Abstract
Background
The purpose of this paper was to assess the feasibility of Micro-Mobile Compression® (MMC) on lactate clearance following exhaustive exercise and on subsequent exercise performance.
Methods
Elite male cyclists were randomized to MMC (n = 8) or passive recovery (control, n = 8). MMC is incorporated into a sandal that intermittently compresses the venous plexus during non-weight bearing to augment venous return. On day 1, subjects performed a graded exercise test on a cycle ergometer followed by 60 minutes of seated recovery, with or without MMC. Blood lactate concentration ([La−]) was measured during exercise and recovery. Subjects returned home for 3 more hours of seated recovery, with or without MMC. On days 2 and 3, subjects exercised to exhaustion in a fixed-load cycle ergometer test at 85% peak power and then repeated the day 1 post-exercise recovery procedures. Lactate clearance data after the time to exhaustion tests on days 2 and 3 were averaged to adjust for interday variation.
Results
On the day after MMC or control recovery, mean time to exhaustion was 15% longer (mean difference, 2.1 minutes) in the MMC group (P = 0.30). The standardized mean difference of MMC for time to exhaustion was 0.55, defined as a moderate treatment effect. Following the graded exercise test, area under the 60-minute lactate curve was nonsignificantly lower with MMC (3.2 ± 0.4 millimolar [mM]) versus control (3.5 ± 0.4 mM, P = 0.10) and times from end of exercise to 4mM and 2mM were 2.1 minutes (P = 0.58) and 7.2 minutes (P = 0.12) shorter, although neither achieved statistical significance. Following time to exhaustion testing, the area under the 60-minute lactate curve was lower with MMC (3.2 ± 0.2 mM) versus control (3.5 ± 0.2 mM, P = 0.02) and times from end of exercise to 4mM and 2mM were 4.4 minutes (P = 0.02) and 7.6 minutes (P < 0.01) faster. The standardized mean difference of MMC on most lactate clearance parameters was >0.8, defined as a large treatment effect.
Conclusion
MMC yields large treatment effects on lactate clearance following high-intensity exercise and moderate treatment effects on subsequent exercise performance in elite male cyclists.
Introduction
Strenuous exercise elicits important stresses on the musculoskeletal system and metabolic functions that can impair subsequent exercise performance and interfere with training practices. Fluxes in muscle cell metabolites associated with energy utilization during heavy exercise (eg, lactate) can delay recovery influence muscle glycogen reserves, and in some circumstances, contribute to transient decreases in subsequent exercise performance. Active recovery is a highly beneficial and advantageous training strategy compared with passive recovery since augmented post-exercise circulation encourages lactate clearance and, in some cases, may enhance subsequent exercise performance.Citation1–Citation7 Recent studies have reported mixed findings on exercise performance following active recovery with compression garmentsCitation8–Citation11 or whole body vibration.Citation12–Citation14 Additionally, compliance with compression garments is generally poorCitation9 and the availability of whole body vibration units is limited to research use.
Micro-Mobile Compression® (MMC) is a novel technology that simulates the effects of active recovery by augmenting blood flow through the deep veins of the leg via cyclic pressure pulses to the plantar venous plexus. The platform for MMC is a sandal that provides cyclic compression to the arch of the foot when the user is in a non-weight bearing position. Dohm et alCitation15 reported that MMC augmented blood flow velocity 12-fold above resting levels in the posterior tibial vein and four-fold above resting levels in the popliteal vein of healthy adults. A distinct theoretical advantage of MMC is that post-exercise circulation and lactate clearance may be augmented without the deleterious effects of decreased glycogen resynthesis in type I muscle fibers,Citation16 lower muscle reoxygenation rates,Citation17 and declines in subsequent exercise performanceCitation17,Citation18 that have been reported in some studies of traditional exercise-based active recovery. The hypothesis of this randomized, controlled trial was that MMC would allow for enhanced clearance of blood lactate immediately following exhaustive exercise and an improvement in subsequent high-intensity, fixed-load exercise performance.
Materials and methods
Subjects
This prospective, randomized, controlled trial was conducted at the Human Performance Laboratory of the Anschutz Health and Wellness Center at the University of Colorado School of Medicine, Aurora, CO, USA. All study procedures were conducted in accordance with the Declaration of Helsinki and in accordance with a predefined protocol that was approved by all researchers and the Colorado Multiple Institutional Review Board. All participants gave informed consent before any study procedures were performed.
Eligible subjects were 16 elite (Pro/category 1/category 2) male road cyclists, aged 21–42 years. Consecutive eligible subjects were randomly assigned to MMC or passive recovery only (control) using a computerized random-number generator with a 1:1 allocation ratio and a block size of four. Treatment assignments were hidden from investigators and subjects via sealed and secured envelopes until each subject was randomized. Blinding of interventions was not feasible in this study.
Interventions
Cycle ergometry graded exercise test
Subjects were instructed to have adequate sleep the night before the test and to avoid food, alcohol, tobacco, and caffeine within 3 hours of the test. Each subject was provided with nutrition recommendations for the 3 days prior to exercise testing as well as during the 3-day experimental period. The dietary recommendations were consistent each day, and included complete abstinence from alcohol and consumption of a diet with 70% of calories from carbohydrate, 15% from protein, and 15% from fat.
Subjects performed a graded exercise test to exhaustion on a calibrated, electrically braked cycle ergometer (Lode Excalibur Sport, Lode, Groningen, The Netherlands) on day 1. Subjects performed an incremental test according to our protocol,Citation19 which was slightly modified for this study. The initial workload was 2 W/kg, with increments of 0.5 W/kg every 3 minutes until volitional exhaustion. Maximal oxygen consumption (VO2max), blood lactate concentration ([La−]), heart rate, and power output were measured during the graded exercise test. Oxygen consumption (VO2), carbon dioxide production (VCO2), ventilation, and respiratory exchange ratio were determined through indirect calorimetry (ParvoMedics TrueOne 2400 Metabolic Measurement System, ParvoMedics Inc, Sandy, UT, USA). Criteria for attainment of VO2max included two of the following: respiratory exchange ratio >1.1, maximal heart rate within 10 beats per minute of the calculated value, or an O2 plateau (<50 mL per minute) with an increase in power output. Heart rate was continuously monitored with a heart monitor (Polar S725x, Polar Electro, Kempele, Finland). At the end of each stage, a sample of capillary blood (25 μL) from the earlobe was collected to analyze both intracellular and extracellular levels of L-lactate (YSI 1500 Sport, YSI, Yellow Springs, OH, USA).
Time to exhaustion
On days 2 and 3 at the same time of day, subjects performed a fixed-load exercise test at 85% of peak power output (power outputPeak) determined on day 1, on the electrically braked cycle ergometer. Pretest procedures were identical to those of the graded exercise test. Subjects were requested to maintain the prescribed power output during exercise until volitional exhaustion. Gas exchange and heart rate were measured identically to day 1. [La−] was measured only at the end of exercise.
Exercise recovery procedures
On each of the 3 days after the exercise tests were completed, subjects recovered by sitting barefooted in the laboratory for 60 minutes, with or without MMC. Blood was collected at 10-minute intervals throughout the 60-minute recovery period. Participants ingested a sports drink containing 1.5 g/kg of carbohydrates during recovery. Thereafter, subjects returned to their residences and immediately completed an additional 3 hours of seated passive recovery, with or without MMC. The post-exercise recovery procedures were identical on each day.
Micro-Mobile compression
The MMC device (AVEX, LLC, Grand Junction, CO, USA, ) consists of a motorized thrusting arm and pressure pad powered by a long-lasting rechargeable battery. The unit is user-activated by depressing a power switch on the body of the motor, which is housed in a hollow within the sole of a custom sandal. Upon activation, the device thrusts an 18.6 cm2 pressure pad directly onto the sole of the foot, compressing the plantar venous plexus. The MMC device adjusts the height of its thrust until the exerted pressure on the arch of the foot reaches a measured force of 3.76 N/cm2. The thrusting pad remains pressed on the arch of the foot for 2 seconds before retreating to its resting position. This thrust-pause-retreat cycle repeats every 20 seconds while the wearer is non-weight bearing. A pressure-sensitive interrupt switch is activated if the wearer stands up. The MMC device returns to its cyclical thrusting rhythm after 60 seconds of wearer inactivity.
Figure 1 The Micro-Mobile compression® device. External (left) and long-axis cross sectional (right) views. Activation switch and pressure pad in raised position shown in right panel.

Data analysis
Lactate clearance data after the time to exhaustion tests on days 2 and 3 were averaged to adjust for interday variationCitation20 and between-group comparisons were adjusted for peak lactate concentration using analysis of covariance. The correlation of time to exhaustion on days 2 and 3 was high (r = 0.78). The area under the lactate curve during the 60-minute post-exercise recovery period was computed using the trapezoidal rule described by Matthews et al.Citation21 To calculate the time needed for peak lactate to reach fixed markers of lactate clearance, individual blood [La−] values were plotted at each time point during the 60-minute recovery period using a smoothed curve fitting model (Microsoft Excel, 2010, Redmond WA, USA). Two fixed time points on each plotted lactate clearance curve were identified ie, the time for lactate concentration to decline from peak to 4 mM ([La−]4mM) and 2 mM ([La−]2mM), respectively.
Time to exhaustion data on days 2 and 3 were averaged to adjust for interday variation,Citation20 and values were assessed with analysis of variance to compare the MMC and control groups. Analysis of covariance was explored to assess the potential influence of baseline characteristics and graded exercise test data. None of these variables influenced the effect of treatment group on time to exhaustion and therefore, unadjusted data are reported.
Statistical significance was set at P < 0.05. Continuous variables were reported as the mean ± standard deviation. Baseline subject characteristics and graded exercise test data were compared using an independent-samples t-test. For each main outcome, the mean between-group difference and 95% confidence interval (CI) were calculated. The standardized mean difference was also calculated for each variable, defined as the between-group mean difference divided by the common standard deviation. For reference, a standardized mean difference of 0.2 is considered small, 0.5 is moderate, 0.8 is large, and 1.0 is very large.Citation22 The sample size in this study allowed the detection of a standardized mean difference > 1.5, assuming two-sided alpha = 0.05, statistical power = 80%, and a 1:1 allocation ratio. All statistical tests were performed using NCSS software, version 7.1.21 (NCSS, LLC, Kaysville, UT, USA).
Results
Subject compliance
All subjects completed the 3-day testing period, and compliance with the testing protocol and dietary recommendations was 100%. No discomfort or complications were reported in subjects allocated to MMC or control.
Subject characteristics
Subject characteristics included a mean age of 29 ± 5 (range 21–42) years, body mass index of 21.7 ± 1.9 kg/m2, VO2max of 60 ± 6 mL/kg per minute, and peak power of 349 ± 40 W. The MMC and control groups did not differ in baseline characteristics () or in responses to the cycle ergometer graded exercise test ().
Table 1 Baseline subject characteristics
Table 2 Exercise capacity measures from cycle ergometer graded exercise test
Time to exhaustion with high-intensity, fixed-load ergometry
On the day after exhaustive exercise followed by MMC or control recovery, mean time to exhaustion with high-intensity, fixed-load cycling was 15% greater (mean difference 2.1 minutes, 95% CI −2.1 to 6.3) in the MMC group (16.2 ± 4.9 minutes) versus control (14.1 ± 2.6 minutes), although statistical significance was not achieved (P = 0.30). The standardized mean difference of MMC on time to exhaustion was 0.55, representing a moderate effect.
Lactate clearance after graded exercise testing
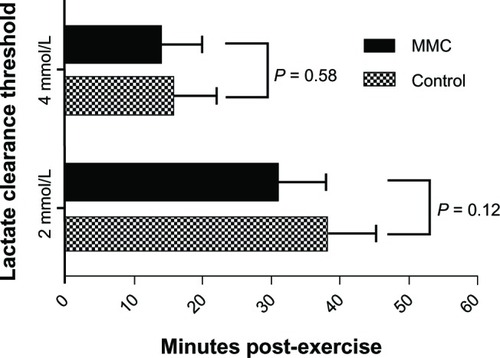
Following the graded exercise test, the area under the 60-minute lactate curve was nonsignificantly lower with MMC (3.2 ± 0.4 mM) versus control (3.5 ± 0.4 mM, mean difference 95% CI −0.8 to 0.1 mM, P = 0.10), indicating somewhat faster lactate clearance with MMC (). The mean time required for lactate concentration to fall from peak exercise to [La−]4mM was 2.1 minutes shorter with MMC versus control (mean difference 95% CI −5.8 to 9.9 minutes, P = 0.58). Similarly, the mean time for [La−] to fall from peak exercise to [La−]2mM was 7.2 minutes shorter with MMC versus control (mean difference 95% CI −2.0 to 16.4 minutes, P = 0.12, ). Despite the lack of statistically significant group differences, the standardized mean difference of MMC on lactate clearance parameters after graded exercise test was 0.88 (large effect) for the area under the 60-minute lactate curve, 0.29 (small effect) for time from peak to [La−]4mM, and 0.85 (large effect) for time from peak to [La−]2mM.
Figure 2 Area under the 60-minute lactate curve after graded exercise test. P-value represents the difference in 60-minute area under the lactate curve with MMC versus control. Plotted values are means.
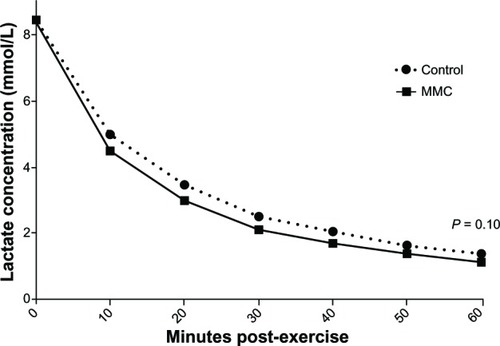
Figure 3 Lactate clearance time to 4 mM and 2 mM thresholds after graded exercise test. Values are means ± 95% confidence intervals.
Lactate clearance after high-intensity, fixed-load ergometry
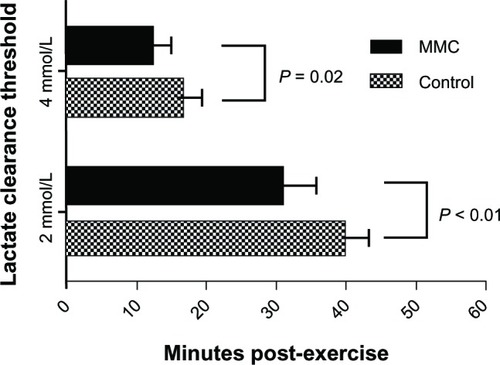
Following time to exhaustion testing, the area under the 60-minute lactate curve was lower with MMC (3.2 ± 0.2 mM) versus control (3.5 ± 0.2 mM, mean difference 95% CI −0.1 to −0.5 mM, P = 0.02, ). The time from peak to [La−]4mM was 4.4 minutes faster with MMC versus control (mean difference 95% CI −0.9 to −7.9 minutes, P = 0.02) and time to [La−]2mM was 7.6 minutes faster with MMC versus control (mean difference 95% CI −3.0 to −12.2 minutes, P < 0.01, ). The standardized mean difference of MMC on all lactate clearance parameters after time to exhaustion tests was > 1.0, representing very large effects.
Figure 4 Area under the 60-minute lactate curve after fixed-load cycle ergometry at 85% peak power. P-value represents the difference in 60-minute area under the lactate curve with MMC versus control. Plotted values are means.
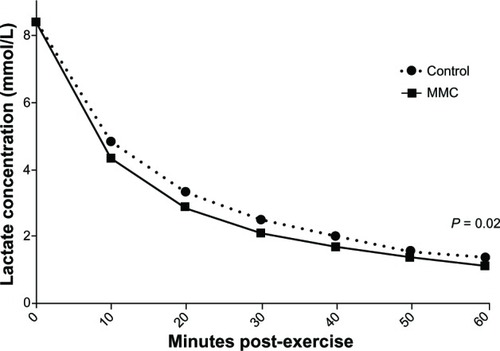
Figure 5 Lactate clearance time to 4 mM and 2 mM thresholds after fixed-load cycle ergometry at 85% peak power. Values are means ± 95% confidence intervals.
Discussion
The major findings of this randomized controlled trial are that application of MMC results in faster clearance of blood lactate following high-intensity exercise and yields moderate improvements in subsequent exercise performance in elite male cyclists. Although statistical significance was not achieved for all lactate clearance and performance parameters, calculated treatment effects were moderate to very large in most cases, despite the fact that the study was underpowered for some outcomes. This study represents the first published report on the potential applicability of MMC for enhancement of athletic performance.
Blood lactate testing is extensively utilized in the field of applied exercise physiology and sports performance. It is well documented that highly trained athletes accumulate lower blood lactate levels,Citation23–Citation28 probably due to an enhanced lactate clearance capacity.Citation29 Lactate concentration at submaximal exercise intensities has discriminative ability to predict performance in competitive cyclists.Citation19 Early in recovery, following high-intensity, fixed-load exercise that elicits high blood lactate accumulations, as in our study, enhanced lactate removal may aid recovery by a number of metabolic processes, including facilitating conversion to glucose in the liver and increasing substrate availability for many organs in the body, including the heart, brain, and less active skeletal muscle.Citation29,Citation30 Various types of active recovery following intense exercise have been shown to improve lactate removal.Citation1–Citation6,Citation31–Citation34 Further, active exercise recovery after strenuous exercise clears accumulated blood lactate in an intensity-dependent manner faster than passive recovery.Citation35 These effects are probably due to increased lactate efflux from active muscle, promoted by enhancing local blood flow and flow-related oxygen delivery, with little or no attendant increase in metabolic demand caused by the mode of active recovery employed. It is also plausible that effective forms of active recovery, in addition, may be instrumental in helping fatigued muscle shift metabolic processes more quickly in ways that shorten the time needed to replenish glycogen stores for heavy exercise training or competition on subsequent days.
Prior studies with MMC have yielded outcomes that are supportive of our findings. Dohm et alCitation15 demonstrated that MMC yields venous velocity increases 12-fold above resting levels for the posterior tibial artery and four-fold for the popliteal artery, which were comparable with the peak venous velocities demonstrated with an intermittent pneumatic compression system approved by the US Food and Drug Administration. Charles et alCitation36 compared MMC and below-knee graduated compression stockings on peak venous velocity at the popliteal vein. MMC yielded a four-fold increase in peak venous velocity versus no change for compression stockings. Based on the pronounced venous augmentation observed with MMC in these studies, the beneficial influence of MMC on lactate clearance in the current study was not surprising. In fact, all lactate clearance parameters in this study were associated with a large or very large standardized mean difference, with the exception of [La−]4mM following the graded exercise test. Given that the time from peak lactate to [La−]4mM was approximately 15 minutes, it is plausible that a greater duration of MMC is required to elicit maximal benefit on lactate clearance.
The exercise performance treatment effect in the current study was of such a magnitude to suggest moderate performance enhancement with exercise or competition on consecutive days, thereby warranting additional larger scale studies. However, the mechanism by which MMC influences subsequent exercise performance is unknown. Venous plexus compression is known to exert shearing stress on the endothelial lining yielding nitric oxide-mediated vasodilation,Citation37 which is known to regulate the microcirculation in upstream muscleCitation38 and to influence glycogen replenishment rates.Citation39 Animal studies demonstrate that intermittent pneumatic leg compressions improve exercise tolerance, in part, by enhancing blood flow to collateral-dependent tissues.Citation40 Additionally, muscle damage indices such as creatine kinase concentrationCitation41 and lymphatic outflow kineticsCitation42 have been explored as possible mediators of exercise performance on consecutive days with compression clothing or devices. These markers are candidates for further study in order to determine the mechanism by which MMC influences subsequent exercise performance.
This study had several limitations worth mentioning. First, despite the promising lactate clearance outcomes with MMC over 60 minutes post-exercise, we did not assess exercise performance during this period. Instead, we focused on exercise performance the day after MMC, a design that is applicable to cyclists participating in intensive training on consecutive days or those competing in multiple-day stage races. Second, the sample size was sufficient only to detect large treatment effects compared with passive recovery. We therefore calculated the standardized mean difference of treatment effects to supplement formal hypothesis tests. Next, no formal comparisons with other active recovery methods were integrated into this study design. The results of this study are generalizable only to competitive male cyclists and, therefore, extrapolation of the study outcomes to females or to non-cyclist endurance athletes should be done with caution. Finally, it is plausible that the wide range of subject ages may have confounded recovery from exercise, despite the fact that no differences in age were identified between groups.
Conclusion
This randomized, controlled trial demonstrated that MMC augments clearance of blood lactate following high-intensity exercise and moderately improves subsequent exercise performance in elite male cyclists. Larger, prospective, randomized, controlled trials are warranted to evaluate further the effect and mechanism of action of MMC technology on exercise performance and recovery.
Acknowledgments
The authors thank William G Herbert for research and editorial assistance.
Disclosure
This research was supported in part by AVEX LLC (Grand Junction, CO, USA).
References
- AhmaidiSGranierPTaoutaouZMercierJDubouchaudHPrefautCEffects of active recovery on plasma lactate and anaerobic power following repeated intensive exerciseMed Sci Sports Exerc19962844504568778550
- BelcastroANBonenALactic acid removal rates during controlled and uncontrolled recovery exerciseJ Appl Physiol1975396932936765313
- DoddSPowersSKCallenderTBrooksEBlood lactate disappearance at various intensities of recovery exerciseJ Appl Physiol1984575146214656520040
- GisolfiCRobinsonSTurrellESEffects of aerobic work performed during recovery from exhausting workJ Appl Physiol1966216176717725929302
- HermansenLStensvoldIProduction and removal of lactate during exercise in manActa Physiol Scand19728621912014640170
- SpiererDKGoldsmithRBaranDAHryniewiczKKatzSDEffects of active vs passive recovery on work performed during serial supramaximal exercise testsInt J Sports Med200425210911414986193
- KoizumiKFujitaYMuramatsuSManabeMItoMNomuraJActive recovery effects on local oxygenation level during intensive cycling boutsJ Sports Sci201129991992621574096
- SperlichBBornDPKaskinoroKKalliokoskiKKLaaksonenMSSqueezing the muscle: compression clothing and muscle metabolism during recovery from high intensity exercisePLoS One201384e6092323613756
- MacRaeBACotterJDLaingRMCompression garments and exercise: garment considerations, physiology and performanceSports Med2011411081584321923201
- HamlinMJMitchellCJWardFDDraperNShearmanJPKimberNEEffect of compression garments on short-term recovery of repeated sprint and 3-km running performance in rugby union playersJ Strength Cond Res201226112975298223007487
- de GlanvilleKMHamlinMJPositive effect of lower body compression garments on subsequent 40-km cycling time trial performanceJ Strength Cond Res201226248048622240553
- KosarACCandowDGPutlandJTPotential beneficial effects of whole-body vibration for muscle recovery after exerciseJ Strength Cond Res201226102907291122130390
- ColsonSSPetitPDLower limbs power and stiffness after whole-body vibrationInt J Sports Med201334431832323143701
- MarinPJHerreroAJMiltonJGHazellTJGarcia-LopezDWhole-body vibration applied during upper body exercise improves performanceJ Strength Cond Res20132771807181223085972
- DohmMWilliamsKMNovotnyTMicro-mobile foot compression device compared with pneumatic compression deviceClin Orthop Relat Res201146961692170021403988
- FairchildTJArmstrongAARaoALiuHLawrenceSFournierPAGlycogen synthesis in muscle fibers during active recovery from intense exerciseMed Sci Sports Exerc200335459560212673142
- OhyaTAramakiYKitagawaKEffect of duration of active or passive recovery on performance and muscle oxygenation during intermittent sprint cycling exerciseInt J Sports Med201334761662223325717
- DupontGBlondelNBerthoinSPerformance for short intermittent runs: active recovery vs passive recoveryEur J Appl Physiol200389654855412734760
- San MillánIGonzalez-HaroCSagastiMPhysiological differences between road cyclists of different categoriesMed Sci Sports Exerc200941S48
- FricJJrFricJBoldtFReproducibility of post-exercise lactate and anaerobic thresholdInt J Sports Med1988953103123246463
- MatthewsJNAltmanDGCampbellMJRoystonPAnalysis of serial measurements in medical researchBMJ199030067192302352106931
- CohenJStatistical Power Analysis for the Behavioral Sciences2nd edHillsdale, NJLawrence Erlbaum1988
- DonovanCMBrooksGAEndurance training affects lactate clearance, not lactate productionAm J Physiol19832441E83E926401405
- HurleyBFHagbergJMAllenWKEffect of training on blood lactate levels during submaximal exerciseJ Appl Physiol1984565126012646725086
- JanssonEKaijserLSubstrate utilization and enzymes in skeletal muscle of extremely endurance-trained menJ Appl Physiol198762399910053571098
- KjaerMBangsboJLortieGGalboHHormonal response to exercise in humans: influence of hypoxia and physical trainingAm J Physiol19882542 Pt 2R197R2032830794
- MacRaeHSDennisSCBoschANNoakesTDEffects of training on lactate production and removal during progressive exercise in humansJ Appl Physiol1992725164916561601768
- BergmanBCWolfelEEButterfieldGEActive muscle and whole body lactate kinetics after endurance training in menJ Appl Physiol19998751684169610562610
- BrooksGACell-cell and intracellular lactate shuttlesJ Physiol2009587Pt 235591560019805739
- GladdenLBLactic acid: new roles in a new millenniumProc Natl Acad Sci U S A200198239539711209043
- KraemerWJFlanaganSDComstockBAEffects of a whole body compression garment on markers of recovery after a heavy resistance workout in men and womenJ Strength Cond Res201024380481420195085
- TaoutaouZGranierPMercierBMercierJAhmaidiSPrefautCLactate kinetics during passive and partially active recovery in endurance and sprint athletesEur J Appl Physiol Occup Physiol19967354654708803508
- BonenABelcastroANComparison of self-selected recovery methods on lactic acid removal ratesMed Sci Sports197683176178979565
- MonederoJDonneBEffect of recovery interventions on lactate removal and subsequent performanceInt J Sports Med200021859359711156281
- MenziesPMenziesCMcIntyreLPatersonPWilsonJKemiOJBlood lactate clearance during active recovery after an intense running bout depends on the intensity of the active recoveryJ Sports Sci201028997598220544484
- CharlesTMacintoshSFingletonJWeatherallMBeasleyREfficacy of micro-mobile foot compression device in increasing lower limb venous blood flowInt J Vasc Med
- BryanNSApplication of nitric oxide in drug discovery and developmentExpert Opin Drug Discov20116111139115422646983
- ChenLELiuKQiWNRole of nitric oxide in vasodilation in upstream muscle during intermittent pneumatic compressionJ Appl Physiol200292255956611796664
- DaiZWuZYangYNitric oxide and energy metabolism in mammalsBiofactors201339438339123553707
- RoseguiniBTArce-EsquivelAANewcomerSCYangHTTerjungRLaughlinMHIntermittent pneumatic leg compressions enhance muscle performance and blood flow in a model of peripheral arterial insufficiencyJ Appl Physiol201211291556156322362398
- CochraneDJBookerHRMundelTBarnesMJDoes intermittent pneumatic leg compression enhance muscle recovery after strenuous eccentric exercise?Int J Sports Med4192013 [Epub ahead of print.]
- KraemerWJBushJAWickhamRBContinuous compression as an effective therapeutic intervention in treating eccentric-exercise induced muscle sorenessJ Sport Rehabil2001101123