
Abstract
Aim
The aim of this study was to compare the pre- and posttreatment corneal densitometry and corneal thickness value of keratoconus (KCN) patients managed via contact lenses (CLs) or by both intrastromal corneal rings and contact lenses.
Patients and methods
This prospective study was performed at the Manchester Royal Eye Hospital, UK. Patients were recruited before treatment and followed up for 12 months. Data of corneal densitometry and corneal thickness were collected using the Oculus Pentacam at the pretreatment visit and posttreatment visit at 12 months.
Results
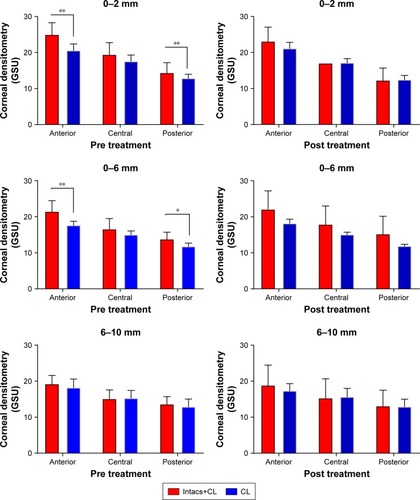
Corneal clarity significantly differs between both groups at pre treatment at zone 0–2 mm for the anterior layer (P=0.002). The same diversity is present at zone 2–6 mm for the anterior layer (P=0.003) and posterior layer (P=0.008). The corneal clarity diversity found was not statistically significant at 12 months post treatment (P>0.05). Corneal thickness was found to be statistically significantly different between pre treatment and post treatment for the CL group for central corneal thickness (CCT) and thinnest area (P=0.01 and P=0.02), respectively.
Discussion
This study shows that KCN management with Intacs was found to be effective in maintaining corneal clarity for a longer time than that with CL alone. On the other hand, corneal clarity reduces with disease progression in cases managed with CLs only. Analysis of Oculus Pentacam images provides an objective evaluation to monitor the corneal status after these different pathways of management.
Introduction
Keratoconus (KCN) is noninflammatory, progressive bilateral dystrophy with corneal stromal thinning.Citation1 Spectacles and/or contact lenses (CLs) are the optional managements available at early stage of the disease. KCN is a progressive disease; when the advanced stage is reached, the only treatment option is corneal transplantation.Citation2,Citation3 In some cases when the cornea is considered clear and the only reasons for corneal transplantation are intolerance of CL or decreased visual acuity (VA), using alternative treatment may be in the best interest of both surgeon and patients.Citation4
CLs have been used for long time to improve VA in KCN even at an advanced stage.Citation5–Citation8 Improving VA without causing any damage to the corneal structures is the most important aim.Citation9 Rigid gas permeable (RGP) lenses are the most widely used lens for keratoconic management at the early stage of the disease.Citation10 The three-point-touch fitting method is the most commonly used method for RGP lenses.Citation11
Intrastromal Corneal Rings Intacs (Addition Technology, Fremont, CA, USA) as keratoconus treatment was first done by Colin et al.Citation12,Citation13 Intacs have been proved to improve the topographic regularity and CL intolerance, both leading to better VA.Citation14–Citation16 Intacs work via shortening the arc and flattening the central cornea along with providing a biomechanical strengthening for the corneal ectatic thinning.Citation17,Citation18 However, an Intac may give a good result in early and moderate stages of the disease, but the Intac is considered poor in advanced stages of keratoconus.Citation19
Corneal clarity in KCN is stated to be at a high level when compared with normal, healthy eyes.Citation20 However, most of keratoconics report increased corneal haze to differing levels. Less attention has been given to the effect of CLs and Intacs on formations of corneal haze.
This study aims to use the Oculus Pentacam (OCULUS Optikgerate GmbH, Wetzlar, Germany) to assess the corneal densitometry level changes in a keratoconic eye before and after fitting with a CL; second, compare changes that takes place in corneal densitometry before and after implanting Intacs in the eye for keratoconic management; and finally, assess the corneal clarity changes between both treatment procedures at pre treatment and post treatment.
Patients and methods
This is a prospective, comparative, and nonrandomized cross-sectional study and was conducted at Manchester Royal Eye Hospital (MREH). This study was approved by Central Manchester University Hospitals NHS Foundation Trust, Manchester, UK, and NREC local ethics committee (ref: 15/NE/0363). The research followed the tenets of the Declaration of Helsinki.
Patients who were aged >13 years at the CL fitting or Intacs and CL placements and had a 1 year follow-up post treatment were selected for this study. A written informed consent was obtained from the patients older than 18 years. For those younger than 18 years, a written consent was obtained from parents and legal guardian in addition to an assent form from the patients. These patients were identified and then recruited following a clinic visit. Clinical notes were examined, where relevant information including patient age, gender, and date of procedures were recorded for descriptive data analysis. Posttreatment parameters including best-corrected visual acuity (BCVA) in logMAR, refraction, and relevant clinical details were extracted from the clinical notes for data analysis. Pretreatment and posttreatment data of corneal densitometry and central corneal thickness (CCT) were retrieved from the Oculus Pentacam.
CL fitting
All patients were fitted with RGP CLs by an optometrist at MREH. The fitting included analysis of the topography results and slit-lamp examination. The fitting procedures followed standard methods for keratoconic patients.Citation11,Citation21,Citation22
Intacs procedure
Intacs fitting was performed by one surgeon for all subjects in this study. The procedure was done using local anesthesia. Mean corneal thickness was >425 µm for all patients and >450 µm at the proposed insertion locations. Keratometry reading showed 58 diopter (D) with mean 50 D and standard deviation (SD) 5.27 for Simk1 and mean 52.77 D and SD 8.34 for Simk2 with clear central cornea. Endothelial cell count was >1,000 cells/mm2. Two Intacs segments of 150–350 µm thickness for each eye were used to embrace the steepest keratoconic meridian at a depth between 300 and 400 µm. The aim was to achieve maximum flattening of the cornea.Citation23 All the cases were fitted with RGP CL based on unsatisfactory VA with spectacles or soft CL correction.
Pentacam imaging
Pentacam topography images are routinely used clinically to assess patients mostly as a corneal diagnostic tool. Densitometry software allows the corneal clarity to be measured from the same image. The protocol takes only 5 minutes, and it is noninvasive, so carries no risks to the patient.Citation24 A good single image of the cornea was taken at each visit, which met the quality requirement determined by Pentacam analysis. The measurements from the Pentacam images were compared for pre treatment and post treatment for both groups at 12 months. The same measurements were compared between groups at 1 year post treatment.
Statistical analyses
IBM SPSS Statistics for Mac, Version 23.0 (IBM Corporation, Armonk, NY, USA) and GraphPad Prism version 7.00 for Windows (GraphPad Software, Inc., La Jolla, CA, USA) were used to perform analysis. Normality of data was assessed using the Shapiro–Wilk W-test. Data were represented in each follow-up as the mean (M)±SD at baseline and 12 months. Independent t-test for data was used to compare both groups. A paired t-test analysis was used to analyze follow-ups as compared to the baseline. A P-value of <0.05 was considered as a statistically significant result.
Results
A total of 27 eyes from 16 patients met our criteria at 12 months posttreatment follow-up. These were seven patients (nine eyes) for Intac treatment with a mean±SD age of 32.04±8.38 years and nine patients (18 eyes) for CL treatment with a mean±SD age of 30.22±7.27 years, which is not statistically significant (P>0.05). The two groups showed similar demographic data.
At pre treatment, the mean (SD) of BCVA logMAR was found to be 0.11 (0.14) for the CL group, whereas it was 0.42 (0.25) for the Intacs group. At post treatment, the mean (SD) of BCVA logMAR was found to be 0.16 (0.35) for the CL group and 0.24 (0.35) for the Intacs group. When both groups were compared in terms of BCVA, a significant difference was found in pre treatment (P<0.001). In contrast, at 12 months post treatment, no statistically significant difference was found between both groups (P>0.05).
The study found a statistically significant increase for the CL group for mean corneal densitometry only in the anterior layer of zone 0–2 mm between pre treatment and 12 months post treatment (P<0.05; ). However, the Intacs group showed no statistical difference between corneal densitometry at pre treatment and 12 months post treatment (P>0.05; ).
Table 1 Mean and SD for corneal densitometry at pre treatment and post treatment for the CL group
Table 2 Mean and SD for corneal densitometry at pre treatment and post treatment for the Intacs group
Corneal densitometry at pretreatment comparison between both groups showed a difference at zone 0–2 mm for the anterior layer (P=0.0001). A significant difference was also seen in the 2–6 mm zone for the anterior layer (P=0.006) and the posterior layer (P=0.01).
Comparing the mean corneal densitometry value between both groups at 12 months post treatment reveals no difference in any zones or layers (P>0.05; ).
Figure 1 A comparison of the pre treatment and post treatment corneal densitometry for both groups at different corneal zones and layers.
Abbreviations: GSU, grayscale unit; CL, contact lens.
Corneal thickness was found to decrease statistically significant between pre treatment and post treatment for the CL group in both CCT and the thinnest area (P=0.02 and P=0.04), respectively. This difference was not seen for the Intacs group (P>0.05, ). Additionally there was a significant difference between both groups at pre treatment for CCT (P=0.02) and thinnest area (P=0.02). Similar differences were found at 12 months post treatment in CCT (P=0.3) and thinnest area (P=0.2; ).
Table 3 Mean and SD for corneal thickness at pre treatment and post treatment at 12 months for CL and Intacs groups
Discussion
Corneal clarity change in KCN has been reported in recent studies.Citation25,Citation26 Factors that can alter corneal clarity include age.Citation27–Citation29 Viral corneal disease as well as keratoconus and Fuchs disease (Fuchs endothelial dystrophy [FED]) can have an impact of decrease in corneal clarity. KCN progression shows decreased corneal clarity.Citation20,Citation30 Management of KCN by corneal collagen cross-linking (CXL) was found to have an effect on corneal clarity and increased corneal haze.Citation31,Citation32 However no reports about the effect of CLs or Intacs on corneal clarity using Pentacam have been published yet.
CL management of KCN is a well-documented evidence-based option for patients. This research did not find any statistical differences in corneal clarity between baseline and 12 months post fitting of CL except at the anterior layer of zone 0–2 mm.
KCN management can involve the Intacs procedure for some advanced cases where patients have difficulty using RGP lenses. This study found no significant change in corneal clarity after 12 months after Intacs were fitted compared to the baseline.
The results for both the Intac and CL groups showed higher corneal haze than published data for age-matched healthy controls at both pretreatment and posttreatment imaging.Citation28,Citation33 Both treatment groups (CLs and INTACS) showed significant differences pretreatment clarity with that at 12 months post treatment, however, there was no difference between the two treatment groups. Other studies of KCN management show a difference between pre treatment and post treatment of corneal clarity, for example, collagen cross-linking where corneal clarity is increased (CXL).Citation32,Citation34
Damage of keratocytes has been associated with haze development post CXL in many reports.Citation33,Citation35,Citation36 It has been reported that corneal morphology can be altered due to a long-period wearing of CLs.Citation37 However, keratocyte density does not seem to be affected by wearing daily CLs for a long period.Citation38 Correspondingly, endothelial cell density was found to be unaffected in keratoconus for those patients who were not wearing CLs.Citation39 However, there are conflicting reports on changes in endothelial density, increasing,Citation40 no change,Citation41 or decreasing,Citation42 for long-time wearing of CL. On the other hand, Intacs placed in the cornea lead to a decrease in irregular astigmatism caused by KCN without attacking the center of the cornea and its tissues.Citation4,Citation43 It is commonly believed that lipid deposits will accumulate after Intac insertion.Citation44 Lipids affect the extracellular matrix in the cornea due to change in the biomechanics,Citation45 and this may change corneal clarity. However, we showed that clarity was increased 12 months after Intacs were fitted.
CLs may cause alteration of corneal thickness.Citation46,Citation47 This could be linked to structural alteration in the cornea due to reduced basal epithelial cells.Citation48 Our result shows statistically significant change between pre treatment and post treatment, which increases the CCT.Citation49 These changes in corneal thickness could be due to inflammation caused by CL wear or induced by an increase in proinflammatory cytokines in tears,Citation50 which increased with wearing CLs.Citation51 However, this study did not find any effect of the Intacs procedure on corneal thickness. These differences of the effect on corneal thickness between both treatment forms despite using CL could be due to lens mechanical effect.Citation52,Citation53
This study was limited by a small sample size; therefore, result is preliminary and needs to be replicated in a large study group. Another limitation was the average age of the participants, which may reflect a stable stage of keratoconic disease progression.
Conclusion
Corneal clarity seems not to be affected by management of the disease progression either by CL alone or Intacs and CL. However, treatment with Intacs seems to stabilize the corneal clarity in comparison with that with CLs alone. Intacs slow down the decrease in clarity associated with the CL treatment alone. Maybe there is less irritation and hence less inflammation after the Intacs are fitted. This study represents the first report, to our knowledge, about change in clarity measured using the Pentacam in keratoconic patients under management by CLs alone or Intacs and CLs. Analysis of Oculus Pentacam images provided an objective evaluation to monitor the corneal status after these treatments.
Acknowledgments
The authors thank the MREH (corneal clinic) for supporting patient’s recruitments for this study. This study was supported by Armed Forces Medical Services, Ministry of Defence, Riyadh, Saudi Arabia.
Disclosure
The authors report no conflicts of interest in this work.
References
- KrachmerJHFederRSBelinMWKeratoconus and related noninflammatory corneal thinning disordersSurv Ophthalmol19842842933226230745
- KymionisGDSiganosCSTsiklisNSLong-term follow-up of Intacs in keratoconusAm J Ophthalmol20071432236244.e23117184717
- Romero-JiménezMSantodomingo-RubidoJWolffsohnJSKeratoconus: a reviewCont Lens Anterior Eye201033415716620537579
- ColinJEuropean clinical evaluation: use of Intacs for the treatment of keratoconusJ Cataract Refract Surg200632574775516765790
- Mandathara SudharmanPRathiVDumapatiSRose K lenses for keratoconus – an Indian experienceEye Contact Lens201036422022220539234
- KokJHvan MilCPiggyback lenses in keratoconusCornea199312160648458233
- BarnettMMannisMJContact lenses in the management of keratoconusCornea201130121510151621993461
- YeungKEghbaliFWeissmanBAClinical experience with piggyback contact lens systems on keratoconic eyesJ Am Optom Assoc19956695395437490414
- BarrJTZadnikKWilsonBSFactors associated with corneal scarring in the Collaborative Longitudinal Evaluation of Keratoconus (CLEK) StudyCornea200019450150710928767
- MandellRBContemporary management of keratoconusInt Cont Lens Clin19972424358
- LeungKKRGP fitting philosophies for keratoconusClin Exp Optom199982623023512482269
- ColinJCochenerBSavaryGMaletFCorrecting keratoconus with intracorneal ringsJ Cataract Refract Surg20002681117112211008037
- RabinowitzYSINTACS for keratoconusInt Ophthalmol Clin200646391103
- ColinJCochenerBSavaryGMaletFHolmes-HigginDINTACS inserts for treating keratoconus: one-year resultsOphthalmology200110881409141411470691
- SiganosCSKymionisGDKartakisNTheodorakisMAAstyrakakisNPallikarisIGManagement of keratoconus with IntacsAm J Ophthalmol20031351647012504699
- Boxer WachlerBSChristieJPChandraNSChouBKornTNepomucenoRIntacs for keratoconusOphthalmology200311051031104012750109
- ShettyRKurianMAnandDMhaskePNarayanaKMShettyBKIntacs in advanced keratoconusCornea20082791022102918812766
- AlióJLShabayekMHArtolaAIntracorneal ring segments for keratoconus correction: long-term follow-upJ Cataract Refract Surg200632697898516814056
- AlióJLShabayekMHBeldaJICorreasPFeijooEDAnalysis of results related to good and bad outcomes of Intacs implantation for keratoconus correctionJ Cataract Refract Surg200632575676116765791
- LopesBRamosIAmbrósioRCorneal densitometry in keratoconusCornea201433121282128625285589
- LeeJLKimMKClinical performance and fitting characteristics with a multicurve lens for keratoconusEye Contact Lens2004301202414722464
- DasSJohnBMohanSRajanMContact lens fitting in keratoconus–a prospective study on visual and functional outcomesInt J Res Med Sci20153818511857
- ArmitageWJTulloABLarkinDFThe first successful full-thickness corneal transplant: a commentary on Eduard Zirm’s landmark paper of 1906Br J Ophthalmol200690101222122316980643
- ChoYKChangHSLaTYTyLAnterior segment parameters using Pentacam and prediction of corneal endothelial cell loss after cataract surgeryKorean J Ophthalmol201024528429021052508
- AnayolMASekerogluMACeranBBDoganMGunaydinSYilmazbasPQuantitative assessment of corneal clarity in keratoconus: a case control study of corneal densitometryEur J Ophthalmol2016261182326165332
- AlzahraniKCarleyFBrahmaACorneal haze in juvenile and adult keratoconus patients after corneal cross-linkingActa Ophthalmol201795S259
- DhubhghaillSNRozemaJJJongenelenSHidalgoIRZakariaNTassignonMJNormative values for corneal densitometry analysis by Scheimpflug optical assessmentInvest Ophthalmol Vis Sci201455116216824327608
- AlzahraniKCarleyFBrahmaAMorleyDHillarbyMCCorneal clarity measurements in healthy volunteers across different age groups: observational studyMedicine20179646e856329145265
- GarzónNPoyalesFIllarramendiICorneal densitometry and its correlation with age, pachymetry, corneal curvature, and refractionInt Ophthalmol20173761263126827837355
- MoftyHAlzahraniKCarleyFEvaluation of corneal symmetry after UV corneal crosslinking for keratoconusClin Ophthalmol20171111
- GutiérrezRLopezIVilla-CollarCGonzález-MéijomeJMCorneal transparency after cross-linking for keratoconus: 1-year follow-upJ Refract Surg2012281178178623347372
- GreensteinSAFryKLBhattJHershPSNatural history of corneal haze after collagen crosslinking for keratoconus and corneal ectasia: Scheimpflug and biomicroscopic analysisJ Cataract Refract Surg201036122105211421111314
- WollensakGSpoerlEWilschMSeilerTKeratocyte apoptosis after corneal collagen cross-linking using riboflavin/UVA treatmentCornea2004231434914701957
- HerrmannCIAHammerTDunckerGIWHaze-Bildung nach Vernetzungstherapie bei Keratokonus [Haze formation after cross-linking therapy in keratoconus]Der Ophthalmologe20081055485487 German17661057
- MazzottaCBalestrazziABaiocchiSTraversiCCaporossiAStromal haze after combined riboflavin-UVA corneal collagen cross-linking in keratoconus: in vivo confocal microscopic evaluationClin Exp Ophthalmol200735658058217760642
- DhaliwalJSKaufmanSCCorneal collagen cross-linking: a confocal, electron, and light microscopy study of eye bank corneasCornea2009281626719092408
- CarlsonKHBourneWMEndothelial morphologic features and function after long-term extended wear of contact lensesArch Ophthalmol198810612167716793196207
- PatelSVMclarenJWHodgeDOBourneWMConfocal microscopy in vivo in corneas of long-term contact lens wearersInvest Ophthalmol Vis Sci2002434995100311923239
- TimucinOBKaradagMFCinalAAskerMAskerSTimucinDAssessment of corneal endothelial cell density in patients with kerato-conus not using contact lensesCont Lens Anterior Eye2013362808523123432
- HollingsworthJGEfronNTulloABIn vivo corneal confocal microscopy in keratoconusOphthalmic Physiol Opt200525325426015854073
- YeniadBYilmazSBilginLKEvaluation of the microstructure of cornea by in vivo confocal microscopy in contact lens wearing and non-contact lens wearing keratoconus patientsCont Lens Anterior Eye201033416717020547093
- NiedererRLPerumalDSherwinTMcgheeCNLaser scanning in vivo confocal microscopy reveals reduced innervation and reduction in cell density in all layers of the keratoconic corneaInvest Ophthalmol Vis Sci20084972964297018579760
- ErtanAKamburoğluGIntacs implantation using a femtosecond laser for management of keratoconus: comparison of 306 cases in different stagesJ Cataract Refract Surg20083491521152618721713
- TwaMDKashRLCostelloMSchanzlinDJMorphologic characteristics of lamellar channel deposits in the human eye: a case reportCornea200423441242015097142
- LyLTMcculleyJPVeritySMCavanaghHDBowmanRWPetrollWMEvaluation of intrastromal lipid deposits after intacs implantation using in vivo confocal microscopyEye Contact Lens200632421121516845269
- YeniadBYiğitBIşseverHKözer BilginLBilginLKEffects of contact lenses on corneal thickness and corneal curvature during usageEye Contact Lens200329422322914555897
- LiuZPflugfelderSCThe effects of long-term contact lens wear on corneal thickness, curvature, and surface regularityOphthalmology2000107110511110647727
- BitirgenGOzkagniciAMalikRAOltuluREvaluation of contact lens-induced changes in keratoconic corneas using in vivo confocal microscopyInvest Ophthalmol Vis Sci20135485385539123882688
- Romero-JiménezMSantodomingo-RubidoJFlores-RodríguezPGonzález-MéijomeJMShort-term corneal changes with gas-permeable contact lens wear in keratoconus subjects: a comparison of two fitting approachesJ Optom201581485525199441
- LemaIDuránJAInflammatory molecules in the tears of patients with keratoconusOphthalmology2005112465465915808258
- LemaIDuránJARuizCDíez-FeijooEAceraAMerayoJInflammatory response to contact lenses in patients with keratoconus compared with myopic subjectsCornea200827775876318650659
- RathiVMMandatharaPSDumpatiSContact lens in keratoconusIndian J Ophthalmol201361841023925325
- GhoshSMutalibHASharanjeet-KaurGhoshalRRetnasabapathySEffects of contact lens wearing on keratoconus: a confocal microscopy observationInt J Ophthalmol201710222828251081