Abstract
Purpose:
To prospectively evaluate the safety, hypotensive effect, and preservation of visual fields of dorzolamide when added to latanoprost.
Subjects and methods:
This study included 46 patients (46 eyes) with primary open-angle glaucoma who had been treated with latanoprost. Dorzolamide (1%) was added to latanoprost, and the intraocular pressure (IOP) was monitored before and after 3, 6, and 12 months. The mean deviation shown by Humphrey perimetry was compared before and after twelve months of treatment. Adverse reactions were monitored over the 12-month study period.
Results:
The mean baseline IOP was 17.2 ± 3.0 mmHg while those after 3, 6 and 12 months of treatment were 14.9 ± 3.0 mmHg, 14.5 ± 3.2 mmHg, and 14.6 ± 2.6 mmHg respectively (P < 0.0001, 1-β(power) = 0.9999571). The absolute reduction of IOP and the percent reduction were similar after 3, 6, and 12 months of treatment. The mean deviation on Humphrey perimetry was similar before and after twelve months of treatment. Three patients discontinued dorzolamide therapy due to elevation of IOP and one patient discontinued it because of adverse reactions.
Conclusion:
Dorzolamide is safe and effective when used for twelve months as add-on therapy to latanoprost for open-angle glaucoma.
Introduction
Prostaglandin analog acts by enhancing the uveoscleral outflow and lowering the intraocular pressure (IOP). The significant effect on reducing IOP and the convenience of once daily administration made Prostaglandin analog eye drops the first line therapy for glaucoma for many ophthalmologists.Citation1 If the reduction of IOP is insufficient, however, switching therapy or adding a new agent is needed.Citation2 β-blockers or carbonic anhydrase inhibitors that inhibit aqueous humor production may be considered as second-line agents to be added on, since they have different mechanisms of reducing IOP to pros-taglandin analog. Use of β-blockers in Japan started about 40 years ago when timolol maleate eye drops became available. As for carbonic anhydrase inhibitors, dorzolamide (0.5% and 1%) was introduced in 1999 and brinzolamide (1%) was released in 2002.Citation3–Citation5 It has been reported that the effect of β-blockers and carbonic anhydrase inhibitors on IOP is comparable, when added to prostaglandin analog therapy.Citation5–Citation7 β-blockers can have systemic adverse effects, however, including induction of asthmatic attack, bradycardia, and depressive symptoms, making it difficult to use these medications in patients with such conditions or in the elderly whose physiological functions are impaired compared with younger individuals. In this respect, carbonic anhydrase inhibitors may have a better safety profile with fewer systemic adverse effects when added to prostaglandin analog therapy.
In previous studies on the IOP-lowering effect of dorzolamide when added to prostaglandin analog therapy, the percent reduction of IOP was reported to be 6.3%–24.0%.Citation4–Citation11 Because dorzolamide is used as a 2% formulation in countries other than Japan,Citation6–Citation10 only a few reports have studied the 1% formulation that is available there.Citation3–Citation5,Citation11 In addition, the duration of treatment in those studies was short (four weeks,Citation4 three months,Citation5 and six monthsCitation11).
We previously reported on the IOP-lowering effect and safety of 1% dorzolamide when added to a prostaglandin analog for six months in patients with primary open-angle glaucoma.Citation11 In the present study, the observation period was extended to twelve months and the effect of dorzolamide on preservation of the visual fields was also evaluated.
Subjects and methods
This was a prospective, multicenter open-label study. The study included 46 patients (22 men and 24 women) with 46 eyes being treated for primary open-angle glaucoma. They were on treatment with latanoprost alone, and dorzolamide was added during the period between June 2008 and May 2009 at Inouye Eye Hospital or 13 other participating institutions. The mean age ± Standard Deviation (SD) (range) of the patients was 69.5 ± 10.5 years (range: 43–87 years). The cases with the mean deviation (MD) value of −24.00 dB and below were excluded from the study. The MD obtained by Humphrey perimetry was −9.0 ± 5.6 dB (−20.05 to −0.63 dB) at baseline and the baseline IOP was 17.2 ± 3.0 (12 to 25) mmHg. The spherical equivalent was −0.5 ± 3.9 (+3.25 to −12.5) D.
In patients with glaucoma affecting both eyes, the eye with the higher IOP was evaluated. If both eyes had the same IOP, the right eye was evaluated.
When the chief physician judged an intraocular pressure drop effect was insufficient, once-daily administration (at night) of latanoprost was continued and 1% dorzolamide (three times daily [tid], morning, noon and night) was added. The IOP was measured by Goldmann applanation tonometry by the same observer at approximately the same time of day in each patient at baseline and every one to two months after starting the administration of dorzolamide. The baseline IOP was compared with that after 3, 6, and 12 months by analysis of variance (ANOVA) with the Bonferroni/Dunnett tests. The reduction of IOP and the percent decrease of IOP relative to baseline after 3, 6, and 12 months were calculated and compared with Friedman’s test. The Humphrey C-30-2 Swedish Interactive Threshold Algorithm (SITA) Standard program was performed at baseline and after twelve months, and the MD values were compared by the paired t-test. Reliability visual field test results <20% fixation errors, <33% false-positive results, and <33% false-negative results. Adverse reactions were evaluated at every visit to hospital. Patients who did not present to hospital for follow-up, who discontinued dorzolamide treatment, who started a new agent, or who underwent surgery during the 12-month study period were excluded from analysis of the IOP data. Differences were considered statistically significant at P < 0.05 for all comparisons. The present study was approved by the ethical committee of Inouye Eye Hospital. The purpose and procedures of the study were explained to the patients and written informed consent was obtained from each subject.
Results
Compared with the baseline IOP (17.2 ± 3.0 mmHg), there was a significant decrease after 3, 6, and 12 months (14.9 ± 3.0 mmHg, 14.5 ± 3.2 mmHg, and 14.6 ± 2.6 mmHg, respectively) in the 46 subjects (P < 0.0001, 1-β (power) = 0.9999571) ().
Figure 1 Intraocular pressure (IOP) before and after addition of dorzolamide.

The absolute reduction of IOP was similar after 3, 6, and 12 months (2.4 ± 2.5 mmHg, 2.7 ± 2.4 mmHg, 2.7 ± 2.6 mmHg, respectively). Likewise, the percent reduction of IOP was similar after 3, 6, and 12 months (13.0 ± 13.4%, 15.1 ± 13.5%, 14.6 ± 12.4%, respectively).
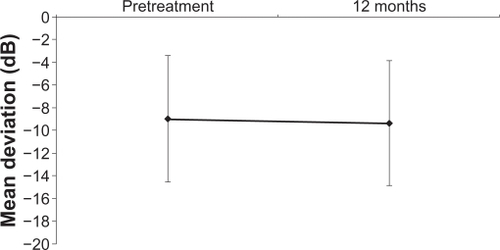
There was no difference of the MD obtained by Humphrey perimetry at baseline and after 12 months of treatment (−9.0 ± 5.6 dB and −9.3 ± 5.5 dB, respectively) ().
Figure 2 Mean deviation at baseline and 12 months after addition of dorzolamide.
Abbreviation: NS, not significant.
During the 12-month period of dorzolamide administration, eleven patients (23.9%) dropped out of the study. Three patients were lost to follow-up, one patient moved and switched to another hospital, one patient suffered from adverse effects (ocular irritation), three patients did not achieve a sufficient reduction of IOP, one patient died of an unrelated disease, one patient underwent surgery for another disease, and one patient was enrolled in another study. The adverse effects observed in one patient resolved after discontinuation of dorzolamide. Of the three patients who did not achieve a sufficient reduction of IOP, one patient increased IOP from 18 mmHg at baseline to 22 mmHg after two months and one patient increased IOP from 13 mmHg at baseline to 14 mmHg after five months. In these two patients, dorzolamide was switched to a β-blocker. In the third patient, IOP increased from 19 mmHg at baseline to 22 mmHg after three months and glaucoma surgery was performed.
Discussion
Several studies have demonstrated that IOP is reduced when dorzolamide is added to basal prostaglandin analog therapyCitation4–Citation11 ().
Table 1 Review of previous studies conducted outside/inside Japan
In Japan, 0.5% and 1% formulations of dorzolamide are used, but only three studies have evaluated the effect of these formulations when added to basal prostaglandin analog therapy.Citation4,Citation5,Citation11 In the study by Maruyama and Shirato, 1% dorzolamide (tid) was added for three months following three months of monotherapy with latanoprost in 33 patients with primary open-angle glaucoma.Citation5 IOP decreased significantly from baseline (16.0 ± 2.1 mmHg), with an absolute reduction and percent reduction of 1.0 mmHg and 6.3%, respectively. In addition, Nakamura et al added 1% dorzolamide (twice daily [bid] or tid) for four weeks in 20 patients with primary open-angle glaucoma, ocular hypertension, or angle-closure glaucoma after laser peripheral iridotomy who had been treated with latanoprost alone, but still had an IOP ≥ 18 mmHg.Citation4 Measurement of the circadian changes of IOP showed a significant decrease from baseline (20.0 mmHg) at all time points, with the absolute reduction and percent reduction being 2.4 to 4.8 mmHg and 12.0 to 24.0%, respectively. In our previous study, 1% dorzolamide (tid) was added to latanoprost or travoprost for six months in 55 patients with primary open-angle glaucoma.Citation11 The IOP decreased significantly from baseline (16.7 ± 2.4 mmHg), and showed an absolute reduction and percent reduction of 2.5 to 2.8 mmHg and 14.2 to 16.4%, respectively. In the present study, 1% dorzolamide (tid) was added to latanoprost for twelve months in 46 patients with primary open-angle glaucoma. We found that the IOP decreased significantly from baseline (17.2 ± 3.0 mmHg), with the absolute reduction and percent reduction being 2.4 to 2.7 mmHg and 13.0 to 15.1%, respectively. These results were consistent with those reported previously.Citation4–Citation11 However, the present study was conducted in an open-label manner, so the IOP-lowering effect of dorzolamide may have been overrated. When the percent reduction of IOP was compared between different formulations of dorzolamide, the IOP lowering effect of the 2% formulation (12.5%–20.6%)Citation6–Citation10 and the 1% formulation (6.3%–24.0%)Citation4,Citation5,Citation11 seemed to be similar.
No previous study has evaluated the effect of dorzolamide on preservation of the visual fields when added to basal prostaglandin analog therapy, possibly because the duration of combined treatment with dorzolamide was short in most studies. In a previous 1-year study, the effect of dorzolamide on the visual fields was not assessed because the study was conducted retrospectively.Citation6 In the present study, the MD obtained by Humphrey perimetry did not change after addition of dorzolamide for 12 months, indicating a positive effect of dorzolamide therapy on preservation of the visual fields. However, the treatment period was only twelve months, so further studies over a longer period are needed.
When dorzolamide is used with a prostaglandin analog, the reported adverse effects include hyperemia, irritation, foreign body sensation, blurred vision, corneal epithelial disorder, and dysgeusia.Citation4,Citation5,Citation7,Citation8,Citation10 In several previous studies, no serious adverse effects were observed,Citation4,Citation5,Citation7–Citation11 which is consistent with the present results. In the present study, sufficient reduction of IOP was not achieved by combined therapy in three patients, suggesting that there is a group of non-responders to dorzolamide.
Conclusion
Dorzolamide had a potent IOP-lowering effect as well as a positive effect on preservation of the visual fields in patients with primary open-angle glaucoma when added to latanoprost for twelve months. However, it remains unclear whether these effects are caused by adding dorzolamide or they can be gained by latanoprost only, or they are synergetic effects of both dorzolamide and latanoprost. It also had a good safety profile and did not cause any serious adverse effects. Thus, the 1% dorzolamide has enough IOP-lowering effect and it may be a useful second-line agent after latanoprost for the treatment of glaucoma.
Acknowledgements
This study was supported by a grant from the Advancement of International Science Foundation.
The following members of the Ochanomizu Ophthalmology Study Group participated in this study.
Ishii Eye Clinic – Yasuhiro Ishii; Ueda Eye Clinic – Hiroko Ueda; Kinugawa Eye Clinic – Yuichi Kinugawa; Goto Eye Clinic – Katsuhiro Goto; Nakai Eye Clinic – Masaki Nakai; Nakai Eye Center – Yoshiyuki Nakai; Fujita Eye Clinic – Natsuya Fujita; Ezure Eye Clinic – Tsukasa Ezure; Nakamura Clinic – Satoshi Nakamura; Shamoto Eye Clinic – Maki Shamoto; Hashida Eye Clinic – Setsuko Hashida; Yanagawa Ophthalmologic Clinic – Takashi Yanagawa; Nishikasai Inouye Eye Hospital – Yasushi Nozaki, Kentaro Shimizu, ShoichiSoeda, Mieko Tsuruoka, and Norie Nozaki; Inouye Eye Hospital – Minako Shiokawa, Risako Higa, Ryo Moriyama, and Hideko Sawada.
Disclosure
The authors report no conflicts of interest in this work.
References
- Van der ValkRWebersCAJanSAIntraocular pressure-lowering effects of all commonly used glaucoma drugsOphthalmology20051121177118515921747
- AraieMAbeHThe Japan Glaucoma Society Guidelines for Glaucoma, 2nd edJpn J Ophthalmol Soc2006110777814
- AraieMKitazawaYAzumaIThe efficacy and safety of dose escalation of dorzolamide used in combination with other topical anti-glaucoma agentsJ Ocul Pharmacol Ther20031951752514733709
- NakamuraYIshikawaSNakamuraY24-hour intraocular pressure in glaucoma patients randomized to receive dorzolamide or brinzolamide in combination with latanoprostClin Ophthalmol2009339540019688026
- MaruyamaKShiratoSAdditive effect of dorzolamide or carteolol to latanoprost in primary open-angle glaucoma. A prospective randomized crossover trialJ Glaucoma20061534134516865013
- O’ConnorDJMartoneJFMeadAAdditive intraocular pressure lowering effect of various medications with latanoprostAm J Ophthalmol200213383683712036683
- TamerCÖksüzHCircadian intraocular pressure control with dorzolamide versus timolol maleate add-on treatments in primary open-angle glaucoma patients using latanoprostOphthalmic Res200739243117164574
- BourniasTELaiJBrimonidinetartate 0.15%, dorzolamide hydrochloride 2%, and brinzolamide 1% compared as adjunctive therapy to prostaglandin analogsOphthalmology20091161719172419592108
- BoyerSGayDAdditive effect of dorzolamide hydrochloride to patients taking travoprost: A retrospective studyOptometry20087950150418722961
- AriciMKTopalkaraAGulerCAdditive effect of latanoprost and dorzolamide in patients with elevated intraocular pressureInter Ophthalmol1998223742
- InoueKWakakuraMKinugawaYShort-term hypotensive effect of dorzolamide added to prostaglandin-related topical medicationJpn J Clin Ophthalmol201064725728