Stab wounds in a Swiss emergency department: a series of 80 consecutive cases. Swiss Med Wkly. 2010;140:w13058. doi:10.4414/smw.2010.13058
- CAPMAS. Egypt in numbers. health statistics. Available from: https://www.capmas.gov.eg/Pages/StaticPages.aspx?page_id=5035. Accessed October 30, 2021.
- Blankson PK, Amoako JKA, Asah-Opoku K, Odei-Ansong F, Lartey MY. Epidemiology of injuries presenting to the accident centre of Korle Bu teaching hospital, Ghana. BMC Emerg Med. 2019;19(1):39. doi:10.1186/s12873-019-0252-3
- Simanski C, Nienaber U, Lefering R, Pape-ko CIA. External factors and the incidence of severe trauma: time, date, season and moon. Injury. 2014;45:93–99.
- Kim MJ, Hong TH, Jung MJ, Lee SH, Lee JG. Single center experience of stab wound management. J Acute Care Surg. 2015;5(2):64–68. doi:10.17479/jacs.2015.5.2.64
- Marshall G, Lee DC, Wall S. Traumatic injury in the United States: in-patient epidemiology 2000–2011. Injury. 2017;47(7):1393–1403.
- Johannesdottir U, Jonsdottir GM, Johannesdottir BK, et al. Penetrating stab injuries in Iceland: a whole-nation study on incidence and outcome in patients hospitalized for penetrating stab injuries. Scand J Trauma Resusc Emerg Med. 2019;27(1):1. doi:10.1186/s13049-018-0582-2
- Kong V, Weale R, Blodgett J, et al. The spectrum of injuries resulting from abdominal stab wounds with isolated omental evisceration: a South African experience. Am J Surg. 2019;217(4):653–657. doi:10.1016/j.amjsurg.2018.06.003
- Olding J, Olding C, Bew D, Fan K. Penetrating head & neck trauma e epidemiology and injury characteristics in terror-related violence, interpersonal violence and deliberate self-harm at a level 1 trauma centre. Surgeon. 2019;17(3):133–138. doi:10.1016/j.surge.2019.01.001
- Kemal CJ, Patterson T, Molina DK. Deaths due to sharp force injuries in Bexar County, Texas, with respect to manner of death. Am J Forensic Med Pathol. 2013;34(3):253–259. doi:10.1097/PAF.0b013e31828ced68
- Vassalini M, Verzeletti A, De Ferrari F. Sharp force injury fatalities: a retrospective study (1982–2012) in Brescia (Italy). J Forensic Sci. 2014;59(6):1568–1574. doi:10.1111/1556-4029.12487
- Yin X, Li D, Zhu K, et al. Comparison of intentional and unintentional injuries among Chinese children and adolescents. J Epidemiol. 2020;30(12):529–536. doi:10.2188/jea.JE20190152
- StatisticsOo N police force area tables, crime in England&Wales, year ending. March, 2019. Available from: https://www.ons.gov.uk/peoplepopulationandcommunity/crimeandjustice/datasets/policeforceareadatatables. Accessed October 1, 2020.
- Gal M, Rus D, Peek-Asa C, et al. Epidemiology of assault and self-harm injuries treated in a large Romanian emergency department. Eur J Emerg Med. 2012;19(3):146–152. doi:10.1097/MEJ.0b013e32834ada2e
- Halawa EF, Barakat A, Rizk HII, Moawad EMI. Epidemiology of non-fatal injuries among Egyptian children: a community-based cross-sectional survey. BMC Public Health. 2015;15(1):1–9. doi:10.1186/s12889-015-2613-5
- Bugaev N, McKay K, Breeze JL, Arabian SS, Rabinovici R. Self-inflicted abdominal stab wounds have a higher rate of non-therapeutic laparotomy/laparoscopy and a lower risk of injury. World J Surg. 2017;41(11):2681–2688. doi:10.1007/s00268-017-4083-7