Abstract
With the dissemination of optical coherence tomography over the past two decades, the role of persistent vitreomacular adhesion (VMA) in the development of numerous macular pathologies – including idiopathic macular hole, vitreomacular traction syndrome, cystoid and diabetic macular edema, neovascularization in diabetic retinopathy and retinal vein occlusion, exudative age-related macular degeneration, and myopic traction maculopathy – has been established. While invasive vitreoretinal procedures have long been utilized to address complications related to these disorders, such an approach is hampered by incomplete vitreoretinal separation and vitreous removal, surgical complications, and high costs. In light of such limitations, investigators have increasingly looked to nonsurgical means for the treatment of persistent pathologic VMA. Chief among these alternative measures is the intravitreal application of pharmacologic agents for the induction of vitreous liquefaction and/or vitreoretinal separation, an approach termed pharmacologic vitreolysis. This article aims to review the available evidence regarding the use of pharmacologic agents in the treatment of VMA-related pathology. In addition, a discussion of vitreous molecular organization and principles of physiologic posterior vitreous detachment is provided to allow for a consideration of vitreolytic agent mode of action and molecular targets.
Introduction
Perhaps owing to its fundamentally “invisible” nature, the vitreous has long been an under recognized cause of macular pathology. More recently, the improved characterization of vitreomacular relationships facilitated by the evolution of optical coherence tomography (OCT) has led to an increasing recognition of the role played by the posterior vitreous in such disorders. Numerous investigators have found an increased prevalence of incomplete posterior vitreous detachment – a surrogate marker for persistent vitreomacular adhesion (VMA) – in association with a number of retinal disorders including idiopathic macular hole,Citation1 vitreomacular traction syndrome (VMT),Citation2 cystoid (CME)Citation3 and diabetic macular edema (DME),Citation4 neovascularization in diabetic retinopathyCitation5 and retinal vein occlusion (RVO),Citation6 exudative age-related macular degeneration (ARMD),Citation7 and myopic traction maculopathy.Citation8 The pathologic role of VMA in many of these disorders relates to the transmission of static and dynamic anteroposterior tractional forces to the macular surface. The specific pathologic phenotype produced depends on the size and strength of the adhesion, with more extensive vitreous separations and smaller areas of vitreous adhesion imparting greater tractional force.Citation8,Citation9 The role of vitreoretinal and/or vitreomacular adhesion (hereafter referred to collectively as VMA) in the development of neovascularization and nontractional macular edema is less well defined. It may be due in part to residual posterior cortical vitreous acting as a barrier to the flux of important intravitreal moleculesCitation10 (specifically oxygen, growth factors, and cytokines) or as a scaffold for the growth of fibrovascular proliferation arising from the retinal surface.Citation11
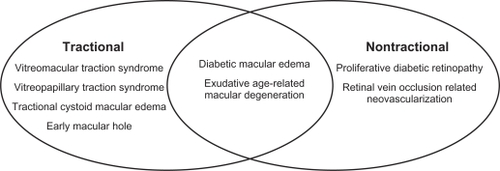
Of note, careful distinction should be made between pathologic (or “symptomatic”) VMA, a categorization that encompasses the pathologic entities described above, and nonpathologic (or “asymptomatic”) VMA in which persistent attachment of the posterior vitreous to the macula does not result in anatomic or functional impairment. This latter form of VMA is frequently noted incidentally on OCT imaging and represents a physiologic stage I posterior vitreous detachment (PVD).Citation8,Citation9 Taken in sum, these descriptions can be utilized to generate a mechanistic classification of disorders associated with pathologic VMA, detailed in .
Figure 1 Schematic representation of mechanistic classification of vitreomacular adhesion-related disease
With the introduction of pars plana vitrectomy by Machemer et al in 1971,Citation12 a definitive solution for VMA-related disease became available to vitreoretinal surgeons. While implementation lagged in line with the delay in recognizing the etiologic role played by the posterior vitreous, the past two decades have seen a dramatic upswing in the application of vitrectomy. In many cases, elimination of vitreoretinal traction and complete separation of the posterior hyaloid from the retinal surface with removal of all vitreous gel lead to both anatomic and functional improvement. Though outcomes have improved with advancements in instrumentation and technique, the utility of vitrectomy remains limited by incomplete vitreoretinal separation and vitreous removal, associated complications, and high costs. Clinical and histologic studies have shown that residual cortical vitreous commonly adheres to the inner retinal surface following vitrectomy despite concentrated aspiration and peeling of the posterior hyaloid.Citation13–Citation15 Cortical vitreous remnants may organize into a fibrocellular epiretinal membrane with subsequent contraction causing macular pucker.Citation16 Indeed, patients with pathologic VMA inherently have exaggerated adherence at the vitreoretinal interface, which in turn leads to a more difficult mechanical separation. Attempts to achieve a cleaner cleavage plane, through mechanical peeling of the internal limiting membrane (ILM), may increase the risk of surgical complications, including retinal hemorrhages, retinal breaks, nerve fiber layer (NFL) damage, and paracentral scotomas.Citation17–Citation19
In light of the inherent limitations associated with vitrectomy for the treatment of pathologic VMA, it is unsurprising that, over the past 15 years, investigators have increasingly examined alternative methods for induction of PVD. Though a few investigators have explored mechanical PVD induction with isolated intraocular gas injectionCitation20–Citation22 and even LASIK (laser-assisted in-situ keratomileusis) suction rings,Citation23,Citation24 the bulk of efforts have focused on the use of pharmacologic agents to modify the molecular structure of the vitreous in order to eliminate its role in disease, a technique termed pharmacologic vitreolysis.Citation25 In general, this involves the induction of vitreoretinal separation and/or liquefaction of vitreous gel either as monotherapy or in conjunction with vitrectomy. This article aims to review the available evidence to date regarding the application of pharmacologic agents in the endeavor of vitreolysis. A summary of vitreous molecular organization and principles of physiologic PVD will provide context for the consideration of vitreolytic agent mode of action and molecular targets. Following a careful analysis of specific indications for pharmacologic vitreolysis, the individual agents will be reviewed with summaries to include postulated mechanism of action, results of past pre-clinical and clinical trials (if available) as well as a discussion of any pending investigations. A final section on emerging trends and future directions will conclude the review.
Vitreous molecular organization and structure
Pharmacologic vitreolysis is largely an outgrowth of an evolving understanding of the molecular organization, structure, and physiology of the vitreous. This knowledge has allowed for the selection of appropriate agents to target key molecules and structures within the vitreous gel as well as at the vitreoretinal interface.
Consistent with its dual purpose of maintaining media clarity and mitigating possible concussive effects associated with ocular movement or trauma,Citation26 the vitreous is a transparent viscoelastic extracellular gel matrix (ECM) composed of approximately 99% water.Citation27 In the gel state, vitreous further maintains media clarity by acting as a barrier to limit cellular invasionCitation27 and may also act to protect sensitive tissues such as the crystalline lens and trabecular meshwork from oxidative damage via its role in oxygen metabolism.Citation28,Citation29 These unique properties are a direct result of the molecular structure of vitreous gel, which consists of two complementary macromolecular structures: a fibrillar component, represented by collagen; and glycosaminoglycans (GAGs), chiefly hyaluronan with a lesser concentration of chondroitin sulfate. Vitreous collagen consists of heterotypic fibrils composed of a combination of collagen type II, type IX, and a hybrid type V/XI. The core of each fibril is composed of type V/XI collagen, which is surrounded by a sheath of fibrillar type II collagen as well as a regular arrangement of type IX collagen along the outermost surface of the fibril.Citation27 The rope-like structures formed are largely resistant to proteolysis except by a few select proteases – bacterial collagenase, cathespin K, and certain matrix metalloproteinases.Citation30 The heterotypic fibrils are arranged into interconnecting bundles that form an extended network, which provides shape, strength, and flexibility to the vitreous and allows it to resist tractional forces. As mentioned above, the GAG component is predominantly hyaluronan (>90%) along with chondroitin sulfate, which is found only in proteoglycan form (attached to a protein core) as either versican or collagen type IX.Citation27 The negatively charged disaccharide moieties of hyaluronan attract a shell of water molecules that act to inflate the collagen matrix and provide swelling pressure to resist compressive forces. Chondroitin sulfate appears to be involved in the maintenance of interfibrillar spacing via interconnections between collagen fibrils mediated through links to opticin, a small leucine-rich repeat protein.Citation31
As the site of adhesion between the posterior cortical vitreous and the ILM, the vitreoretinal interface plays a decisive role in the relationship between physiologic and pathologic VMA. The interface juxtaposes the ILM, a basement membrane secreted by underlying Müller cells, and the posterior hyaloid. Similar to basal membranes elsewhere in the body, the ILM is compromised chiefly of collagen type IV,Citation32 which imparts a sheet-like conformation, in addition to several ECM proteins, notably laminin, fibronectin,Citation33 and collagen type XVIII.Citation34 Despite this expanding knowledge of vitreoretinal interface components, the mechanisms underlying VMA remain poorly understood. Histologic studies have demonstrated that vitreous collagen fibrils are oriented in an anteroposterior manner and, posterior to the vitreous base, run parallel to the ILM.Citation35 However, at the vitreous base, vitreous collagen fibrils run perpendicular to and pass through the ILM where they insert to form an adhesion, considered unbreakable without proteolysis.Citation36,Citation37 This contrasts with the posterior vitreoretinal interface at which collagen fibrils do not insert into the ILM. Instead, VMA posterior to the vitreous base is thought to be fascial in nature and mediated by some form of “extracellular matrix glue” that connects cortical vitreous collagen fibrils with the ILM surface.Citation38 ILM-associated molecules suggested as potential “glue” components include laminin and fibronectin, which have been demonstrated to have high affinity for collagen,Citation39,Citation40 as well as collagen type XVIII, which has been shown to be bound by the opticin molecules coating vitreous collagen fibrils.Citation31
Principles of physiologic PVD
The process of physiologic, or age-related, PVD is well characterized from a mechanistic standpoint, but remains poorly understood on a molecular level. While the lack of an accurate molecular description has hampered the development of pharmacologic vitreolytics, improved understanding of the physical sequence of uncomplicated PVD has shed significant light on ways in which it may go awry and induce pathologic sequelae. Within the vitreous gel, two related processes, liquefaction (synchysis) and fibrillar collapse (syneresis), act as the primary motive force driving vitreoretinal separation.Citation41,Citation42 Liquefaction originates in the premacular cortical vitreous where it has been detected as early as 2 years of age in fixed autopsy specimens.Citation43 Focal collections of liquefaction, or liquefied lacunae, subsequently form throughout the vitreous, increasing in number and size during adolescence and adulthood.Citation41–Citation44 This process culminates in the coalescence of extensive areas of synchysis, with approximately 70% of autopsy eyes obtained from donors aged 70 years and greater demonstrating at least 50% liquefaction of the vitreous body.Citation41 As liquefaction progresses, the collagen fibrillar meshwork undergoes collapse. This leads to the aggregation of collagen into parallel bundles that form thick fibers, seen clinically as syneretic debris, which become progressively dense and tortuous with age.Citation35,Citation44 In line with the demonstrated positive correlation between the extent of synchysis/syneresis and PVD incidence,Citation41,Citation45,Citation46 liquefaction with subsequent collapse appears to drive vitreoretinal separation following attenuation of the adhesion between the cortical vitreous and ILM of the posterior pole. Though previous investigators believed it to be an acute process,Citation41,Citation47 more recent studies indicate that PVD occurs over months to years, beginning as a shallow perifoveal vitreoretinal separation that expands gradually until complete PVD is achieved with acute separation of the vitreous from the optic disc margin.Citation8,Citation9
The weakening of the adhesion between the vitreous and the retina stands as a critical factor in the timing and progression of PVD. Multiple studies have demonstrated that the majority of patients less than age 60 have an intact vitreoretinal interface despite the presence of extensive liquefaction.Citation41,Citation45 After age 60, however, there is a much stronger correlation between PVD incidence and extent of liquefaction, indicating the presence of some factor that enhances the effect of liquefaction and collapse on PVD induction; this factor is likely a weakened adhesive force between the retina and vitreous.Citation41,Citation45 Variations in strength of this force likely determine whether a given PVD is accompanied by pathologic sequelae. In a subset of eyes, age-related PVD progresses normally except where especially firm vitreorentinal adhesions are encountered in the macula, at the optic disc margin, or at focal sites in the retinal periphery. In such eyes, dynamic (saccadic) vitreous traction is exerted upon the retina at the residual adhesion site(s), leading to various complications including macular hole, VMT, tractional DME, vitreopapillary traction syndrome (VPT), vitreous hemorrhage, and retinal tears.Citation8,Citation9 Sebag coined the term “anomalous PVD,” to describe the condition in which the extent of gel liquefaction and collapse exceed the attenuation of vitreorentinal adhesion.Citation48 This condition results from disorders that cause premature vitreous liquefaction, including hereditary vitreoretinal syndromes, uveitis, vitreous hemorrhage, and high myopia, and increases the risk of PVD-associated morbidity.
To improve upon existing mechanical methods for the treatment of pathologic PVD, controlled induction of vitreous liquefaction and weakening of vitreorentinal adhesion will be necessary. Targeted pharmacologic agents, capable of altering the molecular organization of the vitreous gel and vitreoretinal interface, have the potential to provide such control.Citation25 Unfortunately, the development of these agents has been slowed by the lack of accurate molecular descriptions of the processes in question. As mentioned above, the basis of vitreorentinal adhesion remains poorly described. The same is true of the physiologic weakening of vitreorentinal adhesion that accompanies aging. Investigators have proposed several possible age-related changes – including alterations in Müller cell function,Citation49 thickening of the ILM,Citation50 or the cumulative effects of incident light-generated free radicalsCitation51 – as a basis for this weakening. Similarly, models of age-related vitreous liquefaction, implicating incident light-generated free radicalsCitation52–Citation54 or enzymatic degradation of collagen,Citation55–Citation57 have been suggested but remain largely unproven.
Indications for pharmacologic vitreolysis
From a pathophysiologic perspective, any manifestation of pathologic VMA should benefit from pharmacologic vitreoretinal separation, based on either release of anteroposterior traction (tractional VMA) or removal of premacular vitreous cortex (nontractional VMA). While this may be true in principle, the selection of appropriate indications for pharmacologic vitreolysis requires careful consideration of utilization models and therapeutic goals.
While early interest in pharmacologic vitreolysis focused on its application as an adjunct to vitrectomy and removal of fibrovascular proliferative membranes,Citation58–Citation60 investigators quickly realized its potential as a stand-alone therapy.Citation61–Citation63 Indeed, clinical applications of pharmacologic vitreolysis can be broadly grouped into two categories based on utilization model: pharmacology-assisted vitrectomy and pharmacologic PVD induction. In the former model, a pharmacologic agent administered preoperatively acts to either induce vitreous liquefaction, allowing for more rapid vitreous removal, or weaken the vitreorentinal adhesion, allowing for greater ease of mechanical PVD induction with a cleaner vitreoretinal separation.Citation15,Citation64–Citation67 More rapid vitreous removal translates into shorter surgical timesCitation15,Citation25,Citation68 and possibly an increased ability to employ smaller gauge instrumentation,Citation69,Citation70 which are associated with reduced postoperative recovery times.Citation71,Citation72 Weakening of the vitreorentinal adhesion allows mechanical PVD creation without the use of high suction, which reduces the risk of iatrogenic tearsCitation73,Citation74 and permits the use of smaller gauge instrumentation not capable of achieving such high levels of aspiration.Citation69,Citation75,Citation76 Theoretically, it also facilitates cleaner vitreoretinal separation, avoiding cortical vitreous remnants and thereby reducing postoperative complications such as macular pucker,Citation77 proliferative vitreoretinopathy (PVR),Citation78,Citation79 and persistence of diabetic retinopathy-related complications.Citation80
When pharmacologic vitreolysis is used as stand-alone therapy, vitreolytic agents can be employed either as a definitive treatment in active VMA-related disease or as a prophylactic measure in conditions in which PVD is associated with an improved prognosis. Examples of the former include early macular holes, VMT, VPT, and tractional DME/CME,Citation8,Citation9,Citation48 while the latter includes conditions such as DME,Citation4 proliferative diabetic retinopathy (PDR),Citation5,Citation81,Citation82 RVO,Citation6,Citation83–Citation85 and ARMD.Citation7,Citation86,Citation87 In all cases, the therapeutic effect results from induction of complete pharmacologic PVD. The basis of the prophylactic benefit of PVD in macular edema and neovascularization remains unclear, but likely relates to the barrier and scaffold functions played by posterior cortical vitreous discussed earlier. Of note, stand-alone vitreolytic therapy has also been utilized strictly for its liquefactive properties in conditions such as non-clearing vitreous hemorrhage;Citation88,Citation89 however, this indication is outside the scope of this review as it does not pertain to VMA-related disease.
As is the case with most ophthalmologic therapeutic interventions, pharmacologic vitreolysis is indicated in the conditions discussed above based on its potential to improve anatomical and functional outcomes. In addition to this primary therapeutic objective, ancillary goals should also be considered, including: decreased costs, based on shorter surgical times or decreased incidence of progressive disease requiring surgery; and greater access to therapy, based on the simple instrumentation involved and a possible transition to office-based procedures.Citation25,Citation68,Citation90 A reduction in surgical cases, due to either a decreased incidence of advanced disease following prophylactic therapy or due to a transition to office-based treatment of VMA-related disease, would have the additional benefit of reducing patient exposure to vitrectomy-related complications – such as endophthalmitis, cataract, and iatrogenic breaks – as well as complications related to anesthesia.
Vitreolytic agents
Overview
The biochemical properties requisite in any potential vitreolytic agent include the ability to induce vitreous liquefaction (liquefactants), weakening of the vitreorentinal adhesion (interfactants), or both.Citation25,Citation90 These molecular alterations may be accomplished through either nonenzymatic, or more commonly, enzymatic means. Based on these characteristics, the available vitreolytic agents – including those previously tested as well as those that remain under development – can be classified as detailed in .Citation25,Citation90 The following section aims to review the mechanism of action of each agent and summarize the results of relevant pre-clinical and clinical trials.
Table 1 Classification of pharmacologic vitreolytic agents
Collagenase
Bacterial collagenase, purified from Clostridium histolyticum, is one of the few proteases known to cleave the type II collagen comprising the fibrillar network of the vitreous gel.Citation30 In contrast to fibrillar collagen, the resulting proteolyzed fragments are soluble, allowing for spontaneous denaturation and further degradation by nonspecific proteases.Citation91 Prolonged intravitreal incubation of escalating doses of bacterial collagenase in rabbits resulted in dose-dependent liquefaction, but was accompanied by ILM damage and disruption of retinal architecture at doses achieving clinically significant degrees of liquefaction.Citation92 Using lower doses and shorter incubation periods, subsequent studies in a rabbit model of PVR demonstrated some focal fibrovascular membrane digestion prior to vitrectomy, although histologic and electrophysiologic toxicity was noted at incubation periods greater than 30 minutes.Citation58,Citation60 Later human pilot studies of collagenase-assisted vitrectomy resulted in hemorrhages on the surface of the retina as well as evidence of digestion of retinal vasculature on proliferative membranes,Citation59,Citation81 which confirmed earlier reports of severe retinal hemorrhages in rabbits.Citation93
Chondroitinase
Although substrate specificity varies depending on the bacterial species of origin, chondroitinase catalyzes the depolymerization of various GAGs including chondroitin sulfate, hyaluronan, and dermatan sulfate.Citation94 The role of chondroitin sulfate within the vitreous remains unclear. It is generally found in proteoglycan form as either versican, which is linked to hyaluronan, or as collagen IX, which coats the heterotypic vitreous collagen fibrils.Citation27 Some investigators believe it may contribute to vitreous structure or spacing by linking the hyaluronan network to other integral ECM components,Citation27 while others have reported it may play a role in vitreorentinal adhesion based on immunolocalization of chondroitin sulfate to the vitreous base and papillary margin.Citation95 Early pre-clinical results examining the vitreolytic potential of chondroitinase were mixed. One group found intravitreal chondroitinase to have no effect on vitreous liquefaction or vitreorentinal adhesion in a rabbit model,Citation93 while a second group found complete vitreous body disinsertion, including at the vitreous base, prior to vitrectomy in cynomologus monkeys as well as in a limited number of human cadaver eyes.Citation95 This latter group also found no microscopic, immunohistochemical, or electroretinography (ERG) evidence of retinal toxicity up to 16 months following the procedure.Citation95 Two studies comparing the liquefactive capacity of chondroitinase to hyaluronidase and plasmin in animal models demonstrated modest reduction in wet weight following 48-hour incubation of isolated vitreous gel as well as a mild enhancement of gel removal during standardized vitrectomy following 1 and 3 hours incubation.Citation96,Citation97 The significantly lower doses used in these studies did not appear to induce an accompanying gel collapse,Citation96 but were associated with mild ILM or NFL damage in the vitrectomy-based study.Citation97 In a later study evaluating PVD induction in an enzyme-assisted vitrectomy model in pigs, chondroitinase, at similarly low doses, failed to achieve a significant improvement in the rate of spontaneous PVD, the extent of PVD, or the degree of residual collagen detected on electron microscopy (EM) when compared with controls.Citation98 Thus, initial encouraging results were unable to be duplicated in later trials using much lower doses, which did still demonstrate some limited toxicity.
Hyaluronidase
Hyaluronidase is an endoglycosidase capable of cleaving bulky hyaluronan molecules, in addition to other GAGs such as chondroitin sulfate, into much smaller fragments.Citation99 The resulting decreased viscosity within the ECM allows for easier passage of material through the ECM. This property has already been exploited clinically to increase the absorption and dispersion of injected drugs such as anesthetics.Citation100 As hyaluronan plays a critical role in maintaining the gel-like character of the vitreous, hyaluronidase possesses considerable potential as a liquefactive agent. Hyaluronidase-mediated vitreous liquefaction has been demonstrated both in vitroCitation96 and in vivo,Citation101,Citation102 and more recently, in Phase III trials studying its potential in speeding the clearance of vitreous hemorrhage.Citation88,Citation89 Additionally, hyaluronidase was shown to significantly improve the extent of vitreous removal during standardized vitrectomy compared with untreated eyes after incubations of 1 or 3 hours.Citation97 In view of the clear association between age-related PVD and vitreous liquefaction, hyaluronidase would seem a logical agent for pharmacologic induction of PVD. Initial studies examining low dose (1 U) intravitreal hyaluronidase in conjunction with perfluoropropane gas in a rabbit model exhibited only partial PVD following 3-day incubations; this contrasted with eyes receiving either hyaluronidase or gas alone, in which no PVD was detected.Citation103 Using higher doses (5–20 U) of hyaluronidase alone in a similar rabbit model, two follow-up studies produced very different outcomes: one reported gradual development of PVD at 5–8 weeks in nearly all experimental eyes at the highest doses (10 and 20 U),Citation62 while a later study reported no PVD in any experimental eye at 3 and 6 months using a similarly high dose (20 U).Citation104 Although the source of the discrepancy is unclear, the authors of the latter study implicated inadequacy of the light microscopy and clinical examination for PVD determination employed in the former study compared with the EM techniques utilized in their own study.Citation104 The poor performance of hyaluronidase (20 U) in PVD induction was confirmed by a separate group, again using EM to assess PVD status, though the incubation period in this study was considerably shorter at 1 week.Citation105 In terms of safety, hyaluronidase was generally well tolerated up to doses of 20 U at incubation periods ranging from 3 to 28 days.Citation62,Citation102,Citation103,Citation105 Aside from transient vitreous haze noted at nearly all doses and incubation periods,Citation62,Citation102–Citation105 there was no evidence of retinal structural toxicity, as assessed by EM,Citation102,Citation103,Citation105 nor functional toxicity, as assessed by ERG.Citation62,Citation103,Citation105 Reported toxicities at higher doses were mixed, with one group demonstrating disruption of retinal cellular anatomy at doses as low as 30 U (bovine hyaluronidase) for 1 week, while the large Phase III trial using doses of 55 and 75 IU (ovine hyaluronidase) reported only an increased rate of transient moderate-severe iritis.Citation89 Despite impressive liquefactive capacity, hyaluronidase appears limited in terms of PVD induction as it has no demonstrated impact on the vitreoretinal interface. Investigators hypothesized that the induction of PVD by hyaluronidase follows liquefaction of central vitreous, with collapse and subsequent loss of support for cortical vitreous fibers, rendering it susceptible to separation by mechanical forces such as eye movements.Citation62,Citation104 In effect, hyaluronidase produces PVD through an increase in vitreoretinal traction and may worsen existing VMA-related pathologies.
Dispase
A neutral protease obtained from Bacillus polymyxa, dispase is known to cleave type IV collagen and fibronectin while laminin and other collagen subtypes are left largely unaltered.Citation106 Given its activity against type IV collagen, a major component of the ILM, and fibronectin, postulated to be a factor in vitreorentinal adhesion, dispase was tabbed as a vitreolytic agent based on its potential to mediate vitreoretinal disinsertion. Interestingly, dispase was initially utilized intravitreally to generate an animal model of PVR without the addition of exogenous cells.Citation107,Citation108 This model was based on the ability of dispase to release endogenous cells – such as fibroblasts, macrophages, and glial cells – from their cellular attachments and recruit them into the vitreous. As PVR generation was achieved with prolonged incubations at very low doses (0.01–0.50 U),Citation107,Citation108 later studies investigating the utility of dispase in PVD induction used shorter incubation periods (15–120 minutes) at the same or higher doses.Citation63,Citation109–Citation111 In effect, dispase was only evaluated as an agent for enzyme-assisted vitrectomy due to the fact that removal of the enzyme following a specified incubation would be required to avoid PVR development. In the two earliest such studies, dispase achieved significantly higher rates of spontaneous complete PVD in enucleated pig and human eyes as well as pig eyes in vivo at the majority of doses tested following 15 or 120 minutes of incubation.Citation63,Citation109 Neither study revealed significant toxicity, excepting transient vitreous haze.Citation63,Citation109 In contrast, a similar study of dispase-assisted vitrectomy in rabbits in vivo using greater doses and incubation times failed to show any effect on PVD induction, and enzyme use was associated with retinal and vitreous hemorrhages.Citation110 Further evidence of dispase-associated toxicity was found in two follow-up studies in an in-vivo rabbit model: in addition to vitreous hemorrhage and cataract formation, histologic exam revealed disruption of ganglion cell and photoreceptor layers, while ERG testing revealed significant depression of a- and b-wave amplitudes.Citation111,Citation112 These studies did employ longer incubations (1 week), but clinical evidence of toxicity was noted as early as 30 minutes following injection.Citation111,Citation112 The reason for the conflicting results regarding the safety and efficacy of dispase in vitreolysis is unclear but may be related to the model used. Regardless, given its ability to generate PVR as well as its action on collagen IV, a major component of the ILM and lenticular capsule, the safety of dispase remains questionable at best.
Nattokinase
Originally discovered in the Japanese soybean cheese nattō, nattokinase is a serine protease produced by Bacillus subtilius.Citation113 Although incompletely characterized, it is known to possess potent fibrinolytic effects likely due to its enhancement of plasmin activation via increased synthesis of tissue plasminogen activator (tPA)Citation114 as well as inactivation of plasmin activator inhibitors.Citation115 Additionally, nattokinase has direct proteolytic effects on collagen.Citation116 Thus, the postulated PVD induction mechanism of nattokinase involves some combination of direct liquefaction and plasmin-mediated vitreoretinal dehiscence. In the rabbit model, intravitreal injection resulted in histologically confirmed PVD (eg, bare ILM) in all eyes at the two highest doses following 30-minute incubations; however, eyes exposed to the highest dose displayed subtle alterations in inner retinal architecture, parapapillary retinal hemorrhages, and ERG depression.Citation116 To date, no follow-up investigations have been conducted.
Plasmin
Undoubtedly the most widely studied vitreolytic agent, plasmin is a serine protease with a critical role in fibrinolysis. In addition to fibrin, plasmin has been shown to directly degrade other ECM components including laminin and fibronectin,Citation117–Citation119 which have a postulated role in vitreorentinal adhesion.Citation33 Plasmin may also indirectly generate increased levels of other nonspecific proteases such as matrix metalloproteinasesCitation120,Citation121 and elastase,Citation122 capable of cleaving further ECM structures. These downstream activities may enhance the primary action of plasmin – weakening of vitreoretinal insertion – or may allow for a limited degree of liquefaction. Initial studies of plasmin (1 U) with and without adjunctive vitrectomyCitation61 or intraocular gas injectionCitation123 in a rabbit model indicated that such adjunctive procedures were necessary to achieve clean vitreoretinal separation. Similar results were obtained in human cadaver eyes using a plasmin-assisted vitrectomy model in which the addition of 1 U of plasmin was found to eliminate the cortical vitreous remnants noted on the ILM in untreated, vitrectomized eyes.Citation15 Surprisingly, in follow-up studies by the same group in both enucleated pigCitation124 and human eyes,Citation119,Citation125 short incubations (30–60 minutes) with similar doses of plasmin (1–3 U) also resulted in a bare ILM without the use of adjunctive techniques. Further in-vivo studies in rabbits, however, indicated that the previous results in cadaver eyes may have been related to specific properties of post-mortem eyes, as very low rates of complete PVD were found following prolonged exposure (1 week) to 1 U of plasmin.Citation105,Citation112 Better rates of complete PVD were achieved with higher doses (4 U).Citation112 Several studies were able to demonstrate a correlation between both plasmin concentration and exposure time and the resultant extent of vitreoretinal separation.Citation61,Citation119,Citation124 The safety profile of intravitreal plasmin in these pre-clinical trials was excellent. Excepting a consistent finding of transient vitreous haze,Citation61,Citation105,Citation112,Citation123 there were no reported toxicities despite thorough histologic examination with light and EM at doses up to 4 U and with exposure times ranging from 30 minutes to 1 week.Citation61,Citation105,Citation112,Citation119,Citation124,Citation125 No functional toxicity was detected by ERG in three studies,Citation105,Citation112,Citation123 while a fourth found only transient depression of b-wave amplitudes.Citation61 One group, using a plasmin-assisted vitrectomy model in enucleated pig eyes, reported rare ILM (0%–20%) and NFL (0%–10%) damage at doses of 3 and 30 U, with incubations of 1 and 3 hours.Citation97
As plasmin is exceedingly unstable owing to rapid inactivation via autolysis and binding to α2-antiplasmin, clinical application typically requires activation of its proenzyme, plasminogen, with plasminogen activators immediately prior to use. Application in human trials is further complicated by the lack of an approved, commercially available plasminogen. In place of a commercial alternative, investigators have relied on the time-consuming and expensive process of autologous plasmin enzyme (APE) generation via harvesting a patient’s own plasma-derived plasminogen and purifying it via affinity chromatography.Citation126 Numerous human pilot studies used this technique to examine outcomes of plasmin-assisted vitrectomy, with doses ranging from 0.03 U up to 2 U, in a variety of VMA-related disorders. Because of the exceptionally strong vitreorentinal adhesion found in pediatric patients,Citation50 several groups examined the use of APE in the surgical treatment of pediatric traumatic macular holes,Citation126,Citation127 stage 5 retinopathy of prematurity,Citation128,Citation129 and complicated X-linked retinoschisis;Citation130 all reported improved anatomic outcomes compared with previously published studies. Other investigators employed plasmin-assisted vitrectomy to treat full-thickness macular holes in patients without pre-existing PVD and found high rates of spontaneous PVD intraoperatively, which reduced overall surgical time.Citation131–Citation133 The application of APE prior to vitrectomy resulted in nonsignificant increases in spontaneous PVD and ease of PVD induction in eyes with tractional DMECitation77,Citation134,Citation135 and complicated PDR.Citation136 One comparative study reported significantly higher visual acuities at 1 year follow-up in patients with DME treated with APE compared with those not receiving such treatment.Citation134 More recently, a small prospective study found that intravitreal APE without vitrectomy improved central macular thickness and visual acuity in eyes with macular edema complicating branch RVO.Citation137 Of note, many groups reported varying degrees of vitreous liquefaction following APE administration,Citation77,Citation127,Citation131,Citation133,Citation135,Citation136 although several others either did not comment or noted the lack of liquefaction.Citation134 In this collection of pilot studies, no investigator reported a clear enzyme-related complication.
Plasminogen activators (tPA and urokinase [UK])
Potent fibrinolytic agents originally approved for a variety of nonophthalmologic vascular disorders including stroke, symptomatic coronary artery, and peripheral vascular occlusive disease, intraocular plasminogen activators have proven to be of modest utility in the treatment of several ophthalmologic conditions including post-surgical fibrin formation, submacular hemorrhage, and acute RVO.Citation138,Citation139 As serine proteases capable of activating plasminogen, both tPA and UK exert their effects indirectly through plasmin. Several groups turned to plasminogen activators as potential vitreolytic agents in lieu of plasmin based on: (1) the ease of access to a US Food and Drug Administration-approved commercially available formulation, (2) the safety of a recombinant molecule compared with blood derivatives in terms of microbial contamination, and (3) the established intraocular safety record based on its use for other indications.Citation140 The challenge in working with plasminogen activators, however, lies in the need for clinically sufficient quantities of intraocular plasminogen, which outside the setting of pathologic blood–retinal barrier breakdown (ie, intraocular inflammation, hemorrhage, PDR),Citation141 can typically only be achieved via iatrogenic blood–retinal barrier breakdown (ie, cryopexy)Citation142 or exogenous administration.Citation143,Citation144 In a rabbit model, cryopexy followed by tPA and limited vitrectomy (static core vitrectomy only) induced PVD in all treated eyes, whereas no PVD was noted in eyes not receiving either cryopexy or tPA injection.Citation142 Two later in-vivo rabbit studies examined the efficacy of UK plus exogenous plasminogen with differing results.Citation143,Citation144 Complete PVD was noted in all eyes at the two highest nontoxic doses of UK plus purified human plasminogen,Citation143 but only occurred with the addition of intraocular sulfur hexafluoride following UK plus recombinant plasminogen in a later study.Citation144 In human pilot studies, tPA-assisted vitrectomy in patients with complicated PDR was not associated with spontaneous PVD induction (assessed intraoperatively) nor with any significant improvement in postoperative functional outcomes.Citation145 However, a subsequent report of tPA injection alone in patients with RVO-associated macular edema revealed post-treatment PVD in a majority of patients that correlated with improved functional and anatomic outcomes.Citation146 Overall, plasminogen activators, much like plasmin, have a promising efficacy and safety record, but their therapeutic potential will continue to be limited by the need for adequate concentrations of intraocular plasminogen substrate. Assuring sufficient quantities of plasminogen, either through exogenous administration or blood–retinal barrier breakdown, inevitably leads to imprecise dosing.
Microplasmin
Another agent initially developed for systemic administration in the treatment of cerebral thromboembolic disease, microplasmin is a recombinant molecule, highly expressed in the Pischia pastoris yeast expression system, consisting solely of the catalytic domain of human plasmin.Citation147 It has several advantages over plasmin: (1) it is commercially available, allowing investigators to avoid the time-intensive and expensive production of APE; (2) it is generated by recombinant techniques, assuring its sterility and avoiding the risk of microbial contamination; (3) it is much smaller than plasmin (22 versus 88 kDa), which theoretically would allow for greater penetration of epiretinal tissues; and (4) it is inherently more stable than plasmin and can be stored in citrate buffer prior to use.Citation147–Citation149 It is thus unsurprising – given the greater safety, ease of administration, and dosing accuracy – that investigators increasingly turned to microplasmin for the treatment of VMA-related pathologies in favor of either plasmin or plasminogen activators. The initial pre-clinical studies revealed achievement of complete PVD (eg, bare ILM) at doses ranging from 62.5–125.0 μg (equivalent to 1–2 U of plasmin) in enucleated human eyes with or without adjunctive intraocular gas.Citation148 In-vivo studies similarly exhibited complete PVD following 7–21 day intravitreal microplasmin exposure with doses differing based on species; cat eyes achieved PVD at doses of 14.5–25.0 μg,Citation148 while two separate studies in rabbits reported consistent PVD at doses of 125–250 μg.Citation149,Citation150 No histologic toxicityCitation148–Citation150 or functional toxicityCitation149 was noted excepting persistent a- and b-wave depression on ERG testing in the 250 μg group only. A later study in enucleated pig eyes utilized a dose- (range 62.5–400 μg incubated for 1 or 2 hours) and exposure time-escalation (range 15–120 minutes after 125 μg administration) design.Citation151 Their results demonstrated both time- and dose-dependent PVD development with a minimal effective dose of 125 μg and a minimal effective incubation period of 60 minutes with 125 μg dose. These values may have been somewhat inflated by the use of room temperature incubations. Although no disruption of cellular anatomy was noted in any experimental eye, serous-like retinal elevations were detected in 25% of eyes exposed to 400 μg for 120 minutes and scattered dendritic-like cells were found on the ILM in eyes receiving doses of 125 μg or higher for 120 minutes, with a greater number of cells in eyes administered higher doses.
Based on the promising anatomic and safety profile reported in these pre-clinical studies, a series of clinical trials was undertaken collectively entitled the Microplasmin Intravitreal Injections (MIVI) trials. MIVI-I was an uncontrolled Phase I/IIa clinical trial designed to assess safety and preliminary efficacy at various doses (25, 50, 75, and 125 μg for 24 hours) and exposures (2 hours, 24 hours, or 7 days following 25 μg administration) of microplasmin in enzyme-assisted vitrectomy for the treatment of VMA-related pathologies including tractional DME, VMT, and full-thickness macular holes.Citation152 The incidence of spontaneous PVD as well as the ease of PVD induction intraoperatively were found to be both time- and dose-dependent, although no more than 50% of eyes in any one cohort developed spontaneous PVD. Of note, the three eyes in the highest dose cohort were noted to have vitreoschisis intraoperatively, and thus were incorrectly classified as spontaneous PVDs by ultrasound. Aside from a single retinal detachment noted shortly following microplasmin administration, there were no safety concerns ascribed to the study drug. MIVI-IIt (traction) was a follow-up Phase II prospective sham-controlled trial examining the efficacy of microplasmin alone for the treatment of VMT and early macular holes.Citation153 In this trial, patients were divided into four cohorts and randomized 4:1 to microplasmin at doses of 75, 125, 175, and repeatable 125 μg doses or sham injection and followed with serial OCT and ultrasound exams. A significantly higher incidence of PVD was noted in the 125 μg cohort as well as the pooled (all doses) microplasmin cohort at 90 days, but not at the remaining time points (14, 28, and 180 days). At 28 days, nonsurgical release of VMA was achieved in 8%, 25%, 44%, and 27% of patients in the sham, 75, 125, and 175 μg cohorts, respectively, with no significant difference observed in the overall analysis or in pairwise comparisons. A larger multicenter Phase IIb prospective placebo-controlled trial, MIVI-III, was subsequently designed to evaluate three doses of microplasmin (25, 75, and 125 μg) compared with placebo administered 7 days prior to vitrectomy for the treatment of a variety of VMA-related disorders.Citation69 No significant pairwise differences were found in terms of spontaneous PVD induction, but there was significantly greater progression of PVD from the date of microplasmin administration until surgery in the 125 μg cohort compared with placebo. Within the 125 μg cohort, there were also a significantly greater proportion of patients in the total cohort as well as within the subset of patients with macular holes who achieved resolution of their condition without the need for vitrectomy versus placebo. Two additional MIVI trials were conducted, but results have yet to be formally published. MIVI-II (TG-MV-002) is a Phase II sham-controlled non-vitrectomy study in patients with tractional DME that completed data collection in March 2010. MIVI-Trust (Traction Release without Surgical Treatment) (TM-MV-006, TM-MV-007) is a Phase III multicenter, randomized, placebo-controlled trial evaluating 125 μg of microplasmin alone for the treatment of focal VMA associated with subjective visual dysfunction, a concept the study designers have labeled “symptomatic VMA,” that completed data collection in July 2010. The preliminary results of this latter trial were reported at the 2011 ARVO (Association for Research in Vision and Ophthalmology) meeting and indicated a statistically significant improvement in the rate of pharmacological resolution of symptomatic VMA in the microplasmin group compared with placebo.Citation154 Formal publication of results from both of these studies should be forthcoming in the near future.
RGD peptides
Widely expressed cell surface receptors, integrins, play a critical role in cellular-ECM adhesion and signaling.Citation155 Binding to integrins is mediated through a specific binding motif – defined by the amino acid sequence arginine-glycine-aspartate (RGD) – present in a vast array of ECM components including laminin, fibronectin, and certain collagens.Citation155 Synthetic RGD peptides are known to compete for integrin binding sites, which results in disruption of integrin-ECM interaction and subsequent loosening of attachments.Citation156 As immunolocalization studies have identified integrins on the surface of the ILM,Citation157 there has been considerable speculation regarding a possible role of synthetic RGD peptides in disrupting vitreorentinal adhesion, and by extension, a potential utility in vitreolysis. In a rabbit model, 24-hour incubation of intravitreal RGD peptides followed by limited vitrectomy – consisting of 30-second core vitrectomy with attempted PVD induction at low aspiration (≤30 mmHg) – resulted in a significantly greater extent of PVD in treated eyes compared with controls; however, only a single treated eye achieved complete PVD. Aside from focal retinal edema noted in half of the treated eyes, no toxicity was detected on clinical examination, EM analysis, or TUNEL (terminal deoxynucleotidyl transferase dUTP nick end labeling) apoptosis assay.Citation158 Despite the modest success of this initial study, no further studies have been published.
Vitreosolve®
Vitreosolve® (Vitreoretinal Technologies Inc, Irvine, CA) is a proprietary nonenzymatic, urea-based molecule currently undergoing Phase II/III testing (PVD-301, PVD-302) in patients with non-proliferative diabetic retinopathy without pre-existing PVD. Given the proprietary nature of the agent, there is little information regarding its structure or mechanism. Preliminary results from an earlier, unpublished study demonstrated PVD induction in 45% of patients following a single 12 mg injection with the proportion rising to 75% following a second injection 30 days later.Citation159 As Phase II/III trials are currently enrolling patients, final results may be pending for some time.
Conclusion
Medical therapy of VMA-related disorders is an exciting and promising area of investigation but currently remains an incompletely realized technology. To facilitate the identification of new agents and maximize the therapeutic potential of current vitreolytics, additional efforts are needed to expand present knowledge of vitreous molecular structure and physiology. Future work on existing agents will undoubtedly draw on the studies reviewed above, though care must be taken in evaluating this body of literature. Two characteristics of previous study design warrant further discussion: PVD definition and clinical model. The modality used to assess for the presence of PVD varies significantly between studies – ranging from clinical examination to ultrasonography to EM – thus complicating inter-study comparison. Moreover, the definition of complete PVD differed significantly and was often related to the assessment modality employed; complete PVD by microscopy typically signified the absence of collagen fibrils on the small specimen of ILM examined, while OCT and ultrasound looked more macroscopically – though perhaps less sensitively – at the vitreoretinal interface. The considerable variability in choice of clinical models also impacts study outcomes. Physiologic PVD is not known to occur in either rabbitCitation61 or pig eyesCitation124 – indicating a distinctly different vitreous physiology – and differences in ILM thickness might exaggerate perceived toxicities in certain models.Citation36 Additionally, use of cadaver models may be confounded by differences in temperature, pH, solubility parameters, and electrolyte concentrations, which vary depending on the duration of the post-mortem period.Citation160
Study design issues notwithstanding, many of the agents examined to date have shown the capacity to produce significant degrees of vitreous liquefaction or weakening of vitreorentinal adhesion. Unfortunately, these changes are rarely induced concurrently or in the appropriate proportions to induce a safe and reliable PVD. Agents acting either solely through liquefaction (liquefactants such as hyaluronidase and collagenase) or vitreoretinal interface disruption (interfactants such as dispase or RGD peptides) are non-physiologic and have the potential to worsen existing tractional pathology. Plasmin-based agents have shown some ability to concurrently liquefy vitreous and weaken vitreorentinal adhesion; however, the presence of liquefaction is inconsistent and its extent is quite variable.Citation127,Citation131,Citation161 Moreover, some investigators suggest that plasmin/microplasmin-associated liquefaction is actually due to drug-related inflammation and that this change occurs several hours after plasmin exerts its effect on the vitreoretinal interface.Citation161 Such temporal separation of the two components of PVD induction may ultimately reduce efficacy. This combination of factors likely accounts for the surprisingly low rates of spontaneous PVD noted in human trials of plasmin and microplasmin, which were routinely less than 50%.Citation69,Citation77,Citation134,Citation152,Citation153 As no single agent currently appears sufficient for routine PVD production, the future of pharmacologic vitreolysis will likely involve the simultaneous administration of different agents with distinct roles in PVD production.Citation51,Citation90 Two in vivo pre-clinical studies, one in rabbitsCitation105 and the second in diabetic rats,Citation162 have utilized this approach with excellent results. In these studies, 80%–100% of eyes treated with a combination of hyaluronidase and plasmin/microplasmin achieved spontaneous PVD without adjunctive procedure compared with much lower rates in eyes treated with the individual agents alone (0%–12.5%). Future studies could explore the use of different doses and combinations of existing agents and could permit the application of agents previously found to be associated with significant toxicity as combination therapy may allow the use of lower doses. Other promising concepts deserving of further exploration include the use of nonenzymatic agents, which offer the potential for vitreolysis without collateral damage to adjacent ECM structures, and the identification of particular agents for specific clinical indications.
Disclosure
The authors report no conflicts of interest in this work.
References
- AkibaJQuirozMATrempeCLRole of posterior vitreous detachment in idiopathic macular holesOphthalmology19909712161016132087292
- JaffeNSVitreous traction at the posterior pole of the fundus due to alterations in the vitreous posteriorTrans Am Acad Ophthalmol Otolaryngol19677146426526052820
- RoldanMSerranoJMMacular edema and vitreous detachmentAnn Ophthalmol19892141411482729818
- NasrallahFPJalkhAEVan CoppenolleFThe role of the vitreous in diabetic macular edemaOphthalmology19889510133513393226682
- AkibaJArzabeCWTrempeCLPosterior vitreous detachment and neovascularization in diabetic retinopathyOphthalmology19909778898912381702
- AkibaJKadoMKakehashiATrempeCLRole of the vitreous in posterior segment neovascularization in central retinal vein occlusionOphthalmic Surg19912294985021945273
- RobisonCDKrebsIBinderSVitreomacular adhesion in active and end-stage age-related macular degenerationAm J Ophthalmol200914817982e7219327744
- JohnsonMWPerifoveal vitreous detachment and its macular complicationsTrans Am Ophthalmol Soc200510353756717057817
- JohnsonMWPosterior vitreous detachment: evolution and complications of its early stagesAm J Ophthalmol20101493371382.e37120172065
- RanchodTMGoldenbergDTTreseMTPharmacologic vitreodynamicsInt Ophthalmol Clin200949213514019349793
- ChuTGLopezPFCanoMRPosterior vitreoschisis. An echographic finding in proliferative diabetic retinopathyOphthalmology199610323153228594520
- MachemerRBuettnerHNortonEWParelJMVitrectomy: a pars plana approachTrans Am Acad Ophthalmol Otolaryngol19717548138205566980
- SonodaKHSakamotoTEnaidaHResidual vitreous cortex after surgical posterior vitreous separation visualized by intravitreous triamcinolone acetonideOphthalmology2004111222623015019367
- RussellSRHagemanGSOptic disc, foveal, and extrafoveal damage due to surgical separation of the vitreousArch Ophthalmol2001119111653165811709016
- GandorferAUlbigMKampikAPlasmin-assisted vitrectomy eliminates cortical vitreous remnantsEye (Lond)2002161959711913902
- SebagJGuptaPRosenRRGarciaPSadunAAMacular holes and macular pucker: the role of vitreoschisis as imaged by optical coherence tomography/scanning laser ophthalmoscopyTrans Am Ophthalmol Soc2007105121129 discussion 129–131.18427601
- HanDPAbramsGWAabergTMSurgical excision of the attached posterior hyaloidArch Ophthalmol1988106799810003390064
- VanderJFKleinerRA method for induction of posterior vitreous detachment during vitrectomyRetina19921221721731439247
- HaritoglouCEhrtOGassCAKristinNKampikAParacentral scotomata: a new finding after vitrectomy for idiopathic macular holeBr J Ophthalmol200185223123311159494
- ThresherRJEhrenbergMMachemerRGas-mediated vitreous compression: an experimental alternative to mechanized vitrectomyGraefes Arch Clin Exp Ophthalmol198422151921986489766
- MillerBMillerHRyanSJExperimental vitreous syneresisArch Ophthalmol19851039138513883929752
- LincoffHKreissigIJakobiecFIwamotoTVitoloJShapiroRGas vitrectomy in a primate modelGraefes Arch Clin Exp Ophthalmol198622432152173710176
- LunaJDArtalMNReviglioVEPelizzariMDiazHJuarezCPVitreoretinal alterations following laser in situ keratomileusis: clinical and experimental studiesGraefes Arch Clin Exp Ophthalmol2001239641642311561789
- VenkateshPVajpayeeRBGargSInduction of posterior vitreous separation using LASIK suction ring may have a potential role in the management of diabetic macular edemaMed Hypotheses20066661137113916481121
- SebagJPharmacologic vitreolysisRetina1998181139502274
- FouldsWSIs your vitreous really necessary? The role of the vitreous in the eye with particular reference to retinal attachment, detachment and the mode of action of vitreous substitutesEye (Lond)19871Pt 66416643331605
- BishopPNStructural macromolecules and supramolecular organisation of the vitreous gelProg Retin Eye Res200019332334410749380
- ShuiYBHolekampNMKramerBCThe gel state of the vitreous and ascorbate-dependent oxygen consumption: relationship to the etiology of nuclear cataractsArch Ophthalmol2009127447548219365028
- HolekampNMThe vitreous gel: more than meets the eyeAm J Ophthalmol20101491323619875090
- BishopPNVitreous as a substrate for vitreolysisDev Ophthalmol20094471919494647
- HindsonVJGallagherJTHalfterWBishopPNOpticin binds to heparan and chondroitin sulfate proteoglycansInvest Ophthalmol Vis Sci200546124417442316303928
- HeegaardSJensenOAPrauseJUStructure and composition of the inner limiting membrane of the retina. SEM on frozen resin-cracked and enzyme-digested retinas of Macaca mulattaGraefes Arch Clin Exp Ophthalmol198622443553603710190
- KohnoTSorgenteNIshibashiTGoodnightRRyanSJImmunofluorescent studies of fibronectin and laminin in the human eyeInvest Ophthalmol Vis Sci19872835065143549611
- PonsioenTLvan LuynMJvan der WorpRJvan MeursJCHooymansJMLosLICollagen distribution in the human vitreoretinal interfaceInvest Ophthalmol Vis Sci20084994089409518450587
- SebagJBalazsEAMorphology and ultrastructure of human vitreous fibersInvest Ophthalmol Vis Sci1989308186718712759801
- FoosRYVitreoretinal juncture; topographical variationsInvest Ophthalmol197211108018084561129
- WangJMcLeodDHensonDBBishopPNAge-dependent changes in the basal retinovitreous adhesionInvest Ophthalmol Vis Sci20034451793180012714607
- SebagJMolecular biology of pharmacologic vitreolysisTrans Am Ophthalmol Soc200510347349417057814
- TerranovaVPRohrbachDHMartinGRRole of laminin in the attachment of PAM 212 (epithelial) cells to basement membrane collagenCell19802237197267460011
- EngvallERuoslahtiEMillerEJAffinity of fibronectin to collagens of different genetic types and to fibrinogenJ Exp Med1978147615841595567240
- FoosRYWheelerNCVitreoretinal juncture. Synchysis senilis and posterior vitreous detachmentOphthalmology19828912150215127162795
- SebagJThe vitreous: structure, function, and pathobiologyNew YorkSpringer-Verlag1989
- KishiSShimizuKPosterior precortical vitreous pocketArch Ophthalmol199010879799822369358
- SebagJAge-related changes in human vitreous structureGraefes Arch Clin Exp Ophthalmol1987225289933583000
- O’MalleyPThe pattern of vitreous syneresis: a study of 800 autopsy eyesIrvineARO’MalleyCAdvances in vitreous surgerySpringfield, ILThomas19761733
- LarssonLOsterlinSPosterior vitreous detachment. A combined clinical and physiochemical studyGraefes Arch Clin Exp Ophthalmol1985223292954007512
- LinderBAcute posterior vitreous detachment and its retinal complicationsActa Ophthalmol196687Suppl1108
- SebagJAnomalous posterior vitreous detachment: a unifying concept in vitreo-retinal diseaseGraefes Arch Clin Exp Ophthalmol2004242869069815309558
- KlotiRExperimental occlusion of retinal and ciliary vessels in owl monkeys. I. Technique and clinical observations of selective embolism of the central retinal artery systemExp Eye Res1967643933996060551
- SebagJAge-related differences in the human vitreoretinal interfaceArch Ophthalmol199110979669712064577
- SebagJIs pharmacologic vitreolysis brewing?Retina20022211311884870
- UenoNSebagJHirokawaHChakrabartiBEffects of visible-light irradiation on vitreous structure in the presence of a photosensitizerExp Eye Res19874468638703653277
- AkibaJUenoNChakrabartiBMechanisms of photo-induced vitreous liquefactionCurr Eye Res19941375055127924415
- KakehashiAUenoNChakrabartiBMolecular mechanisms of photochemically induced posterior vitreous detachmentOphthalmic Res199426151598134089
- BrownDJBishopPHamdiHKenneyMCCleavage of structural components of mammalian vitreous by endogenous matrix metalloproteinase-2Curr Eye Res19961544394458717491
- Vaughan-ThomasAGilbertSJDuanceVCElevated levels of proteolytic enzymes in the aging human vitreousInvest Ophthalmol Vis Sci200041113299330411006217
- LosLIvan der WorpRJvan LuynMJHooymansJMAge-related liquefaction of the human vitreous body: LM and TEM evaluation of the role of proteoglycans and collagenInvest Ophthalmol Vis Sci20034472828283312824219
- MoorheadLCChuHHGarciaCAEnzyme-assisted vitrectomy with bacterial collagenase. Time course and toxicity studiesArch Ophthalmol198310122652746297438
- MoorheadLCRadtkeNEnzyme-assisted vitrectomy with bacterial collagenase. Pilot human studiesRetina198552981002996104
- MoorheadLCRedburnDAKirkpatrickDSKretzerFBacterial collagenase. Proposed adjunct to vitrectomy with membranectomyArch Ophthalmol19809810182918396252879
- VerstraetenTCChapmanCHartzerMWinklerBSTreseMTWilliamsGAPharmacologic induction of posterior vitreous detachment in the rabbitArch Ophthalmol199311168498548512489
- HarooniMMcMillanTRefojoMEfficacy and safety of enzymatic posterior vitreous detachment by intravitreal injection of hyaluronidaseRetina199818116229502276
- TezelTHDel PrioreLVKaplanHJPosterior vitreous detachment with dispaseRetina19981817159502275
- TreseMTEnzymatic-assisted vitrectomyEye (Lond)200216436536812101442
- TreseMTEnzymatic vitreous surgerySemin Ophthalmol200015211612111309736
- GandorferAPharmacologic vitreolysisDev Ophthalmol20073914915617245084
- GandorferAEnzymatic vitreous disruptionEye (Lond)200822101273127718292784
- BhisitkulRBAnticipation for enzymatic vitreolysisBr J Ophthalmol20018511211133700
- BenzMSPackoKHGonzalezVA placebo-controlled trial of microplasmin intravitreous injection to facilitate posterior vitreous detachment before vitrectomyOphthalmology2010117479179720138368
- HermelMPrennerJAlabdulrazzakMDaileyWHartzerMEffect of intravitreal plasmin on vitreous removal through a 25-gauge cutting system in the rabbit in vivoGraefes Arch Clin Exp Ophthalmol2009247333133419034484
- EckardtCTransconjunctival sutureless 23-gauge vitrectomyRetina200525220821115689813
- FujiiGYDe JuanEJrHumayunMSA new 25-gauge instrument system for transconjunctival sutureless vitrectomy surgeryOphthalmology20021091018071812 discussion 1813.12359598
- RamkissoonYDAslamSAShahSPWongSCSullivanPMRisk of iatrogenic peripheral retinal breaks in 20-G pars plana vitrectomyOphthalmology201011791825183020471685
- TanHSMuraMde SmetMDIatrogenic retinal breaks in 25-gauge macular surgeryAm J Ophthalmol2009148342743019477712
- HubschmanJPGuptaABourlaDHCuljatMYuFSchwartzSD20-, 23-, and 25-gauge vitreous cutters: performance and characteristics evaluationRetina200828224925718301030
- TeixeiraAChongLPMatsuokaNVitreoretinal traction created by conventional cutters during vitrectomyOphthalmology2010117713871392.e138220176400
- AsamiTTerasakiHKachiSUltrastructure of internal limiting membrane removed during plasmin-assisted vitrectomy from eyes with diabetic macular edemaOphthalmology2004111223123715019368
- BonnetMThe development of severe proliferative vitreoretinopathy after retinal detachment surgery. Grade B: a determining risk factorGraefes Arch Clin Exp Ophthalmol198822632012053402740
- CapeansCLorenzoJSantosLComparative study of incomplete posterior vitreous detachment as a risk factor for proliferative vitreoretinopathyGraefes Arch Clin Exp Ophthalmol199823674814859672792
- GandorferARohlederMGrosselfingerSHaritoglouCUlbigMKampikAEpiretinal pathology of diffuse diabetic macular edema associated with vitreomacular tractionAm J Ophthalmol2005139463865215808159
- TakahashiMTrempeCLMaguireKMcMeelJWVitreoretinal relationship in diabetic retinopathy. A biomicroscopic evaluationArch Ophthalmol19819922412457469858
- JalkhATakahashiMTopilowHWTrempeCLMcMeelJWPrognostic value of vitreous findings in diabetic retinopathyArch Ophthalmol198210034324347199900
- KadoMTrempeCLRole of the vitreous in branch retinal vein occlusionAm J Ophthalmol1988105120242447780
- HikichiTKonnoSTrempeCLRole of the vitreous in central retinal vein occlusionRetina199515129337754244
- AvundukAMCetinkayaKKapiciogluZKayaCThe effect of posterior vitreous detachment on the prognosis of branch retinal vein occlusionActa Ophthalmol Scand19977544414429374257
- KrebsIBrannathWGlittenbergCZeilerFSebagJBinderSPosterior vitreomacular adhesion: a potential risk factor for exudative age-related macular degeneration?Am J Ophthalmol2007144574174617884003
- LeeSJLeeCSKohHJPosterior vitreomacular adhesion and risk of exudative age-related macular degeneration: paired eye studyAm J Ophthalmol20091474621626.e62119159862
- KuppermannBDThomasELde SmetMDGrilloneLRPooled efficacy results from two multinational randomized controlled clinical trials of a single intravitreous injection of highly purified ovine hyaluronidase (Vitrase) for the management of vitreous hemorrhageAm J Ophthalmol2005140457358416125661
- KuppermannBDThomasELde SmetMDGrilloneLRSafety results of two phase III trials of an intravitreous injection of highly purified ovine hyaluronidase (Vitrase) for the management of vitreous hemorrhageAm J Ophthalmol2005140458559716226510
- SebagJPharmacologic vitreolysis – premise and promise of the first decadeRetina200929787187419584647
- MandlICollagenaseScience1970169951123412384317926
- O’NeillRSheaMThe effects of bacterial collagenase in rabbit vitreousCan J Ophthalmol1973823663704350501
- QuirozHBuzneySMFurukawaHEnzymatically induced posterior vitreous detachment [abstract]Invest Ophthalmol Vis Sci (Suppl)198425307
- PrabhakarVRamanRCapilaIBosquesCJPojasekKSasisekharanRBiochemical characterization of the chondroitinase ABC I active siteBiochem J2005390Pt 239540516108757
- HagemanGSRussellSRChondroitinase-mediated disinsertion of the primate vitreous body [abstract]Invest Ophthalmol Vis Sci (Suppl)1994351260
- BishopPNMcLeodDReardonAEffects of hyaluronan lyase, hyaluronidase, and chondroitin ABC lyase on mammalian vitreous gelInvest Ophthalmol Vis Sci199940102173217810476780
- StaubachFNoberVJanknechtPEnzyme-assisted vitrectomy in enucleated pig eyes: a comparison of hyaluronidase, chondroitinase, and plasminCurr Eye Res2004294–526126815590471
- HermelMSchrageNFEfficacy of plasmin enzymes and chondroitinase ABC in creating posterior vitreous separation in the pig: a masked, placebo-controlled in vivo studyGraefes Arch Clin Exp Ophthalmol2007245339940616900357
- LudowiegJVenneslandBDorfmanAThe mechanism of action of hyaluronidaseJ Biol Chem196123633333913764073
- MenzelEJFarrCHyaluronidase and its substrate hyaluronan: biochemistry, biological activities and therapeutic usesCancer Lett199813113119839614
- FouldsWSAllanDMoseleyHKylePMEffect of intravitreal hyaluronidase on the clearance of tritiated water from the vitreous to the choroidBr J Ophthalmol19856975295324016049
- GottliebJLAntoszykANHatchellDLSaloupisPThe safety of intravitreal hyaluronidase. A clinical and histologic studyInvest Ophthalmol Vis Sci19903111234523522242999
- KangSWHyungSMChoiMYLeeJInduction of vitreolysis and vitreous detachment with hyaluronidase and perfluoropropane gasKorean J Ophthalmol19959269788818320
- HikichiTKadoMYoshidaAIntravitreal injection of hyaluronidase cannot induce posterior vitreous detachment in the rabbitRetina200020219519810783954
- WangZ-LZhangXXuXSunX-DWangFPVD following plasmin but not hyaluronidase: implications for combination pharmacologic vitreolysis therapyRetina2005251384315655439
- StennKSLinkRMoellmannGMadriJKuklinskaEDispase, a neutral protease from Bacillus polymyxa, is a powerful fibronectinase and type IV collagenaseJ Invest Dermatol19899322872902546994
- FrenzelEMNeelyKAWalshAWCameronJDGregersonDSA new model of proliferative vitreoretinopathyInvest Ophthalmol Vis Sci19983911215721649761295
- KralingerMTKieselbachGFVoigtMExperimental model for proliferative vitreoretinopathy by intravitreal dispase: limited by zonulolysis and cataractOphthalmologica2006220421121616785750
- OliveiraLBTatebayashiMMahmoudTHBlackmonSMWongFMcCuenBW2ndDispase facilitates posterior vitreous detachment during vitrectomy in young pigsRetina200121432433111508877
- JorgeROyamaguchiEKCardilloJAGobbiALaicineEMHaddadAIntravitreal injection of dispase causes retinal hemorrhages in rabbit and human eyesCurr Eye Res200326210711212815529
- ZhuDChenHXuXEffects of intravitreal dispase on vitreoretinal interface in rabbitsCurr Eye Res2006311193594617114119
- WangFWangZSunXXuXZhangXSafety and efficacy of dispase and plasmin in pharmacologic vitreolysisInvest Ophthalmol Vis Sci20044593286329015326153
- SumiHHamadaHTsushimaHMiharaHMurakiHA novel fibrinolytic enzyme (nattokinase) in the vegetable cheese Natto; a typical and popular soybean food in the Japanese dietExperientia19874310111011113478223
- SumiHHamadaHNakanishiKHirataniHEnhancement of the fibrinolytic activity in plasma by oral administration of nattokinaseActa Haematol19908431391432123064
- UranoTIharaHUmemuraKThe profibrinolytic enzyme subtilisin NAT purified from Bacillus subtilis Cleaves and inactivates plasminogen activator inhibitor type 1J Biol Chem200127627246902469611325965
- TakanoAHirataAOgasawaraKPosterior vitreous detachment induced by nattokinase (subtilisin NAT): a novel enzyme for pharmacologic vitreolysisInvest Ophthalmol Vis Sci20064752075207916639018
- LiottaLAGoldfarbRHBrundageRSiegalGPTerranovaVGarbisaSEffect of plasminogen activator (urokinase), plasmin, and thrombin on glycoprotein and collagenous components of basement membraneCancer Res19814111 Pt 1462946366458354
- UemuraANakamuraMKachiSEffect of plasmin on laminin and fibronectin during plasmin-assisted vitrectomyArch Ophthalmol2005123220921315710817
- LiXShiXFanJPosterior vitreous detachment with plasmin in the isolated human eyeGraefes Arch Clin Exp Ophthalmol20022401566211954782
- TakanoAHirataAInomataYIntravitreal plasmin injection activates endogenous matrix metalloproteinase-2 in rabbit and human vitreousAm J Ophthalmol2005140465466016140249
- BaramovaENBajouKRemacleAInvolvement of PA/plasmin system in the processing of pro-MMP-9 and in the second step of pro-MMP-2 activationFEBS Lett199740521571629089282
- WachtfogelYTAbramsWKucichUWeinbaumGSchapiraMColmanRWFibronectin degradation products containing the cytoadhesive tetrapeptide stimulate human neutrophil degranulationJ Clin Invest1988815131013162966812
- HikichiTYanagiyaNKadoMAkibaJYoshidaAPosterior vitreous detachment induced by injection of plasmin and sulfur hexafluoride in the rabbit vitreousRetina1999191555810048374
- GandorferAPutzEWelge-LussenUGruterichMUlbigMKampikAUltrastructure of the vitreoretinal interface following plasmin assisted vitrectomyBr J Ophthalmol200185161011133703
- GandorferAPriglingerSSchebitzKVitreoretinal morphology of plasmin-treated human eyesAm J Ophthalmol2002133115615911755861
- MargherioARMargherioRRHartzerMTreseMTWilliamsGAFerronePJPlasmin enzyme-assisted vitrectomy in traumatic pediatric macular holesOphthalmology19981059161716209754166
- WuWCDrenserKATreseMTWilliamsGACaponeAPediatric traumatic macular hole: results of autologous plasmin enzyme-assisted vitrectomyAm J Ophthalmol2007144566867217870044
- TsukaharaYHondaSImaiHAutologous plasmin-assisted vitrectomy for stage 5 retinopathy of prematurity: a preliminary trialAm J Ophthalmol2007144113914117601440
- WuW-CDrenserKALaiMCaponeATreseMTPlasmin enzyme-assisted vitrectomy for primary and reoperated eyes with stage 5 retinopathy of prematurityRetina200828Suppl 3S75S8018317350
- WuW-CDrenserKACaponeAWilliamsGATreseMTPlasmin enzyme-assisted vitreoretinal surgery in congenital X-linked retinoschisis: surgical techniques based on a new classification systemRetina20072781079108518040249
- TreseMTWilliamsGAHartzerMKA new approach to stage 3 macular holesOphthalmology200010781607161110919918
- RizzoSPellegriniGBenocciFBeltingCBaicchiUVispiMAutologous plasmin for pharmacologic vitreolysis prepared 1 hour before surgeryRetina200626779279616963853
- SakumaTTanakaMInoueMMizotaASouriMIchinoseAEfficacy of autologous plasmin for idiopathic macular hole surgeryEur J Ophthalmol200515678779416329067
- AzzoliniCD’AngeloAMaestranziGIntrasurgical plasmin enzyme in diabetic macular edemaAm J Ophthalmol2004138456056615488781
- SakumaTTanakaMInoueJMizotaASouriMIchinoseAUse of autologous plasmin during vitrectomy for diabetic maculopathyEur J Ophthalmol200616113814016496258
- HirataATakanoAInomataYYonemuraNSagaraNTaniharaHPlasmin-assisted vitrectomy for management of proliferative membrane in proliferative diabetic retinopathy: a pilot studyRetina20072781074107818040248
- UdaondoPDiaz-LlopisMGarcia-DelpechSSalomDRomeroFJIntravitreal plasmin without vitrectomy for macular edema secondary to branch retinal vein occlusionArch Ophthalmol2011129328328721402982
- KameiMEstafanousMLewisHTissue plasminogen activator in the treatment of vitreoretinal diseasesSemin Ophthalmol2000151445010749314
- Glacet-BernardAKuhnDVineAKOubrahamHCoscasGSoubraneGTreatment of recent onset central retinal vein occlusion with intravitreal tissue plasminogen activator: a pilot studyBr J Ophthalmol200084660961310837386
- Le MerYKorobelnikJFMorelCUllernMBerrodJPTPA-assisted vitrectomy for proliferative diabetic retinopathy: results of a double-masked, multicenter trialRetina199919537838210546931
- EsserPHeimannKBartz-SchmidtKUWalterPKrottRWellerMPlasminogen in proliferative vitreoretinal disordersBr J Ophthalmol19978175905949290376
- HesseLNebelingBSchroederBHellerGKrollPInduction of posterior vitreous detachment in rabbits by intravitreal injection of tissue plasminogen activator following cryopexyExp Eye Res2000701313910644418
- UnalMPeymanGAThe efficacy of plasminogen-urokinase combination in inducing posterior vitreous detachmentRetina2000201697510696751
- MenGPeymanGAGenaidyMThe role of recombinant lysine-plasminogen and recombinant urokinase and sulfur hexafluoride combination in inducing posterior vitreous detachmentRetina200424219920915097878
- HesseLKrollPTPA-assisted vitrectomy for proliferative diabetic retinopathyRetina200020331731810872945
- MurakamiTTakagiHOhashiHRole of posterior vitreous detachment induced by intravitreal tissue plasminogen activator in macular edema with central retinal vein occlusionRetina20072781031103718040240
- NagaiNDemarsinEVan HoefBRecombinant human microplasmin: production and potential therapeutic propertiesJ Thromb Haemost20031230731312871505
- GandorferARohlederMSethiCPosterior vitreous detachment induced by microplasminInvest Ophthalmol Vis Sci200445264164714744909
- SakumaTTanakaMMizotaAInoueJPakolaSSafety of in vivo pharmacologic vitreolysis with recombinant microplasmin in rabbit eyesInvest Ophthalmol Vis Sci20054693295329916123432
- ChenWHuangXMaXWMoWWangWJSongHYEnzymatic vitreolysis with recombinant microplasminogen and tissue plasminogen activatorEye (Lond)200822230030717704761
- de SmetMDValmaggiaCZarranz-VenturaJWillekensBMicroplasmin: ex vivo characterization of its activity in porcine vitreousInvest Ophthalmol Vis Sci200950281481918806295
- de SmetMDGandorferAStalmansPMicroplasmin intravitreal administration in patients with vitreomacular traction scheduled for vitrectomy: the MIVI I trialOphthalmology20091167134913551355.e1341e134219447497
- StalmansPDelaeyCde SmetMDvan DijkmanEPakolaSIntravitreal injection of microplasmin for treatment of vitreomacular adhesion: results of a prospective, randomized, sham-controlled phase II trial (the MIVI-IIT trial)Retina20103071122112720616687
- DugelPUGroupM-TSA single injection of ocriplasmin for the treatment of symptomatic vitreomacular adhesion (sVMA): results of the Phase III MIVI-TRUST Program [abstract]Invest Ophthalmol Vis Sci (Suppl)2011526628
- HynesROIntegrins: versatility, modulation, and signaling in cell adhesionCell199269111251555235
- GehlsenKRArgravesWSPierschbacherMDRuoslahtiEInhibition of in vitro tumor cell invasion by Arg-Gly-Asp-containing synthetic peptidesJ Cell Biol198810639259302450101
- BremRBRobbinsSGWilsonDJImmunolocalization of integrins in the human retinaInvest Ophthalmol Vis Sci1994359346634748056522
- OliveiraLBMeyerCHKumarJRGD peptide-assisted vitrectomy to facilitate induction of a posterior vitreous detachment: a new principle in pharmacological vitreolysisCurr Eye Res200225633334012789539
- KarageozianHLDetermine the safety and efficacy of Vitreosolve® administered intravitreally to induce a complete posterior vitreous detachment (PVD) in non proliferative diabetic retinopathy human subjectsInvest Ophthalmol Vis Sci (Suppl)2005465453
- McLaughlinPSMcLaughlinBGChemical analysis of bovine and porcine vitreous humors: correlation of normal values with serum chemical values and changes with time and temperatureAm J Vet Res19874834674733565904
- GandorferAKampikAPharmacologic vitreolysis combining the two enzymes plasmin and hyaluronidaseRetina2005255674 author reply 674–675.16077373
- Zhi-LiangWWo-DongSMinLXiao-PingBJinJPharmacologic vitreolysis with plasmin and hyaluronidase in diabetic ratsRetina200929226927419050667