
Abstract
Purpose
To estimate the frequency of exfoliation syndrome (XFS) and its association with ocular diseases in Northern Nigeria.
Materials and methods
Consecutive patients who presented to the outpatient department of ECWA Eye Hospital Kano from February 2015 to May 2015 were included in the study. Each patient had a complete ophthalmic examination. The anterior segment examination included tonometry, gonioscopy, and detailed slit-lamp examination to assess for the presence or absence of exfoliation material, inflammatory cells, and other abnormal findings. Patients with exfoliation material on the anterior lens surface and/or pupillary margin in either or both eyes were considered to have XFS. Statistical analysis was performed using the Statistical Package for the Social Sciences version 16.0.
Results
A total of 620 patients living in Northern Nigeria from the 6 geopolitical zones were examined. The majority of them (34.5%) were indigenous Hausas. There was a male preponderance of 56.6%, while the mean age at presentation for examination in all age groups was 55.7±13.7 years. There were 9 patients with XFS; the frequency was 1.5%, with most of the patients being 70–80 years old. In patients who were ≥50 years, the frequency was 2.5%. Patients with XFS had a higher mean age of 68±4.9 years. The frequency of XFS among glaucoma patients was 4.4%, while among cataract patients it was 3.7%. No other associated ocular disease was found in the patients with XFS.
Conclusion
This study shows that XFS does exist in Northern Nigeria, as was found in the South. The prevalence of XFS was, however, not reported in the Nigerian National Blindness and Visual Impairment Survey. Therefore, a population-based study is still needed to determine the true prevalence of XFS in Northern Nigeria.
Introduction
Exfoliation syndrome (XFS) is an age-related, generalized disorder of the extracellular matrix characterized by production and progressive accumulation of a fibrillar material in tissues throughout the anterior segment and also in the connective tissue portions of various visceral organs.Citation1 The disorder was first described by Lindberg in 1917 as grayish flecks on the pupillary border.Citation2 These flecks are termed exfoliation material (XFM). XFS is the most common recognizable cause of open-angle glaucoma (OAG) worldwideCitation3 and can also cause angle-closure glaucoma (ACG).Citation4
XFS has been considered rare in West Africa and among those of African descent in the Western Hemisphere,Citation5 but this observation has begun to change in the last two decades.Citation6,Citation7 A recent review of XFS in sub-Saharan Africa showed that the burden of the disease is high in this region.Citation8 Exfoliation glaucoma is often associated with high intraocular pressure (IOP), which can be very difficult to control, greater visual field (VF) loss, wider IOP variations, and more pronounced optic nerve damage as compared to primary open-angle glaucoma (POAG).Citation3 Cataract surgery in patients with XFS is accompanied by an increase in complications such as lens subluxation, zonular dialyses or breaks, posterior capsular rupture, vitreous loss, subluxated intraocular lens, uveitis, hemorrhage, formation of posterior synechiae, and corneal endothelial decompensation.Citation9
Despite the ocular associations of this condition, little work has been done in West Africa, making XFS poorly understood in the region. In Nigeria, a study done in the South-West by Olawoye et alCitation6 had most of the patients from that geopolitical zone.
The Nigerian National Blindness and Visual Impairment SurveyCitation10 identified cataract and glaucoma as the leading causes of blindness in Nigeria, with the northern part of the country having the highest prevalence. This survey, however, did not report any case of XFS and exfoliation glaucoma. XFS was also not reported in another population-based study done in Ghana.Citation11 To the best of our knowledge, no study has documented the prevalence and clinical characteristics of XFS in Northern Nigeria. We evaluated the prevalence and clinical characteristics of XFS in this region. This preliminary study provides relevant information and baseline knowledge which can be used to design a population-based study in the future.
Materials and methods
This was a prospective, cross-sectional study of patients attending ECWA Eye Hospital Kano. The study population comprised all patients aged ≥30 years who attended ECWA Eye Hospital Kano for the first time between February 2015 and May 2015. shows the map of Nigeria depicting Kano and the other geopolitical zones in Nigeria. The study was guided by the tenets and principles of the Helsinki declaration. Ethical clearance for the study was sought and obtained from Catholic Hospitals’ Ethical Committee based in Our Lady of Apostles Catholic Hospital, Oluyoro Oke-Ofa, Ibadan, before the commencement of the study. A letter of approval was sought and obtained from ECWA Eye Hospital Kano before the commencement of the study.
Figure 1 Map of Nigeria showing the six geopolitical zones.

Patients 30 years and older who did not have any corneal disease which precluded clarity and proper examination of the anterior segment were included in the study. A written informed consent was obtained from all patients recruited into the study. Demographic characteristics such as age, sex, place of residence, educational status, and occupation were obtained from all patients. All patients had visual acuity test (unaided and aided) using standard illuminated Snellen’s chart or illiterate E-chart (where necessary). All patients underwent complete slit-lamp examination, applanation tonometry, and gonioscopy using Goldmann 3-mirror goniolens. The corneal endothelium was examined for the presence of XFM and pigment, as were the pupillary margin and anterior lens capsule. The width of the angle and iris configuration was assessed using the Shaffer grading system.Citation12 Those with open angles were dilated with Mydriacyl and 2.5% Phenylephrine and the anterior lens capsule was assessed in patients with pupillary dilatation of ≥6 mm to identify the central, intermediate, and peripheral zones of XFM deposition. IOP was also checked both prior to and after dilatation. The lens was assessed for the presence of cataract after pupillary dilatation and graded based on maturity and morphology using the World Health Organization classificationCitation13 and classified into cortical, nuclear, and posterior subcapsular cataract.
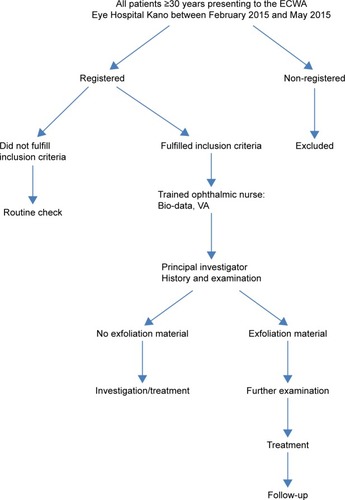
The vertical cup-to-disc ratio (CDR) was examined using the largest value of the cup superiorly from 11:00 to 1:00 o’clock and inferiorly from 5:00 to 7:00 o’clock positions under stereoscopic examination with the slit-lamp biomicroscope and a 78 diopter Volk lens. The optic nerve head was assessed for presence of thinning of neuroretinal rim, focal notching, saucerisation of the optic nerve head, retinal nerve fiber layer loss, and disc hemorrhage. Patients with findings suggestive of glaucoma underwent VF testing using the 24-2 SITA standard program on the Humphrey 740 visual field analyzer (Dublin, California, CA, USA). Patients with XFM in the anterior segment had photographs taken with an anterior segment camera (ChongQing KangHua RuiMing S&T Model: SLM-4ER, ChongQing, People’s Republic of China). shows the patient flow diagram.
Figure 2 Patient flowchart.
Case definitions
Using the American Academy of Ophthalmology Preferred Practice Pattern,Citation14 POAG was defined as a chronic, progressive optic neuropathy in adults in which there is a characteristic acquired atrophy of the optic nerve and loss of retinal ganglion cells and their axons. This condition is associated with an open anterior chamber angle on gonioscopy.Citation14
Glaucoma cases were identified using the International Society of Geographical and Epidemiological OphthalmologyCitation15 criteria as follows:
The highest level of evidence is eyes with optic disc abnormalities (vertical CDR [VCDR]) 97.5th percentile of the hyper-normal population and VF defects compatible with glaucoma, that is, eyes with VCDR ≥0.7 and/or VCDR asymmetry ≥0.2 or a neuroretinal rim width reduced to ≤0.1 CDR (between 11:00 and 1:00 o’clock or 5:00 and 7:00 o’clock) that also shows definite VF defect consistent with glaucoma.
A severely damage optic disc (VCDR 99.5th percentile of the hyper-normal population) if a VF test could not be performed satisfactorily. This means eyes with VCDR ≥0.9 in which a VF could not be done satisfactorily.
If the optic disc could not be examined because of media opacity (hence, no VF test was possible), then a visual acuity 20/400, IOP exceeding the 99.5th percentile of the hyper-normal population (26 mmHg), or evidence of previous glaucoma filtering surgery was taken as sufficient for a diagnosis of glaucoma.
Results
A total of 620 patients aged ≥30 years were recruited into the study from the outpatient department of ECWA Eye Hospital Kano from February 2015 to May 2015. There were 351 males (56.6%) and 269 females (43.4%), with a male to female ratio of 1.3:1. The mean age was 55.7±13.7 years ().
Table 1 Demographic distribution and frequency of the study group
Of the total patients, 162 (26.2%) had no formal education. There were 158 patients (25.4%) with primary education, while 139 patients (22.4%) were educated to a tertiary level and 92 patients (14.8%) to a secondary level. Those with Quranic education were 69 patients (11.2%) ().
Farming was practiced by the majority of patients, 176 (28.4%). There were 27 teachers (4.3%), 139 traders (22.5%), 97 civil servants (15.6%), and 19 engineers (3.1%). Other occupations including security guards, police, artists, and lawyers accounted for 162 patients (26.1%).
The majority of patients, 419 (67.6%), resided in the North-Western geopolitical zone followed by 77 (12.5%) residing in the North-Eastern geopolitical zone, while North-Central geopolitical zone had 59 patients (9.5%). Those living in the South-West accounted for 31 patients (5%), while the South-East was represented 17 patients (2.7%) and South-South by 17 patients (2.7%) ().
The Hausas and Igbos formed the majority of the tribes of patients seen with 216 (34.8%) and 126 (20.3%) patients, respectively, while the Yorubas accounted for 64 (10.4%), Fulani 61 (9.8%), Kanuri 39 (6.3%), and other tribes numbered 114 (18.4%) patients.
Male patients formed the majority of the patients with XFS accounting for 77.8% (p<0.05). There were a total of 9 patients with XFS (1.5%), and the mean age at presentation was 68±4.9 years. The frequency of XFS in patients ≥50 years was 2.5%. Patients within the age group of 70–79 years had the highest prevalence of XFS (5.9%). shows the precise ages of the patients with XFS.
Table 2 Age distribution of 9 patients with XFS
Of the 9 patients with XFS, 3 were Hausas, 2 were Kanuri, and there was 1 patient each from Fulani, Yoruba, Bantu, and Idoma tribes. All patients with XFS were residents of Northern Nigeria for the major part of their lives. There were 5 of 9 patients from the North-Western geopolitical zone accounting for 55.6% followed by the North-Eastern geopolitical zone with 3 (33.3%) and North-Central with 1 (11.1%). Furthermore, 8 patients (88.9%) with XFS were full-time farmers, while one patient was a trader. shows the map of Nigeria depicting the different geopolitical zones.
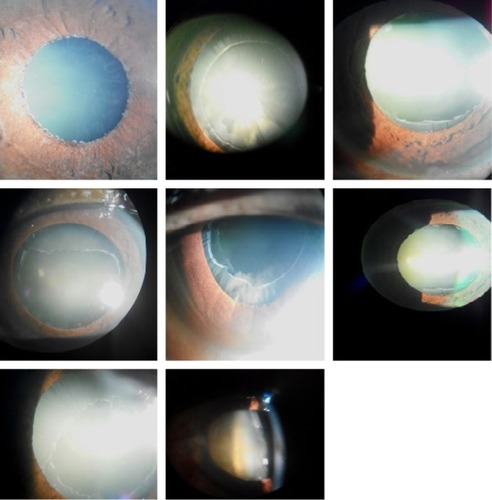
XFS occurred in both eyes in 5 of the 9 patients (55.6%). Two patients (22.2%) had uniocular disease, while two others (22.2%) had XFS in their only eyes, having lost one eye each to harmful traditional practice. XFS was seen in the right eye of the 2 patients with uniocular disease. All patients with XFS had XFM in the peripheral zones of the lens, while 8 patients had XFM on the pupillary margin. One patient had XFM on the lens and not on the papillary margin. shows the anterior segment photos of XFS.
Figure 3 Anterior segment photos of exfoliation syndrome.
There were 115 cases of glaucoma in the study population. The majority, 110 (95.6%), were OAG while 5 (4.4%) had ACG. There were 106 (92.2%) with bilateral glaucoma and 9 (7.8%) with only one eye, the other eye having been lost to trauma, corneal opacity, or harmful traditional practices. Of the 9 patients with XFS, 5 (55.6%) had OAG; there was no case of ACG. The frequency of XFS among glaucoma patients was 4.4%. Two of the 5 patients with exfoliation glaucoma were on medical treatment prior to presentation with a mean IOP of 16.0 mmHg OD and 13.0 mmHg OS, while those not on medical treatment prior to presentation had mean IOP of 28.0 mmHg OD and 24.7 mmHg OS. The mean IOP for patients with XFS was 16.6±5.9 mmHg OD and 18.9±6.0 mmHg OS, while the mean IOP for patients without XFS in was 29.2±8.8 mmHg OD and 30.8±8.6 mmHg OS ().
Table 3 Mean IOP distribution with or without glaucoma in 620 patients
There were 214 patients with cataract. Of this number, 160 (74.8%) had cataract OU, 48 (22.4%) had uniocular cataract, and 6 (2.8%) had cataract in their only eyes. The total number of eyes with cataract was 374, of which 181 was OD and 193 OS.
Of the 9 patients with XFS, 4 had cataract only, 4 had cataract and glaucoma, and 1 patient had glaucoma only. Therefore, 8 patients had cataract, with 6 being bilateral and 2 having it in their only eyes, resulting in a total of 14 eyes; the 2 remaining eyes were blind at presentation. The frequency of XFS among cataract patients was 3.7%. There were 3 eyes with mature cataracts, 11 with immature cataract, and one patient with XFS had no cataract. There were 8 eyes with nuclear sclerosis only, 2 eyes with posterior subcapsular cataract only, 2 eyes with both nuclear sclerosis and posterior subcapsular cataract, and 2 eyes with both cortical cataract and nuclear sclerosis. Nuclear sclerosis therefore occurred in 12 eyes of the patients with XFS. The patients with XFS that required surgery were operated by the most experienced ophthalmic surgeon in the hospital, and there was no perioperative complication.
Discussion
This report confirms the presence of XFS in Northern Nigeria. The frequency of XFS from our study was found to be 1.5%, which is lower than the 2.7% reported in an earlier study in Southern Nigeria.Citation6 There has been great variability shown by several studies in Africa;Citation8 one reason for this may be the different populations studied as some of these studies were hospital basedCitation6,Citation7,Citation16 while others were population-based studies.Citation17,Citation18 It may also be due to the wide difference in the sample size of the studies as well as the age range of individuals analyzed.
This study found a mean age of 55.7±13.7 years in the study population and 68±4.9 years among patients with XFS. This is similar to the study from Southern NigeriaCitation6 with mean age of 65.6±5.6 years in patients with XFS. The youngest age group recorded with XFS in EthiopiaCitation17 is 47 years. BartholomewCitation18 reported that XFS appeared at an earlier age among the black South African population, with a prevalence of 6.4% among patients 30–39 years of age. These differences in presentation might be related to genetic inheritance and nongenetic factors like ultraviolet light exposure.Citation19 Early onset of XFS is however not particularly restricted to the African population alone as it has also been reported among Australian Aborigines, Icelanders, and Lapps.Citation20 The youngest age among XFS patients in this study was 60 years, and the frequency increases with increasing age. For instance, the frequency of XFS in patients ≥40 years in this report was 1.7%, increasing to 4.7% in those ≥60 years. McCarthy et alCitation21 in Australia also reported a prevalence of 5.9% at 40 years, increasing to 12.7% among patients ≥60 years. In a study in Egypt,Citation22 patients aged ≥40 years had a prevalence of 4.14%, which increased to 5.77% in patients ≥60 years. Similar studies from blacks in South AfricaCitation18 and South IndiaCitation23 showed progressive increase in incidence of XFS with age.
Men had a higher frequency of XFS compared to women. Compared to the frequency of men (66.7%) in the study in Southern Nigeria, more men presented to the hospital in this current study (77.8%). This is probably due to the difficulty faced by women in accessing health care in Northern Nigeria compared to the South.Citation24 The male predilection in XFS in Nigeria is comparable to studies from the Aravind comprehensive eye surveyCitation25 where male gender is described as significantly associated with XFS. This could be due to men performing more outdoor activities compared with women. This finding is however contrary to that of the Reykjavik Eye Study,Citation26 which had a higher prevalence in women.
It would be expected that Northern Nigeria with a higher latitude (latitude 12°N) and increased annual sunlight compared to the South (latitude 7°N), should have a higher frequency of XFS, but this was not the case. The study in the South reported a higher frequency. Similarly, TanzaniaCitation27 in the northern tier (latitude 6°S) has no XFS compared to South AfricaCitation17 (latitude 30°S), with a prevalence of XFS of 6.0%–7.7%. Though environmental factors play a role in XFS,Citation28 genetic factors could be a possible reason for this disparity.Citation19 In addition, the studies in the north and south of Nigeria are hospital-based studies and do not provide the true prevalence of the disease. The sample sizes in these studies were relatively small considering the low prevalence of XFS in Nigeria. A large population-based study would be necessary to determine the burden of the disease in Northern Nigeria.
In this study, the frequency of XFS among patients with cataract was 3.7%, and nuclear cataract was the commonest form of cataract among patients with XFS (66.7%). Several studies have shown that nuclear cataract is more often associated with XFS.Citation29,Citation30 This finding, however, is in contrast to findings from the Aravind Comprehensive Eye studyCitation25 where cortical cataract was found to be more common compared to nuclear sclerosis. This is probably due to the method of classification used in the study where mixed cataract was found to be the most common.
In this study, XFS was present in 4.4% of the patients with glaucoma. This is slightly higher compared to the incidence of 3.6% from Southern NigeriaCitation6 and very close to the value from the Andhra Pradesh Eye Disease StudyCitation23 where the prevalence of XFS among glaucoma patients was 4.2%. However, a higher frequency of 13.4% was reported in the Blue Mountain Study,Citation31 and even higher values were obtained from the Scandinavian countries.Citation20 Among the South African blacks, XFS accounted for 24.3% and 23.1% of the cases of OAG in Hlabisa and Temba, respectively.Citation16 In this study, the presence of XFS was associated with OAG as 55.6% of XFS patients had established cases of OAG. This is slightly lower than that seen in the southern part of Nigeria where two-thirds of XFS patients had OAG.Citation6
In the Reykjavik Eye Study,Citation26 eyes with XFS had higher IOP than eyes without XFS. However, there was no direct relationship between IOP and XFS in this study as well as that of Southern Nigeria, as the mean IOP for glaucoma patients with XFS was lower than the mean IOP for glaucoma patients without XFS in both studies. In the Aravind Comprehensive Eye Survey,Citation25 it was stated that IOP measurement cannot be relied upon primarily in testing for glaucoma. Rotchford et alCitation16 also reported that some eyes with signs of XFS had IOP as low as 8 mmHg.
Conclusion
XFS exists in Northern Nigeria as it does in the South. The disease was associated with increasing age. The prevalence of XFS is likely to increase as life expectancy of Nigerians increase. The majority of patients with XFS in this study were engaged in outdoor activities that exposed them to sunlight, indicating that environmental factors could play a role in XFS. Adequate mydriasis and slit-lamp biomicroscopy are essential in assessing the peripheral zone of the lens for exfoliation materials as subtle signs may be missed with poor pupillary dilatation.
This study was a preliminary and hospital-based study; therefore, a population-based study is required to determine the true prevalence of XFS in Northern Nigeria.
Disclosure
The authors report no conflicts of interest in this work.
References
- RitchRSchlötzer-SchrehardtUKonstasAGWhy is glaucoma associated with exfoliation syndrome?Prog Retinal Eye Res200322253275
- LindbergJGClinical Studies of Depigmentation of the Pupillary Margin and Transillumination of the Iris in Cases of Senile Cataract and also in Normal Eyes of the Aged [Thesis]Helsinki, FinlandHelsinki University1917
- RitchRExfoliation syndrome and occludable anglesTrans Am Ophthalmol199492845944
- RitchRExfoliation syndrome-the most common identifiable cause of open-angle glaucomaJ Glaucoma1994317617719920577
- BallSFExfoliation syndrome prevalence in glaucoma population of South LouisianaActa Ophthalmol Suppl198818493982853928
- OlawoyeOOAshayeAOTengCCLiebmannJMRitchRAjayiBGExfoliation syndrome in NigeriaMiddle East Afr J Ophthalmol20121940240523248543
- Chuka-OkosaCMFaalHBOgunroADukeRTypes of glaucoma and recent trends applied in treatment: Observation from a Glaucoma Training Workshop in the GambiaNiger Postgrad Med J20051220320916160723
- OlawoyeOOPasqualeLRRitchRExfoliation syndrome in sub-Saharan AfricaInt Ophthalmol20143451165117324844849
- RitchRSchlotzer-SchrehardtUExfoliation syndromeSurv Ophthalmol20014526531511166342
- AbdullMMSivasubramaniamSMurthyGVNigeria National Blindness and Visual Impairment Study GroupCauses of blindness and visual impairment in Nigeria: the Nigeria national blindness and visual impairment surveyInvest Ophthalmol Vis Sci20095094114412019387071
- BudenzDLBartonKWhiteside-de VosJPrevalence of glaucoma in an urban West African population: the Tema Eye SurveyJAMA Ophthalmol2013131565165823538512
- ShafferRNPrimary glaucomas. Gonioscopy, ophthalmoscopy, and perimetryTrans Am Acad Ophthalmol Otolaryngol19606411212714445374
- ThyleforsBChylackLTJrKonyamaKWHO Cataract Grading GroupA simplified cataract grading systemOphthalmic Epidemiol20029839511821974
- American Academy of OphthalmologyPreferred Practice Pattern201549
- FosterPJBuhrmannRQuigleyHAJohnsonGJThe definition and classification of glaucoma in prevalence surveysBr J Ophthalmol20028623824211815354
- RotchfordAPKirwanJFJohnsonGJRouxPExfoliation syndrome in black south AfricansArch Ophthalmol200312186387012796260
- BedriAAlemuBPseudoexfoliation syndrome in Ethiopian glaucoma patientsEast Afr Med J19997627828010750510
- BartholomewRSPseudo-capsular exfoliation in the Bantu of South Africa. I. Early or pre-granular clinical stageBr J Ophthalmol1971556936995124845
- DamjiKFBainsHSStefanssonEIs pseudoexfoliation syndrome inherited? A review of genetic and nongenetic factors and a new observationOphthalmic Genet1998191751859895242
- ForsiusHPrevalence of pseudoexfoliation of the lens in Finns, Lapps, Icelanders, Eskimos and RussiansTrans Ophthalmol Soc UK197999296298298430
- McCarthyCATaylorHRPseudoexfoliation syndrome in Australian adultsAm J Ophthalmol200012962963310844055
- ShazlyTAFarragANKamelAAl-HussainiAKPrevalence of pseudoexfoliation syndrome and pseudoexfoliation glaucoma in Upper EgyptBMC Ophthalmol2011111821707986
- ThomasRNirmalanPKKrishnaiahSPseudoexfoliation in southern India: The Andhra Pradesh Eye Disease StudyInvest Ophthalmol Vis Sci20054641170117615790875
- AdediniSAOdimegwuCBamiwuyeOFadebiyiODe WetNBarriers to accessing health care in Nigeria: implications for child survivalGlobal Health Action201472349924647128
- KrishnadasRNirmalanPKRamakrishnanRPseudoexfoliation in a rural population of Southern India: The Aravind Comprehensive Eye SurveyAm J Ophthalmol200313583083712788123
- ArnarssonAMDamjiKFSverrissonTSasakiHJonassonFPseudoexfoliation in the Reykjavik Eye Study: prevalence and related ophthalmological variablesActa Ophthalmol Scand20078582282718028119
- BuhrmannRRQuigleyHABarronYPrevalence of glaucoma in a rural East African populationInvest Ophthalmol Vis Sci200041404810634599
- SteinJDPasqualeLRTalwarNGeographic and climatic factors associated with exfoliation syndromeArch Ophthalmol20111291053106021825188
- HietanenJKivelaTVestiETarkkanenAExfoliation syndrome in patients scheduled for cataract surgeryActa Ophthalmol (Copenh)1992704404461414287
- YoungALTangWWLamDSThe prevalence of pseudoexfoliation syndrome in Chinese peopleBr J Ophthalmol20048819319514736771
- MitchellPWangJJHourihanFThe relationship between glaucoma and pseudoexfoliation: The Blue Mountain Eye StudyArch Ophthalmol19991171319132410532440
- National Identity Management CommissionNIMC enrolment centres Available from: https://www.nimc.gov.ng/nimc-enrolment-centres/