Abstract
Purpose
The purpose of this study is to evaluate and compare recurrence rates upon using mitomycin C (MMC) with limbal-conjunctival autograft for treating recurrent pterygia.
Methodology
An interventional, prospective, comparative clinical study was performed in 30 eyes (26 patients) with recurrent pterygia, allocated into two groups: Group A (19 eyes) operated by pterygium excision and limbal-conjunctival autograft transplantation (L-CAT) without MMC and Group B (20 eyes) operated with injection of 0.1 mL of MMC 0.15 mg/mL 1 month before L-CAT surgery. Exclusion criteria included patients with symblepharon, cicatricial conjunctival diseases, limbal stem cell deficiency, and other intraocular diseases.
Results
A total of four cases of recurrences for Group A (P = 0.012) and one case of recurrence for Group B (P < 0.001) were recorded.
Conclusions
Preoperative injection of MMC in low dose and concentration improves the results of L-CAT in recurrent pterygium.
Introduction
A pterygium is a wing-shaped growth of fibrovascular conjunctiva onto the cornea. Its incidence varies across geographical locations. Several hypotheses have been ascribed to its etiology. Currently, it is believed that the pterygium is a growth disorder characterized by conjunctivalization of the cornea due to localized ultraviolet-induced damage to the limbal stem cells. Aggressive pterygial fibroblasts are also responsible for corneal invasiveness.Citation1
The indications for surgery include reduced vision due to encroachment on the visual axis and irregular astigmatism, chronic irritation, recurrent inflammation, restrictive ocular motility, and cosmetic purposes. Numerous surgical techniques including bare sclera excision with or without the use of adjuncts like beta irradiation, thiotepa eye drops, intra- or postoperative mitomycin C (MMC), amniotic membrane transplantation, and conjunctival autograft have been described.Citation2 Pterygium represents a local limbal deficiency. Thus, inclusion of limbal epithelium in the conjunctival graft for pterygium surgery would achieve better anatomic and functional reconstruction after pterygium removal by restoring barrier function of the limbus.Citation3
MMC is an antitumor antibiotic that was first isolated from Streptomyces caespitosus by Wakaki et alCitation4 in 1958, and it acts by inhibiting DNA synthesis. The mechanism of action seems to be inhibition of fibroblast proliferation at the level of the episclera.Citation5 The benefit of MMC is that it has the prolonged if not permanent effect which indicates its toxicity to the cells.Citation6 Adjunctive MMC for pterygium surgery was first described by Kunitomo and MoriCitation7 in Japan in 1963 and in the United States by Singh et alCitation8 in 1988 as postoperative topical MMC of concentration ranging from 0.4 to 1 mg/mL.
Although multiple studies have reported recurrence rates of ~5%–12% with the use of topical MMC,Citation9,Citation10 this technique has been associated with rare but significant conjunctival, sclera, and corneal toxicity.Citation9 In an attempt to decrease ocular morbidity, intraoperative use of MMC was suggested.Citation11 Advantages of this technique include decreasing the MMC dosage and application directly to the area of pathology rather than to the entire ocular surface. A combined pterygium removal with intraoperative MMC and conjunctival autografting was described.Citation12
The purpose of this study was to evaluate the role of MMC injection directly into the surgical site 1 month before limbal-conjunctival autograft transplantation (L-CAT) in recurrent pterygia.
Subjects and methods
A prospective, comparative, interventional clinical study was carried out. This study included 39 eyes (33 patients; 27 unilateral and 6 bilateral) complaining of recurrent pterygium of variable size, duration, and number of recurrences, which are mentioned in . All recurrences happened at least 3 months prior to the MMC injection. Surgeries carried out prior to our study were bare sclera technique for 28 eyes and conjunctival rotational flap for 11 eyes. None had free conjunctival graft or MMC application.
Table 1 Showing descriptive data for both groups
Exclusion criteria were patients with symblepharon, cicatricial conjunctival diseases, limbal stem cell deficiency diseases, and other intraocular diseases. Subjects were recruited from outpatient clinic of Kasr El Aini University and International Eye Hospital in Cairo. They were allocated into 2 groups: Group A included 19 eyes of 15 patients (11 males and 4 females; 4 bilateral and 11 unilateral) all operated by pterygium excision and free autologous limbalconjunctival autograft transplantation (L-CAT) without MMC and Group B included 20 eyes of 18 patients (9 males and 9 females; 2 bilateral and 16 unilateral) all had injection of MMC 1 month before L-CAT surgery.
Preoperative assessment
Both uncorrected and best-corrected visual acuities (UCVA and BCVA, respectively) were measured using decimal system with equivalent standard logarithm of the minimum angle of resolution values. Full ophthalmic examination was performed including intraocular pressure measurement with Goldmann’s applanation tonometry and indirect ophthalmoscopy for fundus.
Pterygium examination was performed to identify its nature (fleshy or fibrotic) and its corneal encroachment. It was graded according to growth onto the cornea: Grade 1 (0–2 mm), Grade 2 (2–4 mm), and Grade 3 (more than 4 mm).
Surgical technique
Anesthesia was given by peribulbar injection of Debocaine® 2.0% (lidocaine HCL 20 mg; El Nasr Chemicals, Cairo, Egypt) and Marcaine® (bupivacaine HCL 0.5%; AstraZeneca AB, Sodertartalje, Sweden) in a ratio of 1:1. Subconjunctival injections at the pterygium and graft sites help in dissection.
Dissection of the pterygium head was carried out with a crescent knife.
Resection was carried out from the underlying sclera or medial rectus.
Excision of the whole pterygium was carried out followed by hemostasis using wet-field cautery.
In Group A, a superficial circumferential incision (around 100-μm depth) in the cornea, 0.5-mm from the superotemporal limbus, was performed to include limbal epithelium to the conjunctival graft. The limbal-conjunctival graft was placed in the correct orientation in the scleral bed and sutured using eight 8/0 vicryl anchoring sutures, conjunctivaepisclera– conjunctiva.
Dressing was carried out with antibiotic-steroid mixtures ointment plus eye cover.
Postoperative treatment given was mixed antibiotic-steroid drops (Dexaflox™, ofloxacin 3.0 mg/mL and dexamethasone 1.0 mg/mL; Jamjoom, Jeddah, Saudi Arabia) and ointment (Tobradex®, tobramycin 0.3 mg/mL and dexamethasone 1 mg/mL; Alcon, Cairo, Egypt) with gradual tapering of medications over 1 month postoperatively.
In Group B, 1 month before carrying out the previously described surgery, under an operating microscope and by using a 30-gauge needle, 0.2 mL of 1% lidocaine anesthetic with epinephrine was injected into the head of the pterygium at the limbus, which caused mild swelling of the conjunctiva. Five minutes after the lidocaine injection, subconjunctival injection at site of pterygium was done using a 30-gauge needle on a tuberculin syringe containing MMC (0.1 mL of 0.15 mg/mL), followed by previously described eye drop and ointment for 1 week.
Evaluation
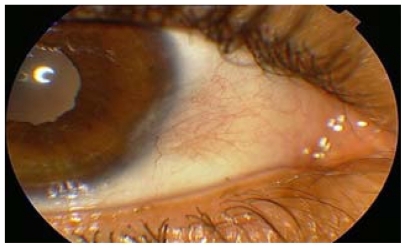
Patients were examined at postoperative days 1, 7, 14, and 30, then every 3 months for 1 year with the exception of 9 eyes which completed only 6 months follow-up. Evaluation is for the occurrence of any complications, such as corneal epithelial toxicity, sclera thinning, or graft sloughing, and for recurrences. and show photographs for 2 cases of Groups A and B, respectively. Recurrence was defined as progressive fibrovascular corneal encroachment after surgery.
Figure 1 Postoperative photograph of a case of Group

Figure 2 Postoperative photograph of a case of Group B.
Results
Data were coded and entered using the statistical package SPSS (version 17; SPSS Inc, Chicago, IL). Data were summarized in percentage for qualitative variables. Comparisons between groups were done using χ2 test. P value ≤ 0.05 was considered statistically significant.
Descriptive results
The study included 39 eyes of 33 patients (20 males and 13 females). Age ranged from 15 to 65 years (mean 43 ± 1.5 years) for Group A and from 27 to 59 years (mean 39 ± 2 years) for Group B.
Visual acuity
Preoperatively, mean UCVA measured for Groups A and B was 0.6 ± 0.1 and 0.56 ± 0.2, respectively. Mean BCVA measured for Groups A and B was 0.9 ± 0.07 and 1 ± 0.1, respectively.
Postoperatively at 1 month follow-up, mean UCVA measured for Groups A and B was 0.58 ± 0.08 and 0.57 ± 0.15, respectively. Mean BCVA measured for Groups A and B was 0.87 ± 0.09 and 1.1 ± 0.08, respectively.
Intraocular pressure
In Group A, the mean of 16 ± 0.5 mm Hg measured preoperatively changed postoperatively at 1 month follow-up to a mean of 15.8 ± 0.2 mm Hg. In Group B, the mean of 17.1 ± 0.4 mm Hg measured preoperatively changed postoperatively at 1 month follow-up to a mean of 16.9 ± 0.1 mm Hg.
Recurrence
A total of four cases of recurrences were recorded for Group A, two at 3 months, one at 6 months, and one at 12 months follow-up. One case of recurrence was recorded for Group B at 6 months follow-up.
Incidence and P value
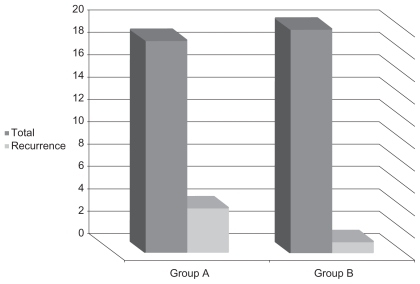
For Group A (19 cases), recurrence in 4 cases (21.1%) (P = 0.012, within the group) was observed. For Group B (20 cases), recurrence in 1 case (5%) (P < 0.001, within the group) was observed. The incidence of recurrence in Group A (4 cases) represents 80% of the total recurrent cases (5 cases) and in Group B (1 case) represents 20% of the total recurrent cases. Comparing the recurrence incidence of the two groups was favorable for Group B (only 1 case of recurrence), but P value was 0.134 (statistically nonsignificant); however, it should be stated that the low number of recurrences in this study may have affected the statistical results of comparing the 2 groups. shows a bar graph with number of recurrences for each group.
Figure 3 A bar graph showing recurrences in both groups; Group A (without MMC) and Group B (with MMC).
Discussion
Pterygium, a worldwide degenerative corneal disease with a multifactorial etiology, is particularly common in tropical countries; the main complication of pterygium treatment is the unpredictable rate and timing of recurrences.Citation13,Citation14
The pterygia recurrence rate reported for patients treated with the bare sclera technique ranges from 24% to 89%,Citation15,Citation16 whereas that reported after conjunctival autograft transplantation ranges from 1.6% to 33%.Citation17,Citation18 Amniotic membrane graft has been used as an alternative to conjunctival autograft transplantation, but the recurrence rate was still as high as 37.5% for recurrent pterygia.Citation19
Recurrent pterygium presents a significant surgical problem. Conjunctival shortening or symblepharon caused by multiple surgeries is especially challenging. Repeated surgical intervention in the limbal area causes severe barrier function destruction. To treat this complicated disorder, both suppression of the subconjunctival fibrosis and the reconstruction of limbal barrier are required. Conjunctival transplantation, lamellar keratoplasty, and limbal autograft transplant have been performed.Citation20
In our study, the idea of using MMC 1 month preoperatively is to further decrease the dosage and morbidity associated with MMC when applied as topical or at time of surgery and to increase its effectiveness by applying the medication in a low concentration and low volume (0.1 mL of 0.15 mg/mL) subconjunctivally 1 month before surgery directly to the target tissue of activated fibroblasts.
Over a follow-up period of 12 months, four cases of recurrences (21.1%) for Group A and one case (5%) for Group B were reported. The superiority of using MMC could be explained by its inhibitor and toxic effect on fibroblasts, and using it 1 month before surgery maximized its effect despite the low dose used.Citation21
Other studies showed rather similar results compared to this study. Donnenfeld and colleagues reported a recurrence rate of 6% on using MMC as a single injection 1 month before surgery with same concentration used in our study; however, all cases operated were primary pterygia.Citation21 Boberg-Ans and colleaguesCitation22 proposed limbal autograft transplantation for the treatment of recurrent and advanced pterygia and reported a 7.4% recurrence rate. However, Gris and colleaguesCitation2 noted no recurrences after L-CAT. Akura and colleaguesCitation23 also investigated a smaller excision graft combination employing a 4-mm window excision with subepithelial pterygium removal, but used intraoperative MMC. Their technique produced no recurrences in 66 patients with follow up ranging from 6 to 32 months.
Conclusion
Although the combined MMC injection followed by L-CAT procedure is time consuming and technically demanding, our reported favorable recurrence rate encouraged us to use this technique for recurrent pterygium treatment.
No broad consensus exists on the best treatment for recurrent pterygium. Further long-term, multicenter, and randomized trials with higher numbers of cases are needed to determine the best treatment method. The results of our study show that both treatment modalities achieved success in the prevention of recurrent pterygium.
Disclosure
The author reports no conflicts of interest in this work.
References
- HirstLWSebbanAChantDPterygium recurrence timeOphthalmology199410147557588152771
- GrisOGüellJLdel CampoZLimbal-conjunctival autograft transplantation for the treatment of recurrent pterygiumOphthalmology2000107227027310690823
- HirstLWThe treatment of pterygiumSurv Ophthalmol200348214518012686302
- WakakiSMarumoHTomiokaKIsolation of new fractions of antitumor mitomycinsAntibiot Chemother19588228240
- DonnenfeldEDPerryHDWallersteinASubconjunctival mitomycin C for the treatment of ocular cicatricial pemphigoidOphthalmology199910617278 discussion 799917784
- SalomãoDRMathersWDSutphinJECuevasKFolbergRCytologic changes in the conjunctiva mimicking malignancy after topical mitomycin C chemotherapyOphthalmology199910691756176010485547
- KunitomoNMoriSStudies on pterygium. Report IV. A treatment of the pterygium by mitomycin C installationActa Soc Ophthalmol Jpn196367601607
- SinghGWilsonMRFosterCSMitomycin eye drops as treatment for pterygiumOphthalmology19889568138213211484
- RubinfeldRSPfisterRRSteinRMSerious complications of topical mitomycin-C after pterygium surgeryOphthalmology19929911164716541454338
- MutluFMSobaciGTatarTYildirimEA comparative study of recurrent pterygium surgery: limbal conjunctival autograft transplantation versus mitomycin C with conjunctival flapOphthalmology1999106481782110201608
- Frucht-PeryJIlsarMThe use of low-dose mitomycin C for prevention of recurrent pterygiumOphthalmology199410147597628152772
- WongVALawFCUse of mitomycin C with conjunctival autograft in pterygium surgery in Asian-CanadiansOphthalmology199910681512151510442896
- StarckTKenyonKRSerranoFConjunctival autograft for primary and recurrent pterygia: surgical technique and problem managementCornea19911031962022055023
- MaharKRNwokoraGERole of mitomycin C in pterygium surgeryBr J Ophthalmol19937774334358343473
- De KeizerRJPterygium excision with or without postoperative irradiation: a double-blind studyDoc Ophthalmol1982523–43093157040006
- SebbanAHirstLWPterygium recurrence rate at the Princess Alexandra HospitalAust N Z J Ophthalmol19911932032061958364
- ChenPPAriyasuRGKazaVLaBreeLDMcDonnellPJA randomized trial comparing mitomycin C and conjunctival autograft after excision of primary pterygiumAm J Opthalmol19951202151160
- LeiGSurgery for pterygium using a conjunctival pedunculated flap slideBr J Ophthalmol199680133348664228
- PrabhasawatPBartonKBurkettGTsengSCComparison of conjunctival autografts, amniotic membrane grafts, and primary closure for pterygium excisionOphthalmology199710469749859186439
- PfisterRRCorneal stem cell disease: concepts, categorization, and treatment by auto- and homo-transplantations of limbal stem cellsCLAO J19942064728149579
- DonnenfeldEDPerryHDFromerSDoshiSSolomonRBiserSSubconjunctival mitomycin C as adjunctive therapy before pterygium excisionOphthalmology200311051012102612750105
- Boberg-AnsJVedel KessingSPterygium excision with limbal autograftEur J Implant Refract Surg199576669
- AkuraJKanedaSMatsuuraKSetogawaATakedaKHondaSMeasures for preventing recurrence after pterygium surgeryCornea200120770370711588420