
Abstract
Preservatives used in topical glaucoma medications have a plethora of well-described toxic effects on the ocular surface. Such ocular toxicity is manifest clinically as ocular surface disease (OSD) and has been confirmed in epidemiologic, prospective clinical trials and studies in which patients are switched from preservative-added to preservative-free topical therapy. Such toxicity has implications not only for tolerability, but also for adherence and persistence with therapy that is known to be poor in glaucoma. Glaucoma medication is now widely available in preservative-free formulations, and the question arises as to which patients should receive preservative-free glaucoma therapy in preference to preservative-added medication. A case can be made for several subpopulations of patients who might particularly benefit from preservative-free medication: patients with existing OSD, older patients, younger adult patients, female patients, pediatric and juvenile patients, patients who work in air-conditioned environments or who use electronic screens frequently, patients with medical risk factors for OSD, patients in whom trabecular surgery may become indicated in the future, contact lens users, perhaps patients with Asian ethnicity and patients with severe or treatment-refractory glaucoma. Whilst arguments could be made for selecting patients for preservative-free medication on the basis of their existing risk of OSD, collectively, these patients form a significant proportion of the glaucoma patient population as a whole and, in the absence of any cost premium or positive indication for preservative-added medication, preservative-free glaucoma medication for all patients seems an appropriate strategy.
Introduction
Preservatives are added to topical ophthalmic preparation to prevent bacterial contamination. In many cases, they were required by regulatory authorities and pharmacopoeias, although alternative methods of avoiding contamination are now available. However, evidence has accumulated that while the acute toxicity of substances such as benzalkonium chloride (BAK), novel detergents (such as Polyquad) and peroxide derivatives (such as Oxyd) may have appeared acceptable in the past, long-term use causes serious deleterious effects on the ocular surface.Citation1–Citation5 Clinically, the effects of BAK generally manifest as ocular surface disease (OSD) that is common in glaucoma patients receiving long-term topical medication.Citation6–Citation8 Moreover, there is increasing evidence suggesting that the associated inflammation may jeopardize the outcome of glaucoma surgery.Citation9–Citation11
As a symptomless, but sight-threatening condition, glaucoma requires long-term, usually life-long treatment. In common with other insidious illnesses, gaining patient acceptance and adherence with treatment is essential if chronic deterioration and ultimate loss of vision is to be avoided. While a number of barriers to good adherence exist, the adverse effects of medication are among the most significant.Citation12–Citation14 Improvements in the tolerability of topical glaucoma medication are likely to have a beneficial effect on adherence as well as the quality of life of patients; indeed, preliminary evidence suggests that ameliorating OSD in glaucoma patients can improve their clinical outcome, and that adherence patterns established early in treatment improves long-term adherence.Citation15–Citation18 The objective of this review is to summarize current understanding of the toxicity of topical ocular therapy preservatives and to identify which patients would benefit from a switch to preservative-free glaucoma medication.
Preclinical studies
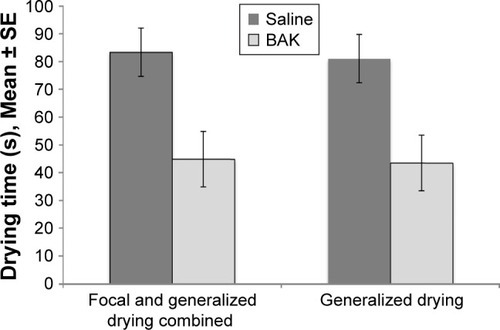
The ability of BAK to disrupt the tear film has been known for decades; in 1975, Wilson et alCitation19 showed that instillation of BAK-containing drops caused disruption of the tear film in both rabbits and humans (). Preservatives exert their toxic impact on the ocular surface by multiple mechanisms including cellular viability, apoptosis, neurotoxicity, effects on the trabecular network and damage to DNA.Citation1,Citation4,Citation7,Citation20–Citation22
Figure 1 Tear film disruption caused by instillation of a single drop of BAK (0.01%).
Abbreviation: BAK, benzalkonium chloride.
Although there have been criticisms of the evidence of BAK toxicity in preclinical studies (in particular, the concentrations of BAK employed),Citation23 the weight of evidence appears to support a significant toxic effect of BAK on the ocular surface.Citation1,Citation3,Citation4,Citation21
Clinical studies of BAK toxicity in glaucoma treatment
Epidemiologic studies
BAK toxicity has been identified in a number of epidemiologic studies conducted in glaucoma patients receiving topical therapy.Citation24–Citation29 The first published of these studies was in 1999, which showed that a number of symptoms were more common among 725 patients receiving preservative-added eye drops, rather than among 125 patients using preservative-free eye drops for treatment of their glaucoma. Discomfort or pain on instillation, presence of symptoms of ocular irritation and clinical conjunctival signs on ocular examination were all more common in patients using preservative-added eye drops than in those using preservative-free drops.Citation29
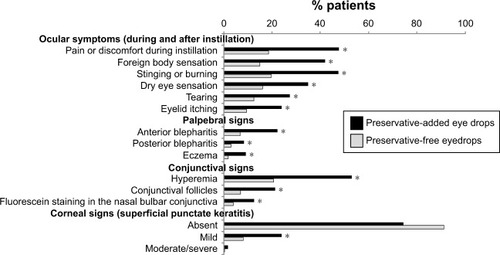
A multinational study examined patient-reported symptoms as well as palpebral, conjunctival and corneal signs in 9,658 patients using preservative-added or preservative-free beta-blocker eye drops. Preservative-added drops were used by 74% and preservative-free eye drops by 12% (combination therapy and unknown drop type accounted for the remainder).Citation25 Reported symptoms, as well as all palpebral, conjunctival and corneal signs were significantly more frequent in patients using preservative-containing drops than in those using preservative-free drops (). Patients who reduced their dosage or switched to preservative-free drops experienced a significant amelioration of their symptoms as well as clinical signs.
Figure 2 Ocular symptoms and signs with preservative-added and preservative-free glaucoma medications.
In addition to increased prevalence of symptoms and clinical signs in patients taking preservative-added compared with preservative-free eye drops, epidemiologic studies in subjects given BAK preservative-added eye drops have also demonstrated similar effects to those seen in animal experiments; increase in inflammatory markers, diminished goblet cells and impression cytology changes, suggestive of increased apoptosis, as well as corneal permeability changes were observed.Citation30–Citation33
Prospective studies
The epidemiologic studies described above suggest that BAK has toxicity properties that may be relevant in patients, but prospective studies provide yet more convincing evidence.
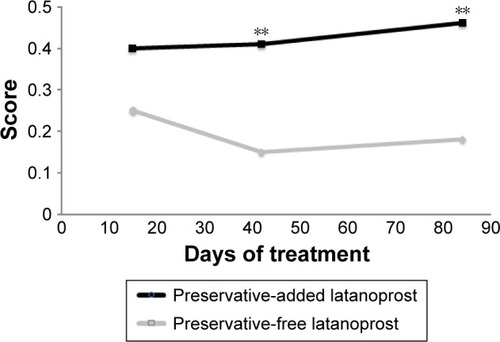
A multicenter, international, prospective, investigator-masked study compared preservative-added and preservative-free latanoprost eye drops in two parallel groups of glaucoma patients.Citation34 Although there was no disadvantage for the preservative-free eye drops in terms of efficacy, there were statistically significant tolerability advantages. Conjunctival hyperemia, subjective symptoms upon instillation and subjective symptoms between instillations were all significantly diminished in patients using preservative-free latanoprost, compared with the preservative-added product. There was a tendency for symptoms to worsen during treatment with the preservative-added eye drops, but to improve when patients were switched to the preservative-free medication. For example, the proportion of patients with moderate to severe conjunctival hyperemia increased almost threefold during the 84 days of study in the patients receiving preservative-added latanoprost eye drops, but fell by 35% in those receiving preservative-free latanoprost eye drops (). Similarly, although the differences were not large, total ocular symptom scores fell slightly in the preservative-free group and increased in the preservative-added eye drops group. Symptoms on instillation of eye drops (comprising pruritus, burning/stinging, blurred vision, sticky eye sensation, eye dryness sensation, foreign body sensation) expressed as a score were significantly reduced from day 42 onward (). Such benefits in tolerability are likely to be reflected in improved adherence.Citation15–Citation17
Figure 3 Hyperemia in patients receiving preservative-added or preservative-free glaucoma medication.
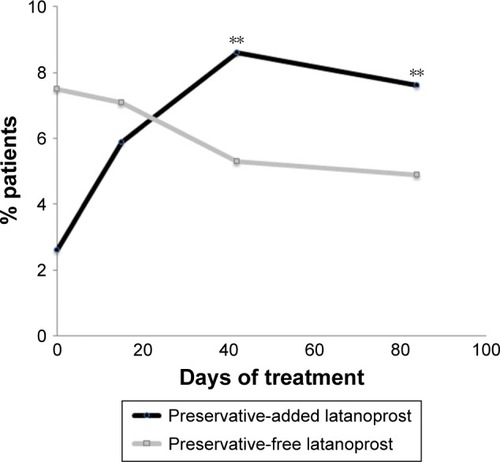
Figure 4 Ocular signs and symptoms in patients receiving preservative-added or preservative-free glaucoma medication.
A recent prospective study, in which 40 glaucoma patients were randomized to preservative-added or preservative-free timolol preparations, confirmed the toxicity of BAK preservative-added glaucoma medication.Citation35 After 12 months, intraepithelial goblet cell density was significantly lower in patients who received preservative-added medication compared with those who received preservative-free medication (48.3 vs 86.8) or controls (88.9). Tear break-up time (BUT) was curtailed in patients who received preservative-added timolol compared with those who received preservative-free timolol (8.12 vs 11.27 s) or controls (12.10 s).
Switch studies
1999
If the toxicity differences between preservative-added and preservative-free medications apparent from laboratory studies and observed in epidemiologic and prospective studies are of genuine clinical significance, then it should be possible to observe improvements in patients’ symptoms and adherence when their medication is switched from a preservative-added to a preservative-free formulation. There have been a number of such “switch studies” that have shown this to be the case. The first of these, although not originally conceived as a switch study, was undertaken by Levrat et al.Citation29 This epidemiologic survey of 919 patients of 125 French ophthalmologists was an early indication of the toxic effects of BAK in glaucoma medication. However, data were also collected on 164 patients who switched from preservative-added to preservative-free eye drops and at a mean follow-up of 3.3 months, the incidence of reported symptoms and objective signs had statistically significantly diminished by threefold to fourfold.
2003
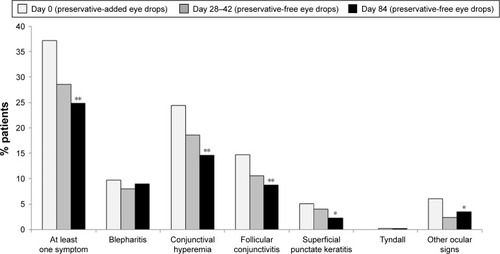
A prospective open clinical trial in which 435 patients with glaucoma or ocular hypertension were switched from BAK preservative-added timolol to the same regimen of preservative-free timolol demonstrated statistically significant reductions in symptoms and clinical signs on or between instillation ( and ).Citation26
Figure 5 Reduction in ocular symptoms following switch from preservative-added eye drops to preservative-free eye drops.
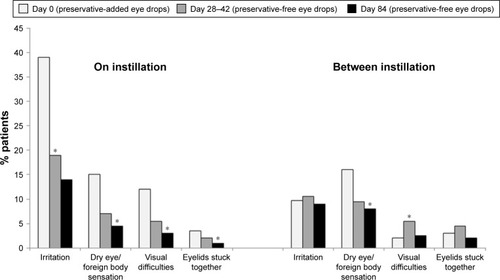
Figure 6 Reduction in clinical signs following switch from preservative-added to preservative-free eye drops.
2010
OSD improved significantly among 678 glaucoma or ocular hypertension patients switched from preservative-added to preservative-free glaucoma medication in a prospective, double-masked, randomized controlled, 12-week trial.Citation36 Intraocular pressure (IOP) was not significantly different between preservative-added and preservative-free groups.
2014
Switching from a preservative-added to a preservative-free preparation had no deleterious effects on IOP. An interesting recent studyCitation15 describes a series of four patients with open-angle glaucoma that was poorly controlled by their current preservative-added medication. All patients reported ocular discomfort and all had previously unrecognized OSD. Modification of their treatment to control OSD, including switching to preservative-free glaucoma medication and intensive treatment of the OSD, not only markedly improved symptomatic and clinical signs of OSD, but also resulted in a clinically significant improvement in IOP control.
In a recent open prospective study, a switch from preservative-added to preservative-free glaucoma medication resulted in improvements in corneal and conjunctival staining, erythema, conjunctival hyperemia and follicular hyperplasia, as well as in Schirmer’s test and tear BUT, which were associated with reduction in reports of dry eye and foreign body sensation. Improvements in IOP were not compromised by the switch to preservative-free medication.Citation37
2016
A combined analysis of two Phase III clinical trials in which glaucoma patients were switched from a preservative-added prostaglandin to a preservative-free prostaglandin medication showed reductions of two thirds in the incidence of ocular surface symptoms (irritation/burning/stinging, foreign body sensation, tearing, itching and dry eye sensation) and a halving of the incidence of blepharitis, abnormal staining and conjunctival hyperemia. A large majority of patients preferred the preservative-free preparation.Citation38
Studies in which patients are switched from preservative-added to preservative-free topical medication provide compelling evidence not only for the clinical toxicity of BAK preservative-added eye drops, but also that such toxicity can be ameliorated or avoided by adopting preservative-free medications in favor of BAK preparations. Importantly, all of the studies show that switching to a preservative-free formulation did not compromise IOP control. While improving tolerability is a laudable objective in its own right, in the context of glaucoma treatment, it has even more important implications in improving adherence and long-term visual outcome.
Adherence, persistence and quality of life
Adherence and persistence with glaucoma treatment is notoriously poor, particularly among patients new to therapy and, as any ophthalmologist will recognize, is a major barrier to the effective management of IOP.Citation12,Citation39–Citation41 In clinical trials, topical adverse effects are the most common reason for drop-out and are a significant source of poor adherence in clinical situations as well.Citation42,Citation43 A recent study completed in Singapore links adherence with quality of life in glaucoma patients.Citation44 Topical adverse events are among the most frequently reported reasons for treatment switching therapy and, as the foregoing discussion shows, it is now recognized that preservatives are responsible for at least some, and possibly most, of these local adverse events and that removing the preservative from the patient’s medication can improve both quality of life and adherence to treatment.Citation1,Citation45–Citation47
Direct evidence for the improvement in quality of life that can be achieved by a switch from a preservative-added to preservative-free therapy in glaucoma comes from a recent study in which patients were switched to a preservative-free medication and their quality of life was determined using the Glaucoma Symptom Scale. Scores for symptoms and functioning improved significantly after 8 weeks following the switch.Citation48
Ameliorating patients’ symptoms and improving quality of life are worthwhile goals for the clinician; however, they are yet more important if they can improve adherence and persistence with therapy and ultimately preserve the patient’s vision.
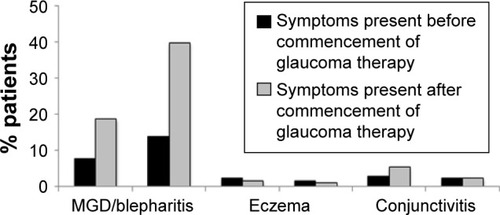
Patient satisfaction with treatment can be considered an overarching parameter that measures patients’ attitude to their medication. A recent study of patient satisfaction with glaucoma treatment showed that, while most patients were satisfied with their treatment, factors significantly associated with dissatisfaction included the presence of OSD, hyperemia, ocular signs, symptoms during and between instillation and the use of tear substitutes. The study also illustrated the frequency of ocular symptoms () and their onset with the commencement of glaucoma therapy ().Citation49
Figure 7 Proportion of patients experiencing symptoms between eye drop instillations.
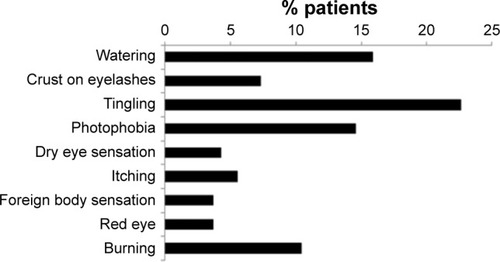
Figure 8 Emergence of ocular symptoms on commencement of glaucoma treatment.
Abbreviation: MGD, meibomian gland dysfunction.
Effects of preservatives on other aspects of glaucoma treatment
It seems clear that preservatives in eye drops can be the cause of both hyperemia and OSD in glaucoma patients. Dry eye can interfere with glaucoma diagnostic tests and deleteriously affect the long-term outcome of trabeculectomy.Citation10,Citation50,Citation51
Patients undergoing topical glaucoma therapy have reduced corneal (and conjunctival) sensitivity.Citation52 A number of studies have suggested that preservatives are responsible for neurotoxic effects in the cornea; for example, reduction in corneal sensitivity in glaucoma patients correlates with the frequency of instillation of preservative-added treatments.Citation53 Supporting this contention is the finding that stromal nerve fibers are significantly reduced in mice treated with BAK-containing eye drops. Moreover, in human studies, sub-basal nerve density is reduced in patients treated with preservative-added eye drops compared with that in patients treated with preservative-free eye drops and in untreated control subjects.Citation54,Citation55 Such a diminution of corneal sensitivity may explain why glaucoma patients frequently have clinical signs of OSD on examination, yet remain satisfied with their treatment and do not volunteer symptoms.Citation49
The study of Martone et al described above additionally investigated a suite of parameters among control subjects, glaucoma patients treated with preservative-free eye drops and those given preservative-added eye drops.Citation55 The study showed significantly better clinical scores for Schirmer test, esthesiometry and tear BUT in preservative-free-treated patients than in those given preservative-added medication. IOP was controlled equally well by preservative-free and preservative-added medication. Confocal microscopy examination showed advantages for preservative-free vs preservative-added medication in a number of parameters, though not all achieved statistical significance.
Indeed, the apoptotic effects of BAK may even promote glaucomatous changes in the eye or antagonize the effects of glaucoma medication by its effects on apoptosis in trabecular cells.Citation56–Citation61
Preservative-free glaucoma therapy for which patients?
Because of the more widespread availability of preservative-free formulations of topical glaucoma medications, consideration needs to be given as to which patients would most benefit from being switched to a preservative-free formulation. A number of patient subgroups can be identified who are at higher risk of OSD, or in whom OSD would be particularly unwelcome.
Newly diagnosed patients with pre-existing OSD
Glaucoma and OSD are commonly comorbid conditions; in some cases, a glaucoma patient’s OSD may be related to their glaucoma medication, but OSD can be present in treatment-naive patients. In addition, OSD, dry eye and glaucoma are all diseases typically more prevalent in older patients.Citation62–Citation65 Exacerbating OSD in such patients can be avoided by starting them on topical therapy that excludes the preservatives that can result in ocular surface toxicity during the long-term treatment the patients will likely require.
Elderly
Glaucoma is a progressive disease and is not only more common in the elderly, but in its later stages, it also often requires the use of more frequent application of eye drops and/or the use of multiple medications, thus increasing the risk of precipitating OSD.
A number of epidemiologic and other studies have demonstrated the increased risk of OSD in older patients.Citation62,Citation66–Citation69 The aging eye is susceptible to OSD for a number of pathophysiologic reasons including functional changes in the lacrimal glands, meibomian glands and goblet cells. Perhaps most importantly, aging is one of the most important risk factors for meibomian gland dysfunction (MGD).Citation70 Consequent changes in the composition of the tear film give rise to a propensity to inflammation.Citation71,Citation72 Anatomic changes such as conjunctivochalasis and eyelid laxity, more common in older populations, also predispose to OSD.Citation71,Citation72 Elderly patients may also be more sensitive to the effects of OSD than the younger patient populations.
Younger patients
Although predominantly a disease of older age, glaucoma can occur in individuals below the age of 40 years. Early-onset glaucoma is generally more difficult to treat and progresses more rapidly than glaucoma arising in older patients.Citation73 Consequently, younger patients tend to be treated more aggressively. Because glaucoma requires long-term, normally life-long therapy, younger patients with extended life expectancy will be exposed for a longer period of time to the cumulative toxicity of preservatives in their medication. Avoiding extended exposure may prevent the development of ocular symptoms and aid adherence and persistence in younger patients.
Pediatric and juvenile patients
Glaucoma is relatively uncommon in pediatric and juvenile patients and is generally treated by surgical methods.Citation74 However, topical medications are used prior to surgery and in those patients whose IOP is not adequately controlled following surgery. Clearly, such patients face many years of topical therapy, during which ocular surface toxicity is unwelcome and likely to impact adherence and persistence. Moreover, as discussed previously, OSD precipitated by the preservatives in topical glaucoma medication may impair the outcome of trabecular surgery.Citation9,Citation50
Work/leisure environments
Many offices and other workplaces are air-conditioned and, while the low humidity air and draft provided in these environments make the individuals physically comfortable, it can increase evaporative losses from their ocular surface and predispose them to dry eye. Other individuals (aircraft cabin staff, frequent air travelers, workers in arid environments, professional drivers) can be at risk from overexposure to draft and desiccated atmospheres.Citation75–Citation78
The use of electronic displays for both work and leisure is close to universal in the developed world and increasing in the developing world. Dry eye is a significant component of an established computer vision syndrome that also includes ocular discomfort, headache, eyestrain and temporary difficulties in accommodation.Citation79,Citation80 Both blink rate and blink amplitude are reduced during the use of display screens, increasing the susceptibility to evaporation of the ocular film, especially where, as is frequently the case, such screens are used in desiccated air-conditioned work environments.Citation80 Moreover, there may be a relationship between blink rate and MGD that further exacerbates OSD in habitual computer screen users.Citation81 Frequent computer use is itself associated with MGD.Citation82
Patients with medical risk factors
A number of other medical conditions are associated with dry eye; collagen vascular disease, refractive surgery, hematopoietic stem cell transplantation, vitamin A deficiency and androgen insufficiency have high levels of evidence for an association with dry eye, while diabetes mellitus, human immunodeficiency virus infection, systemic chemotherapy, some types of cataract surgery, keratoplasty, sarcoidosis and ovarian dysfunction are also candidate risk factors with at least moderate evidence.Citation62,Citation83 Dry eye can also be iatrogenic; there is at least moderately strong evidence showing antihistamines, some antidepressants, diuretics and beta-blockers as risk factors for dry eye. While cancer itself is not a risk factor for dry eye, radiation therapy and some types of systemic chemotherapy are.Citation62,Citation83
Similarly, MGD has been associated with a number of medical treatments including antihistamines, antidepressants, antiandrogens and isotretinoin drugs used for treating benign prostatic hyperplasia.Citation64 The degree of overlap between those drugs identified as potential risk factors for dry eye and those associated with MGD is notable. The list of medical conditions that may be associated with MGD is long, but includes androgen deficiency, atopy (and perhaps associated antihistamine use), benign prostatic hyperplasia, hypertension, menopause, Parkinson’s disease, rosacea, Sjögren’s syndrome and others.Citation64
Clearly, there is a wide range of medical conditions and medical treatments that put patients at increased risk of OSD. Many of these conditions are more prevalent among older patients and, therefore, frequently comorbid with glaucoma. Avoiding preservatives in the glaucoma medication of patients already at risk of OSD because of pre-existing medical conditions or those that develop during the course of their glaucoma treatment would seem to be the responsible course of action.
Presurgical patients
Trabeculotomy or filtration surgery is a common procedure used in patients in whom topical glaucoma therapy does not adequately control IOP or in those who fail to tolerate topical medication sufficiently well. A link between impaired outcome of trabecular surgery and long-term topical therapy has long been suspected.Citation9,Citation50 The role of toxic effects of preservatives in precipitating inflammatory and fibrotic changes in the ocular surface is now well recognized and some of the mechanisms have been elucidated.Citation28,Citation84–Citation88 It would thus seem reasonable that patients in whom filtration surgery might become indicated in the future be spared the additional risk of a poor surgical outcome by using preservative-free, rather than preservative-added medication in the initial stages of their illness.
Women
Dry eye is more common in women, particularly after menopause when there is a specific increase in MGD.Citation68,Citation89–Citation91 A dichotomy appears to exist regarding the benefit of hormone replacement therapy in improving the condition of the ocular surface in postmenopausal women; some studies have identified an improvement with hormone replacement therapy.Citation92–Citation96 On the other hand, The International Workshop on Meibomian Gland Dysfunction identified both menopause and hormone replacement therapy as risk factors for MGD.Citation64 The Dry Eye Workshop identified hormone replacement as a risk factor, but although older age and female sex were risk factors with consistent evidence, the evidence for menopause per se was deemed as “unclear”.Citation62 A possible explanation is that, estrogen may be a risk factor for OSD in premenopausal women, but that the loss of circulating androgens (androgen deficiency being a well-established risk factor) at menopause may be responsible for the postmenopausal increase in OSD.
Regardless of the mechanism, it is clear that women, older women in particular, are at higher risk of OSD than men, and that avoidance of preservative-induced toxicity would be of benefit in this population.
Contact lens use
The use of contact lenses is very common and is a frequent cause of dry eye, with around half of all contact lens wearers reporting symptoms of dry eye.Citation97 Similarly, MGD is more common among contact lens wearers than the population at large, although whether this association is causal or not remains unclear.Citation64 Nevertheless, contact lens use is a risk factor for OSD and the precautionary principle suggests avoiding additional risk in these patients by excluding preservatives from their topical glaucoma medication.
Ethnicity
Although methodological inconsistences exist between studies, a number of studies suggest that the prevalence of MGD is considerably higher among Asian populations than Caucasians.Citation64 A higher rate of dry eye in Asian populations is also supported by suggestive evidence.Citation62
Glaucoma
Although the severity or type of glaucoma is not known to be a risk factor for the development of OSD, patients with higher IOP are more likely to receive more frequent eye drops or treatment with more than one agent, both of which are known to be associated with an increased risk of dry eye.Citation8,Citation16 Patients receiving frequent instillations or multidrug therapy for severe glaucoma could usefully be considered for a switch to preservative-free medication.
Conclusion
There are a number of risk factors that can predispose to OSD among glaucoma patients: long treatment duration, age, sex, working and leisure environments, multiple medical comorbidities and their associated medication, and ethnicity. In such patients, it seems reasonable to avoid an additional risk of OSD caused by exposing them to the preservatives in their glaucoma therapy.
At first sight, there seems little medical rationale to choose a preservative-added medication over a preservative-free alternative. There have been suggestions that BAK enhances the penetration of active molecules into deeper ocular structures.Citation98 However, this phenomenon is better considered as histologic toxicity, rather than a means of improving penetration; in any case, acute pharmacodynamic effects are not necessarily indicative of conditions during chronic sustained treatment.Citation1 Until recently, the cost associated with single-dose or preservative-free multidose containers was a significant barrier to the use of preservative-free eye drops. However, preservative-free formulations are now widely available and often at little or no cost premium over preservative-added alternatives. Health economic studies comparing preservative-added and preservative-free glaucoma medications are lacking; but given an equivalent cost of acquisition, it seems likely that preservative-free formulations would have an advantage in cost-effectiveness (better persistence and adherence) and fewer consultations for OSD.
There are a number of reasons to choose a preservative-free topical therapy for glaucoma over a preservative-added treatment: improvements in patients’ quality of life, better adherence and persistence with therapy, and improving the outcome of trabecular surgery. The question arises as to which patients to choose for preservative-free treatment. However, perhaps the better question is: for which patients would an ophthalmologist choose to prescribe a preservative-added medication?
Disclosure
The author reports no conflicts of interest in this work.
References
- BaudouinCLabbéALiangHPaulyABrignole-BaudouinFPreservatives in eyedrops: the good, the bad and the uglyProg Retin Eye Res201029431233420302969
- MeloniMPaulyAServiBDVarletBLBaudouinCOccludin gene expression as an early in vitro sign for mild eye irritation assessmentToxicol In Vitro201024127628519729060
- ActisAGRolleTOcular surface alterations and topical antiglaucomatous therapy: a reviewOpen Ophthalmol J20148677225317218
- Aguayo BonniardAYeungJYChanCCBirtCMOcular surface toxicity from glaucoma topical medications and associated preservatives such as benzalkonium chloride (BAK)Expert Opin Drug Metab Toxicol2016121112791289
- FreemanDPKahookMYPreservatives in topical ophthalmic medications: historical and clinical perspectivesExpert Rev Ophthalmol2009415964
- LeungEWMedeirosFAWeinrebRNPrevalence of ocular surface disease in glaucoma patientsJ Glaucoma200817535035518703943
- AnwarZWellikSRGalorAGlaucoma therapy and ocular surface disease: current literature and recommendationsCurr Opin Ophthalmol201324213614323542350
- FechtnerRDGodfreyDGBudenzDStewartJAStewartWCJasekMCPrevalence of ocular surface complaints in patients with glaucoma using topical intraocular pressure-lowering medicationsCornea201029661862120386433
- BroadwayDCGriersonIO’BrienCHitchingsRAAdverse effects of topical antiglaucoma medication. II. The outcome of filtration surgeryArch Ophthalmol199411211144614547980134
- BaudouinCOcular surface and external filtration surgery: mutual relationshipsDev Ophthalmol201250647822517174
- MovahedanADjalilianARCataract surgery in the face of ocular surface diseaseCurr Opin Ophthalmol2012231687222081034
- NordstromBLFriedmanDSMozaffariEQuigleyHAWalkerAMPersistence and adherence with topical glaucoma therapyAm J Ophthalmol2005140459860616226511
- KastelanSTomicMMetez SoldoKSalopek-RabaticJHow ocular surface disease impacts the glaucoma treatment outcomeBiomed Res Int2013201369632824224176
- Cohen CastelOKeinan-BokerLGeyerOMilmanUKarkabiKFactors associated with adherence to glaucoma pharmacotherapy in the primary care settingFam Pract201431445346124927725
- BaudouinCBechetoilleABronAIntérêt de la mesure de la qualité de vie (QDV) et de l’observance thérapeutique chez les patients atteints de glaucome chronique à angle ouvert. [Relevance of quality of life and treatment compliance measurement in patients with chronic open-angle glaucoma]J Fr Ophtalmol2000231010571064 French11139707
- RossiGCTinelliCPasinettiGMMilanoGBianchiPEDry eye syndrome-related quality of life in glaucoma patientsEur J Ophthalmol200919457257919551671
- BatraRTailorRMohamedSOcular surface disease exacerbated glaucoma: optimizing the ocular surface improves intraocular pressure controlJ Glaucoma2014231566022828007
- Newman-CaseyPABlachleyTLeePPHeislerMFarrisKBSteinJDPatterns of glaucoma medication adherence over four years of follow-upOphthalmology2015122102010202126319441
- WilsonWSDuncanAJJayJLEffect of benzalkonium chloride on the stability of the precorneal tear film in rabbit and manBr J Ophthalmol197559116676691203224
- ChibretHToxicité oculaire du benzalkonium. [Ocular toxicity of benzalkonium]Ann Pharm Fr2011692108115 French21440103
- HuangCChenWChenYLiuZToxicity research status of benzalkonium chloride on ocular surfaceZhonghua Yan Ke Za Zhi2014504303306 Chinese24931157
- BaudouinCDetrimental effect of preservatives in eyedrops: implications for the treatment of glaucomaActa Ophthalmol200886771672618537937
- TresslerCSBeattyRLempMAPreservative use in topical glaucoma medicationsOcul Surf20119314015821791189
- PisellaPJPouliquenPBaudouinCPrevalence of ocular symptoms and signs with preserved and preservative free glaucoma medicationBr J Ophthalmol200286441842311914211
- JaenenNBaudouinCPouliquenPManniGFigueiredoAZeyenTOcular symptoms and signs with preserved and preservative-free glaucoma medicationsEur J Ophthalmol200717334134917534814
- BronAChiambarettaFPouliquenPRigalDRoulandJFEfficacy and safety of substituting a twice-daily regimen of timolol with a single daily instillation of nonpreserved beta-blocker in patients with chronic glaucoma or ocular hypertensionJ Fr Ophtalmol200326766867413130253
- RoulandJFEtude CARAT: acceptabilité d’un collyre bêtabloquant sans conservateur dans le traitement du glaucome. [Acceptability of preservative-free beta-blocker eye drops in the treatment of glaucoma]Réflexions Ophtalmologiques20111504346 French
- Van WentCBrasnuEHamardPBaudouinCLabbéAInfluence des pathologies de la surface oculaire sur le traitement du glaucome. [The influence of ocular surface diseases in the management of glaucoma]J Fr Ophtalmol2011344230237 French21439676
- LevratFPisellaPJBaudouinCTolérance clinique des collyres antiglaucomateux conservés et non conservés. Résultats d’une enquête inédite en Europe. [Clinical tolerance of antiglaucoma eyedrops with and without a preservative. Results of an unpublished survey in Europe]J Fr Ophtalmol1999222186191 French10327349
- CampagnaPMacriARolandoMChronic topical eye preservative-free beta-blocker therapy effect on the ocular surface in glaucomatous patientsActa Ophthalmol Scand (Suppl)199775S22453
- PisellaPJLalaEParierVRetentissement conjonctival des conservateurs: étude comparative de collyres bêta-bloquants conservés et non conservés chez des patients glaucomateux. [Effect of preservatives on the conjunctiva: a comparative study of beta-blocker eye drops with and without preservatives in glaucoma patients]J Fr Ophtalmol2003267675679 French13130254
- PisellaPJDebbaschCHamardPConjunctival proinflammatory and proapoptotic effects of latanoprost and preserved and unpreserved timolol: an ex vivo and in vitro studyInvest Ophthalmol Vis Sci20044551360136815111589
- BursteinNLPreservative alteration of corneal permeability in humans and rabbitsInvest Ophthalmol Vis Sci19842512145314576511230
- RoulandJFTraversoCEStalmansIT2345 Study GroupEfficacy and safety of preservative-free latanoprost eyedrops, compared with BAK-preserved latanoprost in patients with ocular hypertension or glaucomaBr J Ophthalmol201397219620023203707
- FrezzottiPFogagnoloPHakaGIn vivo confocal microscopy of conjunctiva in preservative-free timolol 0.1% gel formulation therapy for glaucomaActa Ophthalmol2014922e133e14024020826
- KatzGSpringsCLCravenERMontecchi-PalmerMOcular surface disease in patients with glaucoma or ocular hypertension treated with either BAK-preserved latanoprost or BAK-free travoprostClin Ophthalmol201041253126121151330
- IesterMTelaniSFrezzottiPOcular surface changes in glaucomatous patients treated with and without preservatives beta-blockersJ Ocul Pharmacol Ther201430647648124787056
- UusitaloHEgorovEKaarnirantaKAstakhovYRopoABenefits of switching from latanoprost to preservative-free tafluprost eye drops: a meta-analysis of two Phase IIIb clinical trialsClin Ophthalmol20161044545427041987
- ReardonGKotakSSchwartzGFObjective assessment of compliance and persistence among patients treated for glaucoma and ocular hypertension: a systematic reviewPatient Prefer Adherence2011544146322003282
- GurwitzJHGlynnRJMonaneMEverittDEGildenDSmithNAvornJTreatment for glaucoma: adherence by the elderlyAm J Public Health19938357117168484454
- YeawJBennerJSWaltJGSianSSmithDBComparing adherence and persistence across 6 chronic medication classesJ Manag Care Pharm200915972874019954264
- StewartWCDemosCMTurnerMKStewartJARisk factors for subject withdrawals in clinical trials evaluating glaucoma medicationsGraefes Arch Clin Exp Ophthalmol201024871007101220213475
- NordmannJPAuzanneauNRicardSBerdeauxGVision related quality of life and topical glaucoma treatment side effectsHealth Qual Life Outcomes2003117514667241
- LoonSCJinJJin GohMThe relationship between quality of life and adherence to medication in glaucoma patients in SingaporeJ Glaucoma2015245e36e4224248002
- OdbergTJakobsenJEHultgrenSJHalseideRThe impact of glaucoma on the quality of life of patients in Norway. I. Results from a self-administered questionnaireActa Ophthalmol Scand200179211612011284746
- BayerAWeilerWOeverhausUSkrotzkiFEStewartWCXplore Observation GroupTwo-year follow-up of latanoprost 0.005% monotherapy after changing from previous glaucoma therapiesJ Ocul Pharmacol Ther200420647047815684807
- NordmannJPAkesbiJAméliorer l’adhérence au traitement des patients glaucomateux : le rôle du médecin. [Improve adherence in glaucoma patients: a doctor’s duty]J Fr Ophtalmol2011346403408 French21652110
- Abegão PintoLVandewalleEGerlierLStalmansIImprovement in glaucoma patient quality of life by therapy switch to preservative-free timolol/dorzolamide fixed combinationOphthalmologica2014231316617124401549
- LemijHGHoevenaarsJGvan der WindtCBaudouinCPatient satisfaction with glaucoma therapy: reality or myth?Clin Ophthalmol2015978579325999687
- RüferFErbCEinflüsse des trockenen Auges auf die Glaukomdiagnostik. [Influence of dry eye syndrome on glaucoma diagnostic procedures]Ophthalmologe20121091110821086 German23179813
- BroadwayDCChangLPTrabeculectomy, risk factors for failure and the preoperative state of the conjunctivaJ Glaucoma200110323724911442190
- Romero-Díaz de LeónLMorales-LeónJELedesma-GilJNavasAConjunctival and corneal sensitivity in patients under topical antiglaucoma treatmentInt Ophthalmol201636329930326272426
- Van WentCAlalwaniHBrasnuEÉvaluation de la sensibilité cornéenne chez les patients traités médicalement pour un glaucome ou une hypertonie oculaire. [Corneal sensitivity in patients treated medically for glaucoma or ocular hypertension]J Fr Ophtalmol20113410684690 French22093372
- SarkarJChaudharySNamavariACorneal neurotoxicity due to topical benzalkonium chlorideInvest Ophthalmol Vis Sci20125341792180222410563
- MartoneGFrezzottiPTosiGMAn in vivo confocal microscopy analysis of effects of topical antiglaucoma therapy with preservative on corneal innervation and morphologyAm J Ophthalmol20091474725735.e119181302
- LinZLiuXZhouTA mouse dry eye model induced by topical administration of benzalkonium chlorideMol Vis20111725726421283525
- De Saint JeanMBrignoleFBringuierAFBauchetAFeldmannGBaudouinCEffects of benzalkonium chloride on growth and survival of Chang conjunctival cellsInvest Ophthalmol Vis Sci199940361963010067965
- BuronNMicheauOCathelinSLafontainePOCreuzot-GarcherCSolaryEDifferential mechanisms of conjunctival cell death induction by ultraviolet irradiation and benzalkonium chlorideInvest Ophthalmol Vis Sci200647104221423017003409
- HamardPBlondinCDebbaschCWarnetJMBaudouinCBrignoleFIn vitro effects of preserved and unpreserved antiglaucoma drugs on apoptotic marker expression by human trabecular cellsGraefes Arch Clin Exp Ophthalmol2003241121037104314605906
- YuALFuchshoferRKampikAWelge-LüssenUEffects of oxidative stress in trabecular meshwork cells are reduced by prostaglandin analoguesInvest Ophthalmol Vis Sci200849114872488018971427
- SamplesJRBinderPSNayakSThe effect of epinephrine and benzalkonium chloride on cultured corneal endothelial and trabecular meshwork cellsExp Eye Res19894911122759185
- SullivanDARochaEMAragonaPTFOS DEWS II Sex, Gender and Hormones ReportOcul Surf201715328433328736336
- SharmaAHindmanHBAging: a predisposition to dry eyesJ Ophthalmol2014201478168325197560
- SchaumbergDANicholsJJPapasEBTongLUchinoMNicholsKKThe international workshop on meibomian gland dysfunction: report of the subcommittee on the epidemiology of, and associated risk factors for, MGDInvest Ophthalmol Vis Sci20115241994200521450917
- QuigleyHANumber of people with glaucoma worldwideBr J Ophthalmol19968053893938695555
- RossiGCPasinettiGMScudellerLRaimondiMLanteriSBianchiPERisk factors to develop ocular surface disease in treated glaucoma or ocular hypertension patientsEur J Ophthalmol201323329630223335308
- GhoshSO’HareFLamoureuxEVajpayeeRBCrowstonJGPrevalence of signs and symptoms of ocular surface disease in individuals treated and not treated with glaucoma medicationClin Experiment Ophthalmol201240767568122394358
- MossSEKleinRKleinBEPrevalence of and risk factors for dry eye syndromeArch Ophthalmol200011891264126810980773
- MossSEKleinRKleinBEIncidence of dry eye in an older populationArch Ophthalmol2004122336937315006852
- EzuddinNSAlawaKAGalorATherapeutic strategies to treat dry eye in an aging populationDrugs Aging201532750551326123947
- FoulksGNPharmacological management of dry eye in the elderly patientDrugs Aging200825210511818257598
- DingJSullivanDAAging and dry eye diseaseExp Gerontol201247748349022569356
- JohnsonATDrackAVKwitekAECannonRLStoneEMAlwardWLClinical features and linkage analysis of a family with autosomal dominant juvenile glaucomaOphthalmology199310045245298479711
- HuangWPediatric glaucoma: a review of the basics2014 Available from: https://www.reviewofophthalmology.com/article/pediatric-glaucoma-a-review-of-the-basicsAccessed August 16, 2016
- PaschidesCAStefaniotouMPapageorgiouJSkourtisPPsilasKOcular surface and environmental changesActa Ophthalmol Scand199876174779541438
- WolkoffP“Healthy” eye in office-like environmentsEnviron Int20083481204121418499257
- WolkoffPOcular discomfort by environmental and personal risk factors altering the precorneal tear filmToxicol Lett2010199320321220833234
- WolkoffPNojgaardJKFranckCSkovPThe modern office environment desiccates the eyes?Indoor Air200616425826516842606
- BlehmCVishnuSKhattakAMitraSYeeRWComputer vision syndrome: a reviewSurv Ophthalmol200550325326215850814
- RosenfieldMComputer vision syndrome: a review of ocular causes and potential treatmentsOphthalmic Physiol Opt201131550251521480937
- PimenidiMKPoluninGSSafonovaTNMeibomian gland disfunction in computer vision syndromeVestn Oftalmol201012664952 Russian
- FengaCAragonaPCacciolaAMeibomian gland dysfunction and ocular discomfort in video display terminal workersEye (Lond)2008221919517962818
- MessmerEMThe pathophysiology, diagnosis, and treatment of dry eye diseaseDtsch Arztebl Int201511257181 quiz 225686388
- BoimerCBirtCMPreservative exposure and surgical outcomes in glaucoma patients: the PESO studyJ Glaucoma201322973073523524856
- ThiemeHvan der VeldenKKKonservierungsmittel aus Sicht der Glaukomchirurgie. [Preservatives from the perspective of glaucoma surgery]Ophthalmologe20121091110731076 German23179811
- BaudouinCPisellaPJFillacierKOcular surface inflammatory changes induced by topical antiglaucoma drugs: human and animal studiesOphthalmology1999106355656310080214
- BaudouinCMechanisms of failure in glaucoma filtering surgery: a consequence of antiglaucomatous drugs?Int J Clin Pharmacol Res199616129419001927
- BaudouinCSide effects of antiglaucomatous drugs on the ocular surfaceCurr Opin Ophthalmol1996728086
- TanLLMorganPCaiZQStraughanRAPrevalence of and risk factors for symptomatic dry eye disease in SingaporeClin Exp Optom2015981455325269444
- PaulsenAJCruickshanksKJFischerMEDry eye in the beaver dam offspring study: prevalence, risk factors, and health-related quality of lifeAm J Ophthalmol2014157479980624388838
- VersuraPCamposECMenopause and dry eye. A possible relationshipGynecol Endocrinol200520528929816019376
- JinXLinZLiuYLinLZhuBHormone replacement therapy benefits meibomian gland dysfunction in perimenopausal womenMedicine (Baltimore)20169531e426827495030
- AffinitoPDi Spiezio SardoADi CarloCEffects of hormone replacement therapy on ocular function in postmenopauseMenopause200310548248714501611
- FengYFengGPengSLiHThe effect of hormone replacement therapy on dry eye syndrome evaluated with Schirmer test and break-up timeJ Ophthalmol2015201542030226664737
- GuaschinoSGrimaldiESartoreAVisual function in menopause: the role of hormone replacement therapyMenopause2003101535712544677
- PelitABagisTKayaselcukFDursunDAkovaYAydinPTear function tests and conjunctival impression cytology before and after hormone replacement therapy in postmenopausal womenEur J Ophthalmol200313433734212872789
- GomesJAPAzarDTBaudouinCTFOS DEWS II Iatrogenic ReportOcul Surf201715351153828736341
- MajumdarSHippalgaonkarKRepkaMAEffect of chitosan, benzalkonium chloride and ethylenediaminetetraacetic acid on permeation of acyclovir across isolated rabbit corneaInt J Pharm20083481–217517817897799