
Abstract
Purpose
To investigate the biomechanical response of the cornea, lamina cribrosa (LC), and prelaminar tissue (PT) to an acute intraocular pressure (IOP) increase in patients with markedly asymmetrical glaucoma and in healthy controls.
Patients and methods
A total of 24 eyes of 12 patients with markedly asymmetrical primary open-angle glaucoma (POAG) and 12 eyes of 12 healthy patients were examined with spectral-domain optical coherence tomography (SD-OCT) and ocular response analyzer (ORA) at baseline and during acute IOP elevation by means of an ophthalmodynamometer. The displacement of the LC and PT and the change in corneal hysteresis (CH) and corneal resistance factor (CRF) were evaluated.
Results
Following a mean IOP increase of 12.3±2.4 mmHg, eyes with severe glaucoma demonstrated an overall mean anterior displacement of the LC (−6.58±26.09 µm) as opposed to the posterior laminar displacement in eyes with mild glaucoma (29.08±19.28 µm) and in healthy eyes (30.3±10.9; p≤0.001 and p=0.001, respectively). The PT displaced posteriorly during IOP elevation in all eyes. The CH decreased in eyes with severe glaucoma during IOP elevation (from 9.30±3.65 to 6.92±3.04 mmHg; p=0.012), whereas the CRF increased markedly in eyes with mild glaucoma (from 8.61±2.30 to 12.38±3.64; p=0.002) and in eyes with severe glaucoma (from 9.02±1.48 to 15.20±2.06; p=0.002). The increase in CRF correlated with the anterior displacement of the LC in eyes with severe glaucoma.
Conclusion
Eyes with severe glaucoma exhibited a mean overall anterior displacement of the anterior laminar surface, while eyes with mild glaucoma and healthy eyes showed a posterior displacement of the LC during IOP elevation. The CH decreased significantly from baseline only in eyes with severe glaucoma, but the CRF increased significantly in all glaucomatous eyes. The CRF increase correlated with the anterior displacement of the LC in eyes with severe glaucoma.
Introduction
Increased intraocular pressure (IOP) is a well-known risk factor for the onset and progression of glaucomatous optic neuropathy (GON).Citation1–Citation3 It is widely accepted that an increase in IOP may lead to strain at the level of the lamina cribrosa (LC) and to a subsequent variable degree of deformation of the laminar tissue. This, in turn, may result in both mechanical and metabolic damage to the optic nerve fibers exiting the intraocular space via the laminar pores.Citation4–Citation6
The biomechanical properties of the LC have been thoroughly investigated,Citation7–Citation14 with a particular focus on the effect of raised IOP on the deformation of the LC. Studies conducted in this respect have employed ex vivo models,Citation15,Citation16 histomorphometric analysis of the LC in animal models,Citation17 and mathematical models based on human eyes.Citation18–Citation20
In recent years, the increased availability of high-resolution imaging devices, such as spectral-domain optical coherence tomography (SD-OCT), allowed in vivo analysis of the LC and prelaminar tissue (PT) in static and dynamic conditions, such as in human eyes with decreased IOP following filtering surgeryCitation21 or during an acute increase in IOP.Citation22–Citation24
Central corneal thickness (CCT) is also thought to be involved in glaucoma onset and progression, yet its role as an independent risk factor is still a matter of debate, as it could be just a surrogate for IOP. Nonetheless, other corneal features may prove useful to obtain more information on the overall biomechanical quality of the eye. The corneal properties might be linked to those of the LC and, therefore, provide insight into the individual response to mechanical stress at the level of the LC.Citation25–Citation30 More specifically, corneal features might be a surrogate for extracellular matrix (ECM) quality. In support of this hypothesis, it has been shown that 2 corneal biomechanical parameters, namely, corneal hysteresis (CH) and corneal resistance factor (CRF), are both reduced in Marfan syndrome, which is characterized by a systemic alteration of the ECM.Citation31 Given that ECM components of the cornea, peripapillary scleral ring, and LC are coded by the same gene, it is plausible that they also share a similar biomechanical behavior.Citation32
It is well known that primary open-angle glaucoma (POAG), the most common form of glaucoma worldwide, is often a bilateral disease. However, there are a considerable number of cases where the stage of the GON is markedly asymmetrical or even altogether unilateral. This disparity might reflect the presence of asymmetrical biomechanical properties in the contralateral fellow eye.
The aim of this study was to investigate the behavior of LC and PT following an induced increase in IOP via SD-OCT with enhanced depth imaging (EDI) in patients with markedly asymmetrical glaucoma damage and in control subjects. A protocol similar to the one previously described by Agoumi et alCitation24 was implemented.
Two corneal biomechanical properties (CH and CRF) were also assessed at baseline and during IOP elevation in all the patients enrolled.
Patients and methods
The current study was approved by the local ethics committee of the University of Bologna and adhered to the tenets of the Declaration of Helsinki. Written informed consent was obtained from all participants before any procedure. Mauro Cellini, MD, received from the person in the informed written consent to have the image published.
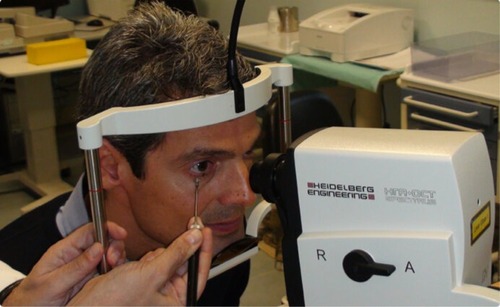
Figure 1 Application of the ophthalmodynamometer on the infratemporal eyelid during an SD-OCT examination.
A total of 12 consecutive patients attending the Glaucoma Unit of the Sant’Orsola-Malpighi Hospital (Bologna, Italy) with a diagnosis of POAG and a marked asymmetry in the GON stage between fellow eyes were recruited in the study. A total of 12 control subjects were enrolled among patients attending the eye clinic of the same hospital for a routine review without any specific ocular condition.
Inclusion criteria for glaucoma patients were the following: clinical diagnosis of glaucoma based on visual field (VF) testing, optic disc and retinal nerve fiber layer (RNFL) clinical appearance, open angle at gonioscopy, asymmetrical VF damage with 1 eye presenting a mean deviation (MD) greater than or equal to -6 dB and the fellow eye presenting an MD less than or equal to -12 dB, a satisfactory IOP control (≤21 mmHg) on medications, and a history of IOP >21 mmHg prior to commencement of treatment.
Exclusion criteria for glaucoma patients were the following: threat to fixation, past ocular history of any laser or surgical procedure, non-glaucomatous optic neuropathies, suboptimal IOP control on current medications (IOP >21 mmHg) and/or recent evidence of disease progression, poor fixation due to ocular (eg, low vision and nystagmus) or cognitive conditions (eg, dementia, poor cooperation), or age <18 years. Patients with a connective tissue disease (such as Marfan syndrome) or diabetes mellitus were also excluded from the study.
Inclusion criteria for control subjects were unremarkable ocular condition with a healthy optic disc and RNFL appearance, IOP within 21 mmHg, and normal VF. Exclusion criteria for normal subjects were past ocular history of any laser or surgical procedure, poor fixation, age <18 years, connective tissue diseases, or diabetes mellitus.
All the patients underwent a complete eye examination, including visual acuity assessment, Goldmann applanation tonometry (GAT), gonioscopy, and anterior and posterior segment biomicroscopy. At least 2 previous reliable VF tests (with fixation losses, false positives, and false negatives ≤20%) were required for each glaucoma patient. One additional VF test was performed with the same perimeter and strategy (Humphrey 24-2 SITA Standard; Carl Zeiss Meditec, Dublin, CA, USA) in every partecipant to the study to collect MD and pattern standard deviation (PSD) data.
Based on the perimetric indices, glaucomatous fellow eyes were divided into 2 groups: mild glaucoma when the MD ranged from -2 to -6 dB or severe glaucoma when the MD was equal or lower than -12 dB. The control group had an MD greater than or equal to -2 dB.
Spectral-domain optimal coherence tomography
SD-OCT has greatly enhanced diagnostic capabilities in ophthalmology. The low-coherence interferometer integrated into the device allows the acquisition of in vivo detailed cross-sectional images of the ocular structures. The reference and the reflected beams are simultaneously recorded by a spectrometer to generate A-scans from Fourier-transform time-delay signals.
A Heidelberg Spectralis OCT (Heidelberg Engineering, Heidelberg, Germany) was employed in this study. During the scan, the EDI mode was turned on to obtain enhanced details of deep ocular tissues and, therefore, facilitate the subsequent analysis. A radial scanning pattern (12 high-resolution 15° spaced radial scans each averaged from 30 B-scans with 768 A-scans per B-scan) was centered on the optic nerve of each eye included in the study. Glaucoma patients had both eyes imaged, whereas a randomly selected eye was scanned in each control subject.
The eye tracker function available in the Spectralis OCT was capable of obtaining a baseline image for each eye and to repeat the scan at the same position during the application of an ophthalmodynamometer on the temporal side of the inferior eyelid. Images with insufficient details were discarded, and the scans were repeated to obtain a quality level appropriate for further analysis.
Ocular response analyzer (ORA)
Corneal biomechanics data were collected with the ORA (Reichert Ophthalmic Instruments Inc, Depew, NY, USA). The device, which is similar to a noncontact tonometer, detects the change of shape of the corneal surface, while an air jet is delivered by the instrument. During the examination, the cornea is first deflected inward by the air puff, and then it regains its prolate configuration when the air stimulus terminates. An integrated infrared beam allows the recording of the forces required to applanate the cornea during the inward and outward movements of the corneal surface. The data collected on the force-in and force-out applanations are then used to calculate 2 biomechanical parameters, CH and CRF. The CH value provides a better characterization of the corneal contribution to IOP measurement than CCT alone. The CRF is a measure of corneal resistance, which is relatively independent of IOP.Citation33
An ORA examination was performed at baseline and during IOP elevation by means of an ophthalmodynamometer applied to the temporal side of the lower eyelid. Four measurements were collected for each eye, and the one with the highest quality score was selected for analysis.
Each patient underwent the ORA examination following the SD-OCT scan, with an interval of at least 1 hour between the 2 examinations. This was considered a sufficient time to allow each eye to recover from the previous ophthalmodynamometer compression.
IOP elevation
An ophthalmodynamometer (Inami, Tokyo, Japan) was used to increase the IOP during the SD-OCT and ORA examinations. The procedure was similar to the one employed by Agoumi et al.Citation24
The device was applied at the temporal side of the lower eyelid and pressure was exerted to reach a reading of ~30 Pa (). An IOP check was performed with a Tono-Pen tonometer (Innova Medical Ophthalmics, Toronto, ON, Canada) at baseline and during the application of the ophthalmodynamometer. The device was held in place during collection of the second set of OCT scans and the second set of ORA measurements. Both the tests took ~<1 min each. No patient experienced pain during the application of the ophthalmodynamometer; only a sensation of pressure on the globe was reported. No patient experienced changes in the quality or comfort of vision after the pressure elevation.
SD-OCT scan processing and analysis
Among the 12 radial scans obtained during each examination, 2 corresponding sets of 4 images that provided the best anatomical details at baseline and during IOP elevation were selected for each eye.
The images were processed with open-source vector graphics software (Inkscape, http://www.inkscape.org). A reference line connecting both sides of the termination of the retinal pigment epithelium–Bruch’s membrane interface was drawn. A set of equidistant lines perpendicular to the reference line were traced to intersect the anterior edge of the PT, and the image was saved. Then the same lines were drawn further down to intersect the anterior edge of the LC, which is seen as a highly reflective tissue beneath the PT, and a second image was saved. The same process was repeated for all the set of images acquired at baseline and during IOP elevation (–).
Figure 2 Vertical distances from the line connecting the Bruch’s membrane ends to the anterior surface of the lamina cribrosa and the prelaminar tissue at baseline (A and C) and during IOP elevation (B and D) in an eye with mild glaucoma.
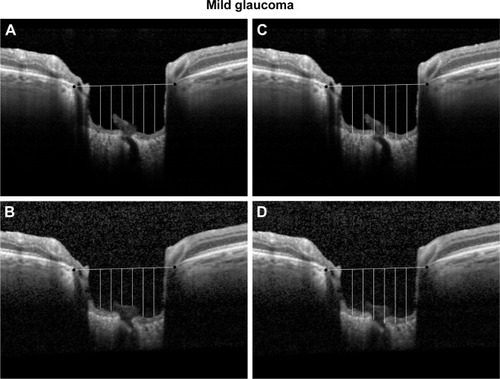
Figure 3 Vertical distances from the line connecting the Bruch’s membrane ends to the anterior surface of the lamina cribrosa and the prelaminar tissue at baseline (A and C) and during IOP elevation (B and D) in an eye with severe glaucoma.
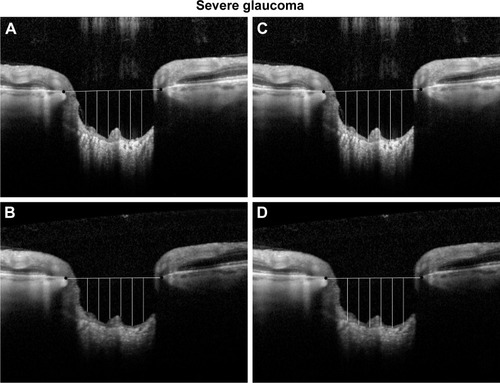
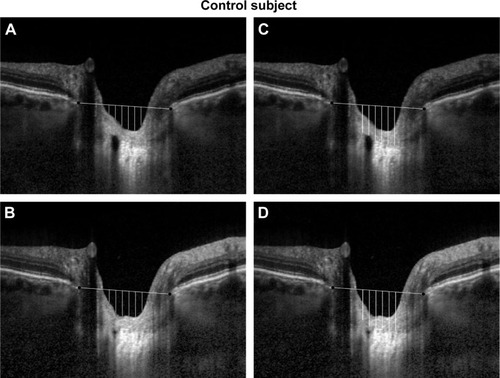
Figure 4 Vertical distances from the line connecting the Bruch’s membrane ends to the anterior surface of the lamina cribrosa and the prelaminar tissue at baseline (A and C) and during IOP elevation (B and D) in a control eye.
The vertical distances from the reference line to both the anterior limit of the PT and the LC were measured with ImageJ (National Institutes of Health, Bethesda, MD, USA), after calibrating the software with the scale bar included in each image.
The prelaminar and laminar tissue displacements were calculated as the mean difference between the corresponding vertical distances from the reference line in the baseline and elevated IOP conditions. Positive values were suggestive of an overall posterior movement of the tissues, whereas negative values were interpreted as an overall anterior displacement of the tissues examined. All the images were analyzed by the same trained examiner (CG) who was masked on the source of the images.
Statistical analysis
The Mann–Whitney U-test, Wilcoxon signed-rank test, and Friedman test were employed as appropriate for statistical analysis. Correlations were evaluated using Spearman correlation coefficients. The statistical analysis was performed with R (R software; provided in the public domain by the R Foundation for Statistical Computing, Vienna, Austria; available at www.r-project.org), and a p-value <0.05 was considered statistically significant.
Results
A total of 24 eyes of 12 patients with POAG and a significant degree of asymmetry in the stage of the disease between fellow eyes and 12 eyes of 12 healthy subjects were recruited for the study. The demographic data of the 3 groups are represented in .
Table 1 Demographic data of the participants to the study
Baseline ocular data (VF, CCT, IOP, CH and CRF) are shown in . As expected, at baseline there was a significant difference in the VF indices among the groups. Moreover the b-CRF (baseline CRF) was significantly lower in eyes with mild glaucoma (8.61±2.3 mmHg) and severe glaucoma (9.02±1.48 mmHg) compared with controls (p=0.039 and p=0.034, respectively).
Table 2 Values at baseline and comparison among groups
provides the details on IOP measured with GAT, Tonopen, and ORA.
Table 3 Baseline IOP with GAT, Tonopen, and ORA
The increase in IOP and the forces exerted following the application of the ophthalmodynamometer during both the OCT scans and the ORA measurements were not statistically different among the 3 groups (). The ophthalmodynamometer-induced CH (i-CH) was significantly lower in eyes with mild glaucoma (7.23±2.29 mmHg; p=0.011) and in eyes with severe glaucoma (6.92±3.04 mmHg; p=0.003) compared to controls (10.59±1.78 mmHg; ). The i-CH was also significantly lower than baseline CH (b-CH) in eyes with severe glaucoma (6.92±3.04 vs 9.30±3.65 mmHg; p=0.012), whereas no significant changes were detected in the other groups ().
Table 4 IOP during ophthalmodynamometer application and forces applied
Table 5 Values during IOP elevation and comparison among groups
Table 6 Intragroup comparison between values at baseline and during IOP increase
The ophthalmodynamometer-induced CRF (i-CRF) was significantly higher in eyes with severe glaucoma (15.2±2.06 mmHg) than in eyes with mild glaucoma and in controls (12.38±3.65 and 11.27±1.46 mmHg; p=0.027 and p=0.019, respectively). The i-CRF was also significantly higher than the b-CRF in both eyes with mild and severe glaucoma (12.38±3.64 vs 8.61±2.30 mmHg and 15.20±2.06 vs 9.02±1.48 mmHg; p=0.002 and p=0.002, respectively), whereas no significant change was observed in the control group (11.27±1.46 vs 10.64±1.28, p=0.275).
In terms of the anterior laminar surface response to the ophthalmodynamometer compression, we found that the laminar displacement (LD) was not statistically different between eyes with mild glaucoma and control eyes (29.08±19.28 and 30.3±10.9 µm, respectively; p=0.833). On the other hand, eyes with severe glaucoma exhibited an overall mean anterior displacement of the LC (−6.58±26.09 µm), which was significant when compared with both the control and mild glaucoma groups (p=0.001 and p<0.001, respectively).
It was also observed that the PT displacement (PTD) was reduced in eyes with severe glaucoma (13.08±17.06 µm) when compared with the control group (36.0±17.9 µm; p=0.001). On the other hand, the PTD in eyes with mild glaucoma (22.33±33.14 µm) was not significantly different to the PTD in eyes with severe glaucoma and in controls (p=0.518 and p=0.131, respectively). The data are summarized in .
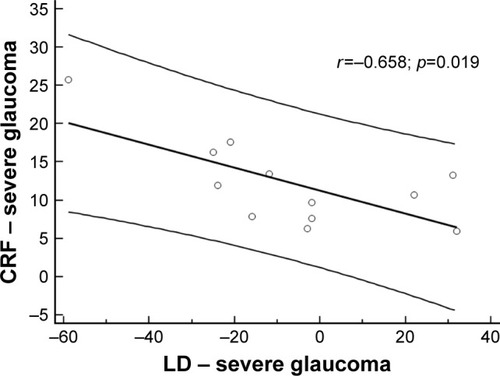
Finally, we found a correlation (r=−658; p=0.019) between the anterior LD and an increase in CRF in the severe glaucoma group ().
Figure 5 Scatterplot illustrating the inverse correlation by Spearman’s test between CRF and LD in eyes with severe glaucoma.
Discussion
The biomechanical properties of the LC have attracted the interest of many researchers in recent years as they might lead to a better understanding of glaucoma pathophysiology.Citation34 An increase in the IOP is thought to induce a strain on the laminar tissue that may put the integrity of the optic nerve fibers at risk. The damage induced on the axons might be the result of a mechanical stress,Citation35 a vascular impairment,Citation36 an increase in the translaminar pressure gradient,Citation12,Citation37–Citation40 or a combination of all these mechanisms.
The importance of IOP on the dynamics of the optic nerve structures has been highlighted by the observation of an anterior displacement of the optic nerve surface after IOP reduction both surgically and with medical treatment.Citation41–Citation43 On the other hand, it has been demonstrated that an increase in the IOP may result in a posterior displacement of the optic nerve head (ONH).Citation22,Citation23 Similar outcomes have been achieved in experimental studies on animals.Citation44
The availability in recent years of SD-OCT with EDI allowed the study of the LC and PT with unprecedented accuracy. This advanced technology provides considerable details even when the globe is compressed and deformed by the application of an external force via an ophthalmodynamometer.Citation24
We observed that an average IOP increase of 12.3±2.4 mmHg determined a mean posterior displacement of the LC both in healthy controls and in eyes with mild glaucoma. However, in eyes with advanced glaucoma, we detected a mean anterior displacement of the LC.
All the groups demonstrated a mean posterior displacement of the PT, although it was significantly lower in the advanced glaucoma group compared with the control group.
Anterior laminar surface response to mechanical strain has been investigated in different study cohorts and with different protocols. This, together with the high degree of biomechanical complexity of the LC and scleral canal, might explain the dissimilar and sometimes contradictory results obtained.
Agoumi et alCitation24 did not find any significant displacement of the LC with SD-OCT following an induced IOP increase with an ophthalmodynamometer in both glaucoma and control subjects. Differences in the baseline characteristics of the patients investigated, including the glaucoma stage (the average MD was -2.8 dB in the study by Agoumi et al), might at least partially explain the inconsistency of our results.
Fazio et alCitation45 found that a biphasic behavior of the LC was dependent on the IOP level in healthy subjects of European descent. The LC displaced posteriorly until the IOP elevation from baseline was within 12 mmHg; after that value, the LC displaced anteriorly.
Previous studies on healthy enucleated human eyesCitation15,Citation16 and primate eyes with 3D histomorphometric analysisCitation46 demonstrated a variable response of the lamina to an increased IOP, ranging from a posterior displacement to a nonsignificant displacement.
On the basis of mathematical models, some authors described the behavior of the laminar tissue as the result of the biomechanical and anatomical properties not only of the LC itself but also of the adjacent scleral tissue.Citation19,Citation20 Recent studies supported the hypothesis of a high degree of complexity in the interaction between the laminar tissue and the peripapillary scleral tissue, which may cause a variable response to the mechanical strain exerted by IOP.Citation47–Citation54
We found that eyes with advanced glaucoma had an overall mean anterior displacement of the LC during acute IOP elevation, which is contrary to the posterior displacement observed in mild glaucoma and healthy eyes. We speculate that the different behavior reflected progressive changes at the level of the laminar and peripapillary scleral tissue. An increasing stiffening of the laminar tissue relative to the surrounding sclera might explain the trend toward an anterior bowing of the anterior laminar surface in eyes with advanced glaucoma during IOP elevation as opposed to that noted in eyes with mild glaucoma and in healthy eyes. The opposite direction of displacement observed in fellow eyes might reflect the progressive anatomical and biomechanical changes occurring within the ocular tissues as the glaucoma stage progresses.
The CCT was previously found to be correlated with optic disc features and the likelihood of VF progression in glaucoma.Citation25–Citation29 However, CCT is not considered a reliable reflection of the rigiditiy of the ocular structures and may not provide a significant description of the biomechanics of the eye.Citation55 Hence, CCT values, which were found to be not significantly different among the groups, have probably a marginal role in the interpretation of our results. Corneal biomechanical parameters, such as CH and CRF, are much more closely related to ocular biomechanics and have been correlated to glaucoma onset and progression.Citation30 While CH is a measure of the viscoelastic dampening features of the cornea, CRF indicates the whole viscoelastic resistance. These indices might also be linked to the overall quality of the ECM.Citation31
We performed an ORA examination at baseline and during an ophthalmodynamometer-induced increase in IOP. We found that b-CH was not significantly different among the groups. On the other hand, the CRF was significantly lower in eyes with glaucoma than in control eyes, but no significant difference was found between the eyes with mild and severe glaucoma.
During the ophthalmodynamometer-induced increase in the IOP, mean CH was significantly lower in eyes with mild and advanced glaucoma than in the controls. However, compared with baseline, only eyes with advanced glaucoma exhibited a significant decrease in CH.
The CRF during IOP elevation was significantly higher in eyes with severe glaucoma compared with the other groups. The mean CRF value was also significantly higher than baseline in eyes with mild and severe glaucoma. We also observed a correlation between the increase in CRF during IOP increase and the anterior displacement of the LC in the severe glaucoma group.
The corneal behavior observed in our experiment is in line with a previously described viscoelastic model of the cornea, where a stiffening of the corneal structure (CRF increase) is accompanied by the parallel reduction of the viscous component (CH reduction).Citation56 A CH reduction and a CRF increase, such as the one observed in eyes with glaucoma during IOP elevation, might be linked to an LC with an impaired capacity to dampen IOP changes. This might increase the susceptibility to glaucoma damage.
A reduction in the CH was previously noted in glaucomatous subjectsCitation57–Citation59 and was thought to be related to deterioration in VF.Citation28,Citation60–Citation64 The potential role of CH in glaucoma as a surrogate for ONH biomechanics is also suggested by the observation that in glaucomatous eyes, CH is correlated to optic nerve surface deformation.Citation23,Citation65 Corneal biomechanical properties might therefore give indirect information on the structural features and vulnerability of the ONH. However, other authors reported a lack of correlation between ORA parameters (both CH and CRF), MD, and the severity of glaucoma.Citation66
Although we observed a lower CH in the glaucoma groups compared with the control group, the difference among the groups failed to reach statistical significance.
In summary, we found that in patients with markedly asymmetrical glaucoma, eyes with advanced glaucoma responded to an acute IOP elevation with an overall mean anterior displacement of the LC as opposed to the posterior displacement observed in eyes with mild glaucoma and healthy eyes.
The CH baseline value was lower (but not significantly) in eyes with glaucoma compared with the controls. During acute IOP elevation, the CH decreased markedly in both the advanced and mild glaucoma eyes to a mean value significantly lower than the one found in healthy eyes.
The CRF value at baseline was lower in glaucoma eyes compared with healthy eyes. However, CRF increased significantly during acute IOP elevation in all the groups, and the increase was significantly higher in eyes with advanced glaucoma.
We also found that in patients with markedly asymmetrical glaucoma damage, the eye with advanced glaucoma shows a positive correlation between the CRF increase and the anterior displacement of the LC during IOP elevation.
In light of our findings, we may formulate a hypothesis to interpret our results despite the complexity of the matter. Raised IOP in POAG patients causes progressive anatomical and biomechanical changes at the level of the LC and adjacent scleral tissue. These alterations might be reflected by the biomechanical response of the cornea and LC to an induced increase in the IOP, which might, in turn, correlate to the stage of glaucoma.
There are several limitations in this study. The groups were small, and the laminar features were manually analyzed instead of being automatically detected and measured by the software. The measurements obtained on the laminar and PTs were limited to 4 scans per eye, which might be insufficient to estimate the actual response of these tissues to biomechanical strain. However, despite these limitations, the inclusion of patients with markedly asymmetrical disease between fellow eyes offered the chance to investigate differences in biomechanical response in different stages of the disease. Further studies with larger groups are necessary to validate our preliminary results.
Acknowledgments
The authors thank mechanical engineer Marco Cellini for his contribution to the understanding of corneal biomechanics after an acute increase in intraocular pressure.
Disclosure
The authors report no conflicts of interest in this work.
References
- GordonMOBeiserJABrandtJDThe Ocular Hypertension Treatment Study: baseline factors that predict the onset of primary open-angle glaucomaArch Ophthalmol2002120671472012049575
- LeskeMCHeijlAHusseinMEarly Manifest Glaucoma Trial GroupFactors for glaucoma progression and the effect of treatment: the early manifest glaucoma trialArch Ophthalmol20031211485612523884
- LeskeMCHeijlAHymanLBengtssonBDongLYangZEMGT GroupPredictors of long-term progression in the early manifest glaucoma trialOphthalmology2007114111965197217628686
- VarmaRMincklerDSAnatomy and pathophysiology of the retina and optic nerveRitchRShieldsMBKrupinTThe Glaucomas2nd ed1St. Louis, MOMosby1996139175
- SigalIAFlanaganJGTertineggIEthierCRPredicted extension, compression and shearing of optic nerve head tissuesExp Eye Res200785331232217624325
- SigalIAFlanaganJGTertineggIEthierCRModeling individual-specific human optic nerve head biomechanics. Part I: IOP-induced deformations and influence of geometryBiomech Model Mechanobiol200982859818309526
- DownsJCRobertsMDBurgoyneCFMechanical environment of the optic nerve head in glaucomaOptom Vis Sci200885642543518521012
- BurgoyneCFDownsJCBellezzaAJSuhJKHartRTThe optic nerve head as a biomechanical structure: a new paradigm for understanding the role of IOP-related stress and strain in the pathophysiology of glaucomatous optic nerve head damageProg Retin Eye Res2005241397315555526
- SigalIAFlanaganJGEthierCRFactors influencing optic nerve head biomechanicsInvest Ophthalmol Vis Sci200546114189419916249498
- BellezzaAJHartRTBurgoyneCFThe optic nerve head as a biomechanical structure: initial finite element modelingInvest Ophthalmol Vis Sci200041102991300010967056
- BurgoyneCFDownsJCBellezzaAJHartRTThree-dimensional reconstruction of normal and early glaucoma monkey optic nerve head connective tissuesInvest Ophthalmol Vis Sci200445124388439915557447
- DownsJCBlidnerRABellezzaAJThompsonHWHartRTBurgoyneCFPeripapillary scleral thickness in perfusion-fixed normal monkey eyesInvest Ophthalmol Vis Sci20024372229223512091421
- EthierCRJohnsonMRubertiJOcular biomechanics and biotransportAnnu Rev Biomed Eng2004624927315255770
- EdwardsMEGoodTAUse of a mathematical model to estimate stress and strain during elevated pressure induced lamina cribrosa deformationCurr Eye Res200123321522511803484
- LevyNSCrappsEEDisplacement of optic nerve head in response to short-term intraocular pressure elevation in human eyesArch Ophthalmol198410257827866721773
- YanDBColomaFMMetheetrairutATropeGEHeathcoteJGEthierCRDeformation of the lamina cribrosa by elevated intraocular pressureBr J Ophthalmol19947886436487918293
- BellezzaAJRintalanCJThompsonHWDownsJCHartRTBurgoyneCFDeformation of the lamina cribrosa and anterior scleral canal wall in early experimental glaucomaInvest Ophthalmol Vis Sci200344262363712556392
- SigalIAFlanaganJGTertineggIEthierCRModeling individual-specific human optic nerve head biomechanics. Part I: IOP-induced deformations and influence of geometryBiomech Model Mechanobiol200982859818309526
- SigalIAFlanaganJGEthierCRFactors influencing optic nerve head biomechanicsInvest Ophthalmol Vis Sci200546114189419916249498
- SigalIAFlanaganJGTertineggIEthierCRModeling individual-specific human optic nerve head biomechanics. Part II: influence of material propertiesBiomech Model Mechanobiol2009829910918301933
- YuenDBuysYMDisc photography and Heidelberg retinal tomography documentation of reversal of cupping following trabeculectomyGraefes Arch Clin Exp Ophthalmol2010248111671167320532551
- Azuara-BlancoAHarrisACantorLBAbreuMMWeinlandMEffects of short term increase of intraocular pressure on optic disc cuppingBr J Ophthalmol19988288808839828770
- WellsAPGarway-HeathDFPoostchiAWongTChanKCSachdevNCorneal hysteresis but not corneal thickness correlates with optic nerve surface compliance in glaucoma patientsInvest Ophthalmol Vis Sci20084983262326818316697
- AgoumiYSharpeGPHutchisonDMNicolelaMTArtesPHChauhanBCLaminar and prelaminar tissue displacement during intraocular pressure elevation in glaucoma patients and healthy controlsOphthalmology20111181525920656352
- PakravanMParsaASanagouMParsaCFCentral corneal thickness and correlation to optic disc size: a potential link for susceptibility to glaucomaBr J Ophthalmol2007911262816973656
- HongSKimCYSeongGJHongYJCentral corneal thickness and visual field progression in patients with chronic primary angle closure glaucoma with low intraocular pressureAm J Ophthalmol2007143236236317258538
- RogersDLCantorRNCatoiraYCantorLBWuDunnDCentral corneal thickness and visual field loss in fellow eyes of patients with open-angle glaucomaAm J Ophthalmol2007143115916117188056
- MedeirosFASamplePAZangwillLMBowdCAiharaMWeinrebRNCorneal thickness as a risk factor for visual field loss in patients with preperimetric glaucomatous optic neuropathyAm J Ophthalmol2003136580581314597030
- JonasJBStrouxAVeltenIJuenemannAMartusPBuddeWMCentral corneal thickness correlated with glaucoma damage and rate of progressionInvest Ophthalmol Vis Sci20054641269127415790889
- CongdonNGBromanATBandeen-RocheKGroverDQuigleyHACentral corneal thickness and corneal hysteresis associated with glaucoma damageAm J Ophthalmol2006141586887516527231
- BeeneLCTraboulsiEISevenICorneal deformation response and ocular geometry: a noninvasive diagnostic strategy in marfan syndromeAm J Ophthalmol201616156.e164.e126432567
- KaraliARussellPStefaniFHTammERLocalization of myocilin/trabecular meshwork-inducible glucocorticoid response protein in the human eyeInvest Ophthalmol Vis Sci200041372974010711688
- LuceDADetermining in vivo biomechanical properties of the cornea with an ocular response analyzerJ Cataract Refract Surg200531115616215721708
- BurgoyneFCDownsJCPremise and prediction-how optic nerve head biomechanics underlines the susceptibility and clinical behavior of the aged optic nerve headJ Glaucoma200817431832818552618
- GaasterlandDTanishimaTKuwabaraTAxoplasmic flow during chronic experimental glaucoma. 1. Light and electron microscopic studies of the monkey optic nerve head during development of glaucomatous cuppingInvest Ophthalmol Vis Sci197817983884681192
- HiraokaMInoueKNinomiyaTTakadaMIschaemia in the Zinn-Haller circle and glaucomatous optic neuropathy in macaque monkeysBr J Ophthalmol201296459760322223748
- MaumeneeAECauses of optic nerve damage in glaucoma. Robert N. Shaffer lectureOphthalmology19839077417526413917
- BerdahlJPAllinghamRRJohnsonDHCerebrospinal fluid pressure is decreased in primary open-angle glaucomaOphthalmology2008115576376818452762
- JonasJBBerenshteinEHolbachLAnatomic relationship between lamina cribrosa, intraocular space, and cerebrospinal fluid spaceInvest Ophthalmol Vis Sci200344125189519514638716
- MorganWHYuDYBalaratnasingamCThe role of cerebrospinal fluid pressure in glaucoma pathophysiology: the dark side of the optic discJ Glaucoma200817540841318703953
- IrakIZangwillLGardenVShakibaSWeinrebRNChange in optic disk topography after trabeculectomyAm J Ophthalmol199612256906958909209
- LeskMRSpaethGLAzuara-BlancoAReversal of optic disc cupping after glaucoma surgery analyzed with a scanning laser tomographOphthalmology199910651013101810328406
- BowdCWeinrebRNLeeBEmdadiAZangwillLMOptic disk topography after medical treatment to reduce intraocular pressureAm J Ophthalmol2000130328028611020405
- MorganWHChauhanBCYuDYCringleSJAlderVAHousePHOptic disc movement with variations in intraocular and cerebrospinal fluid pressureInvest Ophthalmol Vis Sci200243103236324212356830
- FazioMAJohnstoneJKSmithBWangLGirkinCADisplacement of the lamina cribrosa in response to acute intraocular pressure elevation in normal individuals of African and European descentInvest Ophthalmol Vis Sci20165773331333927367500
- YangHDownsJCSigalIARobertsMDThompsonHBurgoyneCFDeformation of the normal monkey optic nerve head connective tissue after acute IOP elevation within 3-D histomorphometric reconstructionsInvest Ophthalmol Vis Sci200950125785579919628739
- SigalIAEthierCRBiomechanics of the optic nerve headExp Eye Res20098879980719217902
- GirardMJSuhJKBottlangMBurgoyneCFDownsJCBiomechanical changes in the sclera of monkey eyes exposed to chronic IOP elevationsInvest Ophthalmol Vis Sci20115285656566921519033
- GrytzRMeschkeGJonasJBThe collagen fibril architecture in the lamina cribrosa and peripapillary sclera predicted by a computational remodeling approachBiomech Model Mechanobiol201110337138220628781
- RobertsMDLiangYSigalIACorrelation between local stress and strain and lamina cribrosa connective tissue volume fraction in normal monkey eyesInvest Ophthalmol Vis Sci201051129530719696175
- RobertsMDSigalIALiangYBurgoyneCFDownsJCChanges in the biomechanical response of the optic nerve head in early experimental glaucomaInvest Ophthalmol Vis Sci201051115675568420538991
- DownsJCSuhJKThomasKABellezzaAJHartRTBurgoyneCFViscoelastic material properties of the peripapillary sclera in normal and early-glaucoma monkey eyesInvest Ophthalmol Vis Sci200546254054615671280
- GirardMJDownsJCBottlangMBurgoyneCFSuhJKPeripapillary and posterior scleral mechanics – part II: experimental and inverse finite element characterizationJ Biomech Eng2009131505101219388782
- YanDMcPheetersSJohnsonGUtzingerUVande GeestJPMicrostructural differences in the human posterior sclera as a function of age and raceInvest Ophthalmol Vis Sci201152282182921051726
- PallikarisIGKymionisGDGinisHSKounisGATsilimbarisMKOcular rigidity in living human eyesInvest Ophthalmol Vis Sci200546240941415671262
- GlassDHRobertsCJLitskyASWeberPAA viscoelastic biomechanical model of the cornea describing the effect of viscosity and elasticity on hysteresisInvest Ophthalmol Vis Sci20084993919392618539936
- ShahSLaiquzzamanMMantrySCunliffeIOcular response analyser to assess hysteresis and corneal resistance factor in low tension, open angle glaucoma and ocular hypertensionClin Experiment Ophthalmol200836650851318954311
- NarayanaswamyASuDHBaskaranMComparison of ocular response analyzer parameters in chinese subjects with primary angle-closure and primary open-angle glaucomaArch Ophthalmol2011129442943421482869
- Grise-DulacASaadAAbitbolOAssessment of corneal biomechanical properties in normal tension glaucoma and comparison with open-angle glaucoma, ocular hypertension and normal eyesJ Glaucoma201221748648921734593
- AnandADe MoraesCGTengCCTelloCLiebmannJMRitchRCorneal hysteresis and visual field asymmetry in open angle glaucomaInvest Ophthalmol Vis Sci201051126514651820574009
- MedeirosFAMeira-FreitasDLisboaRKuangTMZangwillLMWeinrebRNCorneal hysteresis as a risk factor for glaucoma progression: a prospective longitudinal studyOphthalmology201312081533154023642371
- De MoraesCVHillVTelloCLiebmannJMRitchRLower corneal hysteresis is associated with more rapid glaucomatous visual field progressionJ Glaucoma201221420921321654511
- MansouriKLeiteMTWeinrebRNTafreshiAZangwillLMMedeirosFAAssociation between corneal biomechanical properties and glaucoma severityAm J Ophthalmol20121533419.e1427.e122018707
- VuDMSilvaFQHaseltineSJEhrlichJRRadcliffeNMRelationship between corneal hysteresis and optic nerve parameters measured with spectral domain optical coherence tomographyGraefes Arch Clin Exp Ophthalmol201325171777178323519885
- PrataTSLimaVCde MoraesCGFactors associated with topographic changes of the optic nerve head induced by acute intraocular pressure reduction in glaucoma patientsEye (Lond)201125220120721127505
- NongpiurMEPngOChiewJWLack of association between corneal hysteresis and corneal resistance factor with glaucoma severity in primary angle closure glaucomaInvest Ophthalmol Vis Sci201556116879688526517405