Abstract
We report a case of an acute endothelial failure after the implantation of a new cosmetic, colored, artificial iris diaphragm implant called NewIris®. A 21-year-old woman came to us complaining of progressive loss of vision and pain after NewIris lenses had been implanted. Decreased visual acuity, corneal edema, and increased intraocular pressure in both eyes appeared only 3 weeks after the surgery. The lenses were removed as soon as possible but had already severely affected the endothelial cell count. NewIris implants are an alternative to cosmetic contact lenses, but they are not as safe as other phakic anterior chamber intraocular lenses, nor are they a good option for the patient.
Introduction
Cosmetic, colored contact lenses are worn to give the appearance of a different eye color. A new artificial iris diaphragm implant was first presented by Khan in 2004.Citation1 This device was designed to improve the appearance of patients with partial coloboma, traumatic iridectomy, or ocular albinism. However this implant has also been promoted on the Internet as a cosmetic implant for consumers who wish to change the color of their eyes
We report a severe case of corneal decompensation 3 weeks after the implantation of NewIris® lenses (Kahn Medical Devices Corp, Panama City, Panama) which have resulted in lasting visual impairment despite their removal.
Case report
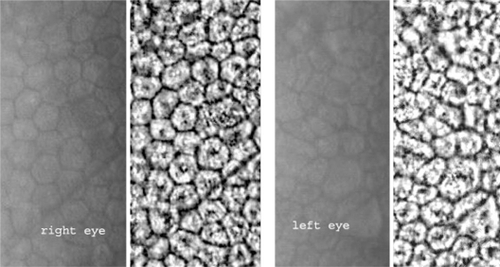
A 21-year-old woman came to the emergency department complaining of progressive loss of vision and pain in both eyes. She had had ocular surgery to change her eye color 3 weeks before in Panama. The patient’s best corrected visual acuity (BCVA) was 20/60 in the right eye (OD) and 20/80 in the left (OS). Slit lamp examination showed significant results of anterior chamber blue-colored implants with angle-support (NewIris implants) (): corneal edema, pigmented precipitates, and flare grade 1 in both eyes. Intraocular pressure (IOP) with Goldman applanation tonometry was 30 mmHg in OD and 35 mmHg in OS. The endothelial cell count was 1071 cells/mm2 in OD and 950 cells/mm2 in OS, with some changes in the size and shape of the cells ().
Figure 1 A) Anterior chamber image. The NewIris lens is positioned over the whole surface of the iris. Corneal incision to insert the lens is at twelve o’clock with a size of 2.8 mm; B) Iris lens diaphragm after explantation.
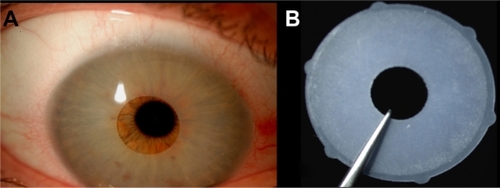
Figure 2 Endothelial cell count. The polymorphism and polymegathism are very evident in both eyes, especially the left one.
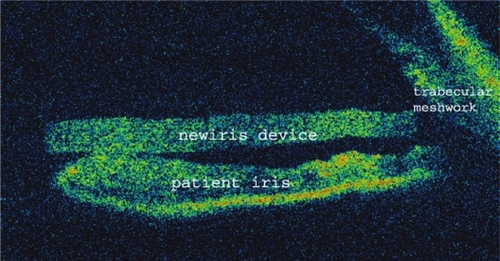
Anterior segment optical coherence tomography (OCT) revealed areas of implant–iris contact and implant–corneal contact ().
Figure 3 Anterior chamber optical coherence tomography. The lens is positioned over the iris and is in contact with all the 360° coneoescleral trabecular meshwork.
Topical dexamethasone 0.1%, timolol 0.05%, and dorzolamide treatment was initiated and continued until surgery. The lenses were removed through a scleral incision. This was achieved by corneal paracentesis and the injection of dispersive viscoelastic to protect the endothelium. Then we performed a large scleral wound (about 10 mm) 3 mm from the corneoscleral limbus. The implant was folded and removed en bloc. Scleral suture with nylon 10/0 was performed to close the wound following anterior chamber washout of the viscoelastic. Once the lenses had been removed we realized that no preventive iridotomies had been made before surgery.
Postoperative treatment consisted of topical dexamethasone 0.1% and tobramycin 0.3% combination drops 4 times a day during the first week, then decreasing to 1 drop per week for 4 weeks of treatment. Timolol 0.05% twice a day was added during the first week.
There were no postoperative recovery complications and at 4 weeks after surgery the BCVA was 20/20 in the OD and 20/25 in the OS. Corneal edema had completely resolved in both eyes but some pigment had been deposited in the corneal endothelium. IOP was controlled without treatment and the endothelial cell count maintained as before the lenses were removed.
Today, 2 years after NewIris removal, visual acuity is maintained at 20/20 in both eyes and IOP is normalized without any treatment. Despite this, severe losses of endothelial cell count and pigmented precipitates remain.
Discussion
The NewIris lens () is made of very thin ophthalmic-grade silicone, colored and elastic, so that it can be inserted through a 2.8 mm clear corneal incision. The device has a diameter of 15 mm with a central opening in the pupil of 3.5 mm and 0.16 mm thickness.Citation1 The NewIris features flaps instead of haptics, by which it can be placed without any supposed pressure on the angle. It is available in 3 colors intended to mimic the natural iris. A similar artificial iris diaphragm implant has been used on patients with anatomic or functional iris deficiencies, aphakia, or cataract,Citation2 with some postoperative complications such as hyphema, inflammation, or IOP increase.
Endothelial cell loss following phakic intraocular lenses (IOL) is well established. The majority of anterior chamber phakic IOL studies rate cell loss at 3 months and 1 year at about 7%.Citation3 Some mechanisms have been suggested to explain the endothelial cell loss: first, the surgery sacrifices a certain amount of endothelial cells (between 2.1% and 7.6%), depending largely on the surgeon’s experience and is generally accepted as inevitable;Citation4 second, the consequence of intermittent contact between the cornea and the IOL;Citation4 and third, the natural age-related endothelial loss (0.6% per year).Citation5 An inflammatory mechanism for endothelial cell deprivation is also thought to play a part.Citation6 In this case we propose that at least two mechanisms were involved in the rapid endothelial cell loss. The first one is the surgery. The NewIris is implanted into the anterior chamber under topical anesthesia. The anterior chamber is filled with viscoelastic and the folded implant is then inserted through a 3.2-mm corneal incision and unfolded. The second is the contact between the lens and the endothelium and between the lens and the anterior part of the iris, as has been shown by OCT images.
It is well known that when an angle-supported anterior chamber IOL is implanted, between 7% and 21% of patients develop high IOP and require treatment.Citation5 The IOP increases because of two mechanisms. The first one is the pupillary block due to lens implantation without iridotomies being performed.Citation4 The second is the pigment dispersion due to contact between the lens and the iris, which can lead to occlusion of the trabecular meshwork. Castanera et alCitation7 reported some irregularities in the NewIris surface by scanning electron microscopy. These irregularities can promote the contact between the lens and the iris, enhancing the pigment dispersion. In this case the hypothesis that pigment dispersion is the primary mechanism of elevated IOP is supported because there was no pupillary block and we saw pigment deposition in the corneal endothelium.
Data on complications associated with cosmetic iris implants are limited. Some authorsCitation8–Citation11 have published previous cases with serious complications related to this lens as glaucoma that required trabeculectomy, corneal decompensation with endothelial keratoplasty, and impairment to visual acuity. In this case the quick removal of the cosmetic iris implants avoided more serious complications but the endothelial cell loss was unavoidable.
The iris-lens diaphragm device is supposed to be a new approach to cosmetic ophthalmological surgery and in theory a more comfortable option than cosmetic contact lenses. As a result of the significant implications from this surgery, the authors strongly recommend not using this type of cosmetic implant.
Disclosure
The authors report no conflicts of interest.
References
- Xth Keratomileusis Study Group International CongressPanama2004
- PozdeyevaNAPashtayevNPLukinVPBatkovYNArificial iris-lens diaphragm in reconstructive surgery for aniridia and aphakiaJ Cataract Refract Surg2005311750175916246779
- LovisoloCFReinsteinDZPhakic intraocular lensesSurv Ophthalmol20055054958716263370
- MimouniFColinJKoffiVBonnetPDamage to the corneal endothelium from anterior chamber intraocular lenses in phakic myopic eyesRefract Corneal Surg199172772811911508
- BourneWMNelsonLRHodgeDOCentral corneal endothelial cell changes over a ten-year periodInvest Ophthalmol Vis Sci1997387797829071233
- Jiménez-AlfaroIBenítez del CastilloJMGarcía-FeijoóJSafety of posterior chamber phakic intraocular lenses for the correction of high myopia: anterior segment changes after posterior chamber phakic intraocular lens implantationOphthalmology2001108909911150270
- CastaneraFFuentes-PáezGTenPPinallaBGuevaraOScanning electron microscopy of explanted cosmetic iris implantsClin Experiment Ophthalmol20103864865120456447
- ArthurSNWrightMMKramarevskyNKaufmanSCGrajewskiALUveitis-glaucoma-hyphema syndrome and corneal decompensation in association with cosmetic iris implantsAm J Ophthalmol200914879079319660735
- ThiagalingamSTarongoyPHamrahPComplications of cosmetic iris implantsJ Cataract Refract Surg2008341222122418571095
- HullSJayaramHMearzaAAComplications and management of cosmetic anterior chamber iris implantsCont Lens Anterior Eye20103323523820382066
- AndersonJEGrippoTMSbeityZRitchRSerious complications of cosmetic NewColorIris implantationActa Ophthalmol20108870070419493251