
Abstract
Purpose
The aim of this study was to compare stereoacuity before and after KAMRA corneal inlay implantation for the correction of presbyopia.
Patients and methods
This is a prospective study of 60 patients who underwent KAMRA inlay implantation. Patients were examined before and 6 months after surgery for stereoacuity, uncorrected distance visual acuity (UDVA), and uncorrected near visual acuity (UNVA).
Results
The mean stereoacuity before surgery was 29.5±28.1 arcsec (range: 20–200) and at 6 months was 29.8±26.4 arcsec (range: 20–200). The decline in stereoacuity was not statistically significant. At 6 months follow-up, UDVA was 20/25 or better in all 60 patients and UNVA was J2 (20/25) or better in 51 (85%) patients.
Conclusion
There is no significant change in stereoacuity following KAMRA inlay implantation. The KAMRA inlay is a good treatment option for improving near vision in presbyopic patients while preserving stereoacuity and distance vision.
Introduction
Stereopsis, or the perception of depth, is a higher level of visual function produced by the brain as it receives visual stimuli from both eyes. Stereoacuity is the smallest measurable difference in depth detected with binocular vision and is reported in arc seconds (1/3,600 of a degree). Smaller numerical values correlate with better stereoacuity and greater depth perception. Impaired stereoacuity may significantly impact daily visuomotor tasks, even in the setting of excellent visual acuity. Recently, the KAMRA corneal inlay (AcuFocus, Inc.) has become a popular surgical option for the treatment of presbyopia. The KAMRA inlay is a small disk that is placed within the corneal stroma of the non-dominant eye. Utilizing the principle of pinhole optics, it increases the depth of focus and improves near vision. Multiple studies have shown the KAMRA inlay to be a safe and effective device.Citation1–Citation3 Change in stereoacuity has previously been investigated for treatments of presbyopia, such as monovision laser in situ keratomileusis (LASIK) and monovision contact lenses.Citation4,Citation5 However, in this work, we compare the stereoacuity of patients before and after KAMRA inlay implantation.
Patients and methods
This is a prospective study of 60 patients who underwent KAMRA inlay implantation for the correction of presbyopia at our institution between October 2009 and June 2010. Analyses performed for this study were part of routine postoperative data collection, and written informed consent was provided by all patients to have their data used for research purposes. An institutional review board approval was not obtained for this study according to the Office for Human Research Protection/Recommended Guidance on Minimal Risk Research and Informed Consent (45 CFR 46.102.i). The mean age was 53 (range: 45–60). Inclusion criteria included a spherical equivalent between +0.50 and −0.75, a monocular uncorrected near visual acuity (UNVA) worse than 20/40 and better than 20/100, and a monocular corrected distance visual acuity (CDVA) of 20/20 or better. Stereoacuity was measured using the Optec 5000 Visual Screener (Stereo Optical Co., Inc., Chicago, IL, USA). The surgical technique and third-generation KAMRA inlay used in this study have previously been described.Citation1,Citation2 Patients were examined before and 6 months after KAMRA inlay implantation for stereoacuity, uncorrected distance visual acuity (UDVA), and UNVA. Statistical analysis and figure production were accomplished using Microsoft Excel 2016 (Microsoft Corporation, Redmond, WA, USA). Statistical significance was determined using a Wilcoxon signed-rank test for paired samples, with a P-value of ≤0.05.
Results
In this study, the mean stereoacuity preoperatively and 6 months postoperatively was 29.5±28.1 arcsec (range: 20–200) and 29.8±26.4 arcsec (range: 20–200), respectively. There was a mean difference between preoperative and postoperative groups of −0.3±19.0 arcsec (range: −50 to 80), which was not statistically significant (P=0.60). Thirty-six (60%) patients had no change in stereoacuity, 9 (15%) patients had improved stereoacuity (range: 10–80), and 15 (25%) patients had worsened stereoacuity (range: −5 to −50). For unknown reasons, one patient had a stereoacuity of 200 arcsec before implantation. However, this patient had no change in stereoacuity after surgery. Preoperatively, this cohort had a mean UDVA of 20/20 (logMAR −0.04±0.09) and UNVA of J7 (20/60, logMAR 0.47±0.06). At 6 months follow-up, the mean UDVA was 20/20 (logMAR −0.04±0.07), and UNVA was J2 (20/25, logMAR 0.06±0.07).
Discussion
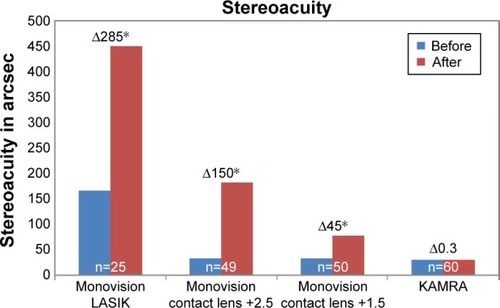
Stereopsis is an important visual function to determine both position and distance. Following monovision treatment for presbyopia, some patients complain of poor visual outcomes despite great binocular visual acuity. Diminished stereoacuity may be a contributing factor to their discontent. In this study, we report a negligible change in stereoacuity following implantation of the KAMRA corneal inlay in the non-dominant eye. On the contrary, it has been reported that both monovision LASIK and monovision contact lenses for the correction of presbyopia result in a significant decline in stereoacuity ().Citation4,Citation5 Levinger et al measured stereoacuity before and after monovision LASIK with the Optec 6500 vision testing system using far stereo depth perception slides for 20–400 arcsec. The author reported a statistically significant difference between the preoperative and postoperative stereoacuity of 52 and 142 arcsec, respectively. For the study group, the mean postoperative uncorrected binocular visual acuity at distance was 20/25 Durrie evaluated the effect of different monovision contact lens powers on stereoacuity using the Optec 3500 (Stereo Optical, Co. Inc.) device in 50 emmetropic presbyopic patients.Citation5
Conclusions
Overall, the author showed worsening stereoacuity with increasing lens power. Initially, the mean distance stereoacuity was 32±23 arcsec. Following treatment, the mean stereoacuity worsened to 44±38 arcsec for the +0.75 D lens power, 77±76 arcsec for the +1.50 D lens power, and 182±142 arcsec for the +2.50 D lens power. The KAMRA corneal inlay results in improved UNVA while maintaining preoperative UDVA in the treated eye.Citation1,Citation3 While all three methods significantly improved visual acuity, preoperative stereoacuity was only preserved with the KAMRA corneal inlay.
Disclosure
The publication fee for this article was paid by AcuFocus Inc. The authors report no other conflicts of interest in this work.
References
- SeyeddainORihaWHohensinnMNixGDexlAKGrabnerGRefractive surgical correction of presbyopia with the AcuFocus small aperture corneal inlay: two-year follow-upJ Refract Surg2010261070771520438021
- DexlAKSeyeddainORihaWOne-year visual outcomes and patient satisfaction after surgical correction of presbyopia with an intracorneal inlay of a new designJ Cataract Refract Surg201238226226922138501
- DexlAKJellGStrohmaierCLong-term outcomes after monocular corneal inlay implantation for the surgical compensation of presbyopiaJ Cataract Refract Surg201541356657525726504
- LevingerETrivizkiOPokroyRLevartoskySSholovGLevingerSMonovision surgery in myopic presbyopes: visual function and satisfactionOptom Vis Sci201390101092109724064524
- DurrieDSThe effect of different monovision contact lens powers on the visual function of emmetropic presbyopic patients (an American Ophthalmological Society thesis)Trans Am Ophthalmol Soc200610436640117471352