Abstract
Purpose:
To compare visual performance in eyes with intraocular lenses (IOLs) that filter short-wave blue light versus contralateral eyes with IOLs that do not filter visible blue light.
Methods:
In this prospective, assessor-masked study that was conducted at five clinics in the US, eligible candidates were at least 12 months postimplantation of a control IOL and a contralateral IOL that filtered blue light. Glare disability was defined as the intensity of a white-light annulus that obscured a subject’s ability to see a central target. Heterochromatic contrast thresholds were defined as the intensity of a blue-light disk that obscured a central target. Photostress recovery time was the duration required to regain sight of the target after a five-second flash of annulus light.
Results:
Fifty-two subjects were evaluated. Mean glare disability was significantly less (P = 0.04) in the blue-filtering IOL group (1.97 ± 0.44 log μW/cm2) than in the control group (1.88 ± 0.43 log μW/cm2). Mean heterochromatic contrast threshold was significantly higher (P = 0.0003) in the blue-filtering IOL group (0.36 ± 0.43 log μW/cm2) than in the control IOL group (0.15 ± 0.49 log μW/cm2). Geometric mean photostress recovery time was significantly faster (P = 0.02) in the blue-filtering IOL group (21 ± 3 seconds) than in the control IOL group (26 ± 3 seconds).
Conclusions:
Glare disability was significantly lower, heterochromatic contrast threshold was significantly better, and recovery from photostress was significantly faster in the eyes with blue-filtering IOLs than in the contralateral control eyes with IOLs that did not filter blue light.
Introduction
The idea that intraocular blue-light filters could improve visual function has been posited for many decades. In 1933, Walls and Judd noted the preponderance of intraocular blue-light filters across many species of vertebrates and noted that “scattered light, in nature, is largely of short wave-lengths; if sufficiently bright a true glare results”.Citation1,Citation2 Therefore, they believed that intraocular blue-light filters could improve visual function by reducing glare discomfort and ‘dazzle’ and by enhancing contrast.Citation1,Citation2 Glare refers generally to a condition where individuals are exposed to a light source, either direct or indirect, that is in excess of their adaptive state. Such light can cause both discomfort and disability (a reduction in visual performance). As originally noted by Walls and Judd,Citation1,Citation2 light in the short-wave region of the visible spectrum, blue light, has proven to be particularly deleterious for inducing discomfortCitation3 and masking visual targets.Citation4
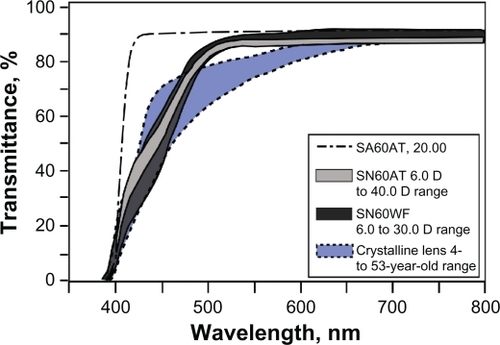
Another way that blue-light filters might improve visual performance is by enhancing contrast, an idea that was originally reviewed by Luckiesh in 1915.Citation5 In 1972, Luria demonstrated this effect by showing that the threshold for a yellow increment flash on a blue background was reduced when viewed through a blue-absorbing filter.Citation6 More recently, Wolffsohn et al confirmed this effect using contrast measures.Citation7 The degree of contrast enhancement varied among studies of filters with different spectral characteristics.Citation8–Citation11 For optimum enhancement, some research supported blocking wavelengths shorter than 450 nm but not longer than 480 nm.Citation12,Citation13 This recommended absorbance profile is similar to the natural crystalline lens,Citation14 as shown in . The contrast-enhancing effects that were measured with blue-filtering lenses arose because the filters reduced the luminance of the background relative to the target, which increased contrast and therefore increased the detectability of the central target. These simple laboratory situations are a good description of many visual situations outdoors. The preponderance of Rayleigh scattered light (seen as ‘blue haze’ and blue sky light) creates a natural situation where many targets are viewed on short-wave (blue) backgrounds.Citation15
Figure 1 Transmission spectra of the natural crystalline lens and of the intraocular lens models under investigation. Copyright © 2010, Association for Research in Vision and Ophthalmology. Reproduced with permission from Boettner and Wolter. Transmission of the ocular media. Invest Ophthalmol Vis Sci. 1962;1(6):776–783.Citation14 Spectra are redrawn from package inserts of intraocular lenses with permission from Alcon Laboratories, Inc.
As with extraocular filters and native intraocular filters, blue-filtering intraocular lenses (IOLs) that have an absorbance profile similar to the crystalline lens have also demonstrated enhancement of some aspects of visual performance.Citation16 The blue-light filtering properties of these IOLs were originally designed to be similar to healthy crystalline lenses (see ), in order to protect the retina from photodamage.Citation17 In addition, these blue-filtering IOLs also reduced glare disability and improved photostress recovery (relative to a lens that filters only ultraviolet light).Citation16 The present study replicates our earlier study of subjects with blue-light filtering IOLs versus subjects with control IOLs,Citation16 with some important modifications. First, we have added an assessment of heterochromatic contrast threshold (longer-wave target against a shorter-wave blue background). Also, rather than using a between-subject design (ie, comparing subjects with blue-filtering IOLs with subjects with IOLs that did not filter visible light), the present study used a within-subject (contralateral) design. All subjects had an implant that filtered both ultraviolet and blue light in one eye and had an ultraviolet-only filtering implant in the other eye, so that all subjects served as their own controls. These more thorough and rigorously controlled experiments were designed to measure the glare disability, photostress recovery, and heterochromatic contrast thresholds more conclusively in eyes with blue-light filtering IOLs versus eyes with control IOLs.
Subjects and methods
In this cross-sectional, prospective, multicenter study, participating clinicians reviewed their charts to identify eligible candidates who were at least 12 months postimplantation of the appropriate contralateral IOLs. All subjects were required to have a monofocal IOL that filtered only ultraviolet light (AcrySof IOL model SA60AT; Alcon Laboratories, Inc, Fort Worth, TX, USA) in one eye. In the contralateral eye, subjects were required to have a monofocal IOL with a chromophore that filtered both ultraviolet light and short-wave blue light (AcrySof Natural IOL, model SN60AT; Alcon) or (AcrySof IQ Aspheric Natural IOL, model SN60WF; Alcon). shows the transmission spectra of the SA60AT, SN60AT, and SN60WF IOLs, as provided in the package inserts (AcrySof IQ Aspheric Natural IOL Product Information, 2005, and AcrySof Natural Single-Piece IOL Product Information, 2007; Alcon).
Subjects were required to be at least 21 years of age, in good ocular health, and able to perform the testing competently. Subjects who agreed to visit an investigative clinic were screened for a defined list of ocular health inclusion criteria, including the following: corneal health (no dystrophy, irregular astigmatism, or prior corneal surgery), retinal health (no macular degeneration, previous detachment, or diabetic retinopathy), optic nerve health (no atrophy), iris health (no clinical miosis), and overall ocular health (no ocular disease and/or condition that could compromise study results). Slit-lamp examinations were used to confirm the presence of clear ocular media and the absence of clinically significant posterior capsule opacification. Subjects were excluded from participation if they had any conditions that could be exacerbated, triggered, or worsened by exposure to high-intensity light. Baseline measures included manifest refraction and uncorrected and corrected distance visual acuity.
This study was approved by the Sterling Institutional Review Board (Atlanta, GA, USA) for all participating clinical sites. The experimental procedures adhered to the tenets of the Declaration of Helsinki. Subjects were informed about the aims and methods of the study, and all subjects signed a statement of informed consent.
Apparatus
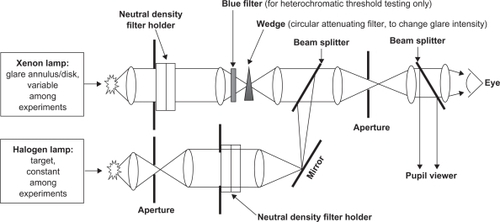
A two-channel Maxwellian-view optical system, which was similar to previously described systems,Citation4,Citation18–Citation20 was constructed at each clinic, disassembled after use, and reassembled at the next clinic. shows a schematic of the system. The glare source (annulus/disk) and the visual target were produced by a dual-port xenon-arc and halogen lamp as the light source (Jintan Jinyang Medical Instruments, China). Alignment of the subject’s eye with the optical system was maintained with forehead rests and a dental impression bite bar that was custom-fit for each subject. An auxiliary optical channel with magnifying lenses was used to monitor the pupil during testing to ensure proper fixation and sustained alignment. The same apparatus, with small variations, was used to test glare disability, contrast threshold, and photostress recovery.
Figure 2 Schematic of the systems used for our dependent measures. The lenses were ultraviolet-coated, planoconvex achromats.
All photometric calibrations were performed using a PR-650 SpectraScan Colorimeter (Photo Research, Inc, Chatsworth, CA). Wedge and neutral density radiometric calibrations were performed by using a Graseby Optronics United Detection Technology (UDT) instrument (Orlando, FL). The same UDT instrument was used before every experimental session and at every clinical site to ensure that the total light output of the optical system remained constant and consistent at all clinical sites.
Visual target
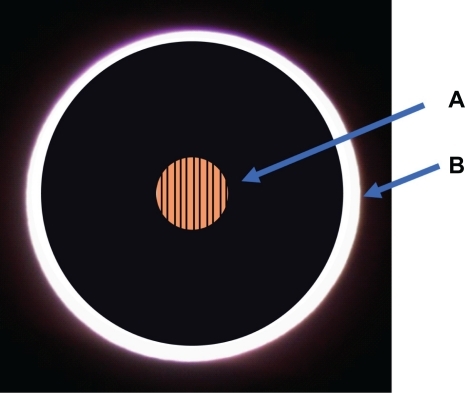
The visual target was the same in all tests (glare disability, photostress recovery, and heterochromatic contrast threshold). The target was produced by the 100 W halogen bulb of the dual-port source. The halogen bulb had an emission spectrum as shown in (as assessed by the SpectraScan colorimeter). The emission spectrum had a peak radiance at 645 nm and a chromaticity of u′ = 0.21 and v′ = 0.50 on the color space definition, which was established by the International Commission on Illumination (Commission Internationale de l′Éclairage, CIE).Citation21 The output in the halogen channel was maintained at constant energy and was checked by a dedicated radiometer at the beginning and end of each clinic visit. The visual target that was produced in the halogen channel was composed of a 3.1° diameter disk that contained a sine-wave grating with a spatial frequency of eight cycles/degree (produced by a sine-wave on clear glass; Rolyn Optics, Covina, CA, USA). The halogen channel was shuttered during testing so that the target was off for one second and exposed for one second, in order to avoid adaptation effects and to make the task less difficult. A schematic depicting a subject’s view of the visual target is shown in .
Figure 3 Gray trace: unattenuated emission spectrum of the halogen bulb that was used to create the target visual stimulus. Blue trace: unattenuated emission spectrum of the light in the xenon channel that was used to create the broad-band glare annulus and photostress condition.
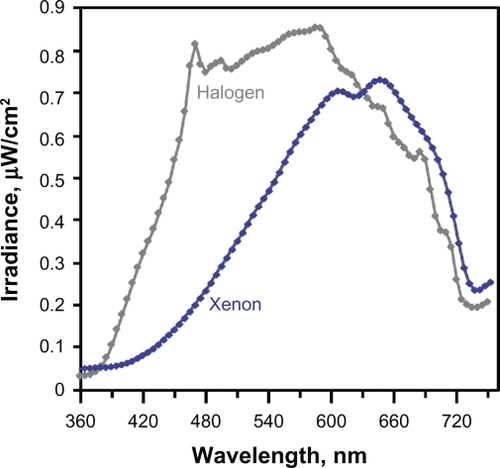
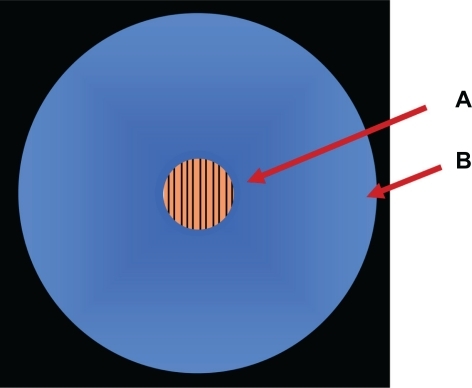
Figure 4 Schematic depicting a subject’s view into the testing apparatus for the glare disability experiment. A) Visual target. B) Glare annulus.
Glare light source
The characteristics of the glare light varied somewhat among the three tests (glare disability, photostress recovery, and heterochromatic contrast threshold). For all tests, the glare light originated from the 250 W xenon bulb of the dual-port source. The xenon source was modified to allow point-source illumination and was manipulated to produce either an annulus or a background field, depending on the test. The xenon source had an emission spectrum, as shown in (as assessed by the SpectraScan colorimeter). This xenon glare source appeared as a broad-band white light, with a CIE chromaticity of u′ = 0.25, v′ = 0.53.
Visual testing
The procedure for each assessment was explained to the subjects prior to testing using a standardized set of animated slides. Prior to each type of test, each subject was instructed to fixate on the center of the target stimulus, and the investigator aligned the optical system so that the arc image (2.5 mm diameter) was in focus in the plane of the subject’s pupil. The investigator was masked to the identities of the IOLs during testing.
Disability glare testing
During disability glare testing, the xenon-channel spectrum was unfiltered and was set to produce an annulus with a 20° inner diameter and 22° outer diameter, as shown in . The subject first viewed the target surrounded by an annulus that had an intensity set at a level that was much too low to obscure the target stimulus. The technician then increased the intensity of the annulus via a neutral-density wedge until the subject stated that the target stimulus was no longer visible. The intensity of the annulus of light at that point was defined as the glare disability value. An ascending method of limits combined with the method of constant stimuli procedure was used. Five measures were taken per eye, unless a subject’s values had more than 5% variability, in which case up to four additional trials were conducted. If extra trials were conducted, all trials were averaged into the subject’s mean result.
Heterochromatic contrast threshold testing
During heterochromatic threshold testing, the xenon source was filtered with an interference filter (half-power bandwidth = 8 nm, Edmund Optics, Barrington, NJ, USA) in order to produce a monochromatic 430 nm field. The diameter of the background encompassed a 24° visual angle, as shown in . At the beginning of each test, the intensity of the blue background was set at a level that was much too low to obscure the target stimulus. The technician then increased the intensity of the background until the subject stated that the target stimulus was no longer visible. An ascending method of limits was used. Once an approximate threshold had been determined, the method of constant stimuli was used to determine a precise threshold. Five trials were sufficient to derive accurate thresholds, but if a subject’s values were excessively variable (ie, more than 5% variability), up to four additional trials were conducted. If extra trials were conducted, all trials were averaged into the subject’s mean result.
Figure 5 Schematic depicting a subject’s view into the testing apparatus for the heterochromatic threshold testing experiment. A) Visual target. B) Background field.
Photostress recovery testing
For the photostress recovery experiment, a 24° diameter disk with an intensity of 5.0 log trolands served as the photostress stimulus. A shutter from Vincent Associates (Rochester, NY, USA) was used to present the photostress stimulus. The target stimulus alone (without photostress) was presented for the subject to view for 20 seconds. Subjects were instructed to keep their eye open during the upcoming photostress exposure. The subject was then presented with the photostress for five seconds. If the investigator observed that the test beam was occluded by blinking or eye closure, the test was discarded. After the photostressor was discontinued, a stopwatch was started. Subjects were instructed to indicate when they could first perceive the target stimulus, and this duration was defined as the photostress recovery time. After early experiments showed that these measures were not reproducible for each subject (due to the inability of the retina to recover fully within a convenient amount of time), these measures were taken only once per eye, to ensure that measurements were taken from a naïve retina.
Statistical analyses
Comparisons for glare disability assessment, heterochromatic contrast threshold, and photostress recovery between IOL groups were performed using paired t-tests, at a level of significance of alpha = 0.05. The data were averaged, including those with the additional trials, and standard deviation values were calculated. The mean values for glare disability and heterochromatic contrast threshold were compared, and the data are presented as log energy values (μW/cm2). For photostress, the analyses were performed on the logarithms, and the means and standard deviations of the log-scale values were then converted using antilogs, so as to convert these summary values to the original scale of measurement. For photostress recovery, the data are presented in seconds. All results are reported as mean ± standard deviation unless otherwise specified.
Results
Demographics
A total of 52 subjects were enrolled, of whom 28 were women (54%) and 24 were men (46%). The study population had a mean age of 76 ± 9 years. All subjects had a control SA60AT lens in one eye. In the contralateral eyes, 50% of subjects (26 of 52) had a model SN60AT lens (spherical IOL with the blue-filtering chromophore), and 50% of subjects (26 of 52) had a model SN60WF lens (aspheric IOL with the blue-filtering chromophore). The average duration of pseudophakia before entering the study was 5.2 ± 1.3 years for the eyes with blue-filtering IOLs, and 5.6 ± 1.3 years for the eyes with control SA60AT IOLs. The average duration between contralateral IOL implantations was 0.4 ± 1.1 years. Uncorrected and corrected distance visual acuities were similar in eyes with blue-filtering IOLs and eyes with control SA60AT IOLs, as shown in .
Table 1 Monocular distance visual acuities among groups, by model of intraocular lens
Glare disability
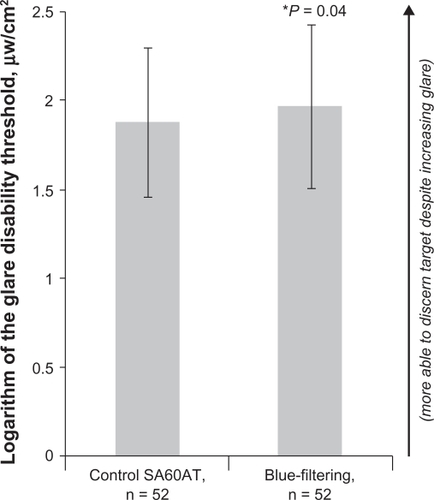
Significantly more light (P = 0.04) could be withstood by eyes with blue-filtering IOLs (1.97 ± 0.44 log μW/cm2) than by eyes with nonfiltering control IOLs (1.88 ± 0.43 log μW/cm2) before losing sight of the target, as shown in . Due to variability in repeat measurements, which may have been caused by difficulty in aligning the subject with the optical axis of the system, five eyes with blue-filtering IOLs and five eyes with control IOLs required more than five tests per eye (up to nine trials per eye).
Figure 6 Glare disability (the amount of energy in an annulus necessary to veil a central target). Values are presented as mean ± standard deviation.
Heterochromatic contrast threshold
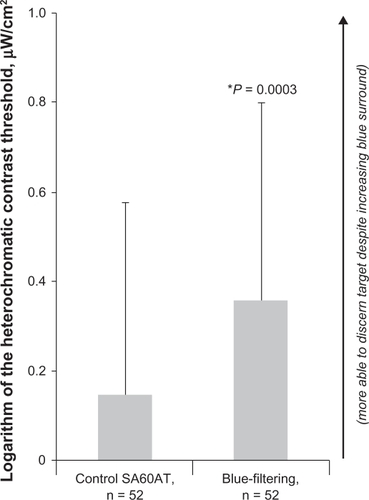
The mean heterochromatic contrast threshold was significantly better (P = 0.0003) in the blue-filtering IOL group (0.36 ± 0.43 log μW/cm2) than in the control SA60AT IOL group (0.15 ± 0.49 log μW/cm2), as shown in . Due to variability in repeat measurements, which may have been caused by difficulty in aligning the subject with the optical system, eight eyes with blue-filtering IOLs and five eyes with control IOLs required more than five tests per eye (up to nine trials per eye).
Figure 7 Heterochromatic contrast threshold (the amount of energy in the 430 nm background that forced the subject to lose sight of the central target). Values are presented as mean ± standard deviation, with error bars shown unidirectional for clarity.
Photostress recovery
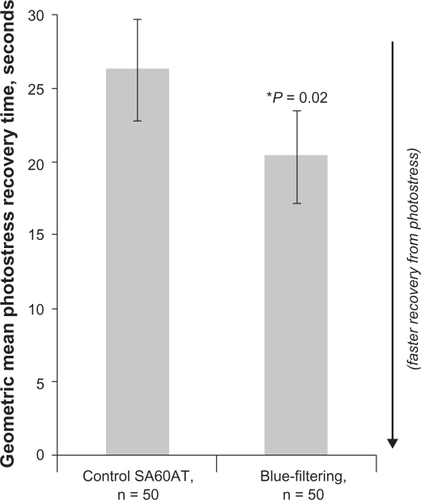
The geometric mean transformed photostress recovery time was significantly faster (P = 0.02) in the group with the blue-filtering IOLs (21 ± 3 seconds) than in the group with the nonfiltering IOLs (26 ± 3 seconds), as shown in . A similar result was obtained (P = 0.023, for a one-tailed test) when analyzing the raw data using a Student’s t-test (with corrections for unequal variance). Photostress recovery times were analyzed for 100 eyes (50 blue-filtering IOLs and 50 nonfiltering IOLs) of the total cohort of 104 eyes. Data were missing for four eyes due to head movement or blinking during the test. For one additional eye in the blue-filtering IOL group, no photostress recovery time was recorded because the time during which photostress recovery should be recorded had exceeded six minutes without the subject reporting the ability to discern the target. It was suspected that this subject may have had covert retinal pathology that could have affected photostress recovery. Photostress recovery times of up to 407.4 seconds had been observed for the other eyes, so the decision was made to impute the value of 410 seconds into the unrecorded parameter, in order to preserve the information that the photostress recovery time for this eye was long.
Figure 8 Photostress recovery durations (amount of time required to regain sight of the central target after exposure to photostress). Values are presented as geometric mean ± standard deviation.
Discussion
The results of the present study are consistent with the conclusion that the filtering of blue light provided by the AcrySof Natural IOLs has distinct effects on visual performance.
Glare disability was statistically different between the group with blue-filtering IOLs and the group with nonfiltering IOLs. The intense light entering the eye from the glare source was scattered forward by the intraocular media, causing a veiling luminance over the visual target. Analogous situations could occur in the real world when a driver is looking into oncoming headlights. By filtering such light, the visibility of a target within an individual’s sight line would be improved, as was demonstrated by the model in this study. This improvement would be directly related to the amount of energy absorbed. As shown in , our glare source contained some energy in the 400–450 nm region, where absorbance by the blue-filtering IOLs is higher than absorbance by the nonfiltering IOL (see ). The extent to which an intraocular filter absorbs the scattering source should determine the degree to which that filter will reduce glare disability. Consistent with this presumed mechanism, past studies that presented stimuli with relatively little short-wave energy to subjects with blue-filtering IOLs have reported minimal effects on glare disability.Citation22 Under more naturalistic conditions (eg, outdoors in the sunlight, which contains more short-wave energy), the effect of a blue-light filter on glare disability could be even more substantial.
Using the same xenon light source, we also found a large effect on photostress recovery. On average, visual function was recovered five seconds faster by the eyes with the blue-filtering IOLs than by the eyes with the non-blue-filtering IOLs. The contralateral design of the study was optimal for studying this parameter, as many factors influence the regeneration kinetics of bleached photopigment, eg, age and disease state. Such a difference could be quite significant. For example, recovering visual function five seconds faster translates to 440 feet when driving at 60 miles per hour. This could mean the difference between having an accident or not when impaired by bright oncoming headlights. The fact that we found a stronger effect for photostress recovery compared with glare disability may be due to the intense light levels that were presented in the photostress condition. Even a small amount of short-wave energy is probably significant if the bleaching source is sufficiently intense.
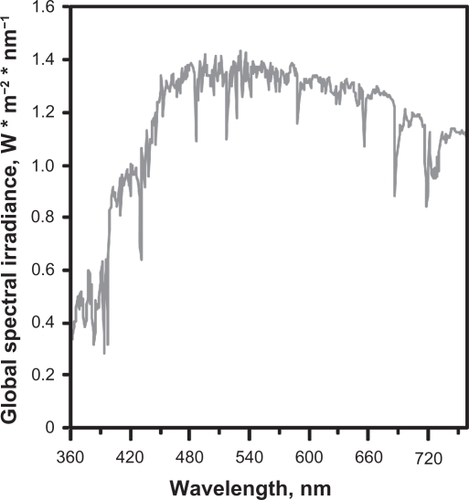
The spectrum of the xenon arc lamp that produced the glare and photostress conditions in this study was applicable as a model both for nighttime driving and for daytime function. Xenon headlights are available for many models of automobiles. Moreover, the spectrum of the xenon arc lamp (see ) is a good approximation of midday sunlightCitation23 (see ). Broad-band white light sources, such as the one used in this study, are thus common in everyday life.
Figure 9 Spectrum of daytime sunlight.
Copyright © 2010, ASTM international. Reproduced with permission from ASTM G173-03e1 Standard Tables for Reference Solar Spectral Irradiances: Direct Normal and Hemispherical on 37° Tilted Surface. A copy of the complete standards may be obtained from ASTM, www.astm.org.
In addition to the white-light experiments in this study, heterochromatic contrast thresholds were also significantly better in the blue-filtering IOL group than in the control IOL group when using a short-wave background and a mid-wave target. Given the neural mechanisms underlying edge detection, any alteration of an image that enhances contrast of a given target relative to its surrounding spectral environment should improve detectability of that target. Hence, under the right wavelength conditions, and if the eye acted as a simple detector, a blue-filtering IOL would improve contrast, by definition. The wavelength conditions are simply that the blue-filtering lens absorbs one side of a chromatic border more than the other side and hence enhances the difference across the edge. Our study has shown that a blue-filtering IOL enhanced contrast as directly as the simple optics of contrast would predict.
Increased heterochromatic contrast thresholds have practical ecologic significance. Recent data have shown that color borders (ie, isoluminant edges) are probably very common in the natural environment,Citation24 and therefore chromatic differences likely play a significant role in object detection in the real world. This is particularly true when viewing objects at a distance, because distance would tend to equalize differences in luminance that would have defined edges if they were closer. A blue-filtering lens would recreate a luminance edge when it absorbed one side of a chromatic border more than the other side. In this study we used a 430 nm background with a mid-long-wave target (halogen). Is this kind of stimulus generalizable? In an analysis of vision in the natural environment, Wooten and Hammond argued that such a simple stimulus was a good characterization of vision outdoors.Citation15 Rayleigh scatter and blue haze often create blue backgrounds when viewing objects at a distance, such as an airplane on a blue sky. The opposite effect occurs for objects directly within the sight path, ie, light scatters out of the sight line, causing a shift toward mid-long-wave light. Hence, we are often viewing longer-wave targets on short-wave backgrounds.
Vision with good heterochromatic contrast is also necessary indoors. Vision scientists have noted that black and white documents have been the subject of frequent indepth studies, but chromatic documents are now becoming an issue due to the large-scale appearance of web pages in color.Citation25 Experimenters who tested the readability of chromatic web pages with healthy phakic subjects noted that certain chromatic situations were counterproductive for good visual performance and produced a discomfort that was “similar to that produced by dazzling, a phenomenon when using an insufficiently shaded and incorrectly placed light source”.Citation25 It was already known that blue-filtering AcrySof IOLs do not adversely affect color vision.Citation26 Our study shows that, to the contrary, these IOLs increase heterochromatic contrast thresholds.
Given our study design, it is likely that the mechanism underlying our results was wholly due to the spectral properties of the blue-filtering IOL. However, the blue-light filtering could also have induced other changes that could further enhance the visual effects. For example, Nolan et al recently found that implantation of a blue-filtering IOL was associated with increases in another intraocular blue-light absorber, macular pigment, when compared with implantation of a nonfiltering IOL.Citation27 Macular pigments influence glare disability and photostress recovery timesCitation4,Citation20 and improve contrast enhancement (when targets are presented with a 460 nm background, a wavelength that matches the peak absorbance of macular pigments).Citation28 If macular pigment was denser in the eyes containing the blue-filtering IOLs, this could explain at least part of the visual effects we measured. Whatever the mechanisms of visual enhancement with blue-filtering IOLs, the benefits were significant for all outcomes measured in this study.
In conclusion, our results are consistent with the hypothesis that the blue-filtering AcrySof IOLs (with the specific absorption spectra conferred by the proprietary chromophore) reduced disability due to glare, improved the heterochromatic contrast threshold, and improved recovery from photostress, under the spectral conditions presented in these experiments.
Acknowledgements
The authors would like to acknowledge the following participating clinical investigators: Robert Lehmann MD (Lehmann Eye Center, Nacogdoches, TX, USA); James Davison MD (Wolfe Eye Clinic, Marshalltown, IA, USA); W Andrew Maxwell MD, PhD (Fogg, Maxwell, Lanier and Remington, Fresno, CA, USA); Stephen F. Brint MD (Brint Custom Vision, Metairie, LA, USA); and David A. Nethery MD (Nethery Eye Associates, Fort Worth, TX, USA), and Laura Fletcher MS (Vision Sciences Laboratory, University of Georgia, Athens, GA, USA) for assistance.
Disclosures
This study was supported by Alcon Research Ltd, Fort Worth, TX, USA. BRH and LMR have no financial or proprietary interest in any products in this manuscript. SS was an employee of Alcon during the conduct of the study. SFB is a consultant to Alcon.
References
- WallsGLJuddHDThe intra-ocular colour-filters of vertebratesBr J Ophthalmol1933171164167518169162
- WallsGLJuddHDThe intra-ocular colour-filters of vertebratesBr J Ophthalmol1933171270572518169167
- StringhamJMFuldKWenzelAJAction spectrum for photophobiaJ Opt Soc Am A Opt Image Sci Vis200320101852185814570098
- StringhamJMHammondBRJrThe glare hypothesis of macular pigment functionOptom Vis Sci200784985986417873771
- LuckieshMColor and visionColor and Its Applications2nd edNew York, NYD. van Nostrand Co1915
- LuriaSMVision with chromatic filtersAm J Optom Arch Am Acad Optom197249108188294564949
- WolffsohnJSCochraneALKhooHYoshimitsuYWuSContrast is enhanced by yellow lenses because of selective reduction of short-wavelength lightOptom Vis Sci2000772738110701805
- YapMThe effect of a yellow filter on contrast sensitivityOphthalmic Physiol Opt1984432272326472852
- LeatSJNorthRVBrysonHDo long wavelength pass filters improve low vision performance?Ophthalmic Physiol Opt19901032192242216468
- HovisJKLovasikJVCullenAPKotheACPhysical characteristics and perceptual effects of “blue-blocking” lensesOptom Vis Sci198966106826892587033
- LeguireLESuhSEffect of light filters on contrast sensitivity function in normal and retinal degeneration subjectsOphthalmic Physiol Opt19931321241288265145
- ZigmanSVision enhancement using a short wavelength light-absorbing filterOptom Vis Sci19906721001042336247
- ZigmanSLight filters to improve visionOptom Vis Sci19926943253281565435
- BoettnerEWolterJTransmission of the ocular mediaInvest Ophthalmol Vis Sci196216776783
- WootenBRHammondBRMacular pigment: Influences on visual acuity and visibilityProg Retin Eye Res200221222524012062535
- HammondBRBernsteinBDongJThe effect of the AcrySof natural lens on glare disability and photostressAm J Ophthalmol2009148227227619426959
- SparrowJRMillerASZhouJBlue light-absorbing intraocular lens and retinal pigment epithelium protection in vitroJ Cataract Refract Surg200430487387815093654
- HammondBRBernsteinBDongJThe effect of the AcrySof natural lens on glare disability and photostressAm J Ophthalmol2009148227227619426959
- RenziLHammondBThe effect of macular pigment on contrast thresholdsJ Vision2010In press.
- StringhamJMHammondBRMacular pigment and visual performance under glare conditionsOptom Vis Sci2008852828818296924
- PointerMA comparison of the CIE 1976 colour spacesColor Res Appl198162108118
- MuftuogluOKarelFDumanREffect of a yellow intraocular lens on scotopic vision, glare disability, and blue color perceptionJ Cataract Refract Surg200733465866617397740
- ASTM G173-03e1, Standard Tables for Reference Solar Spectral Irradiances: Direct Normal and Hemispherical on 37° Tilted SurfaceWest Conshohocken, PAAmerican Society for Testing and Materials, ASTM International2003
- HansenTGegenfurtnerKRIndependence of color and luminance edges in natural scenesVis Neurosci2009261354919152717
- PescioCde MattielloMAlvarezRReadability of chromatic documentsCaivanoJLAIC 2004 Color and Paints, Proceedings, Interim Meeting of the International Color AssociationPorto Alegro, BrazilInternational Color Association2005
- Rodríguez-GalieteroAMontés-MicóRMuñozGAlbarrán-DiegoCComparison of contrast sensitivity and color discrimination after clear and yellow intraocular lens implantationJ Cataract Refract Surg20053191736174016246777
- NolanJMO’ReillyPLoughmanJAugmentation of macular pigment following implantation of blue light-filtering intraocular lenses at the time of cataract surgeryInvest Ophthalmol Vis Sci200950104777478519628740
- RenziLMSnodderlyDMHammondBRJrReduction of surround suppression and enhancement of discriminability by macular pigmentInvest Ophthalmol Vis Sci20095051703