
Abstract
Purpose
To assess visual and refractive results after bilateral implantation of a trifocal intraocular lens (IOL) in patients with hyperopia.
Methods
In a retrospective nonrandomized study, 196 eyes of 98 patients had bilateral implantation of a trifocal IOL. The Barrett Universal II formula was used for IOL power calculation. Eyes were divided into two groups for their analysis: low-moderate, with IOL power ranging from 22 to 26 D, and high, with IOL power ranging from 25 to 34 D. Refractive error was used to assess predictability, and corrected distance visual acuity (CDVA) and uncorrected distance visual acuity values were used to assess efficacy and safety of the surgery.
Results
Six months postoperatively, our results revealed a Snellen decimal CDVA of 0.97±0.05 and 0.94±0.09, for the low-moderate and high groups, respectively. The low-moderate hyperopia group showed a 75.23% of eyes with 20/20 of CDVA and 100% of eyes with 20/25 of CDVA, and the high hyperopia group showed 60.95% and 94.29% for these values of visual acuity, respectively. The mean postoperative spherical equivalent was −0.25±0.36D and −0.24±0.42D for low-moderate and high hyperopia groups, respectively. In the case of low-moderate hyperopia group, 81% of eyes were within ±0.50D and 99% within ±1.00D. These values were 78% and 95%, respectively, for the high hyperopic eyes.
Conclusion
Bilateral implantation of a trifocal IOL in hyperopic eyes provided good visual and refractive outcomes. The Barrett Universal II formula was accurate in predicting the IOL power in hyperopic eyes.
Introduction
Multifocal intraocular lenses (IOL) have been widely used to provide patients with good visual acuity at different distances, from near to distance vision.Citation1 Traditional bifocal diffractive lenses have been used, being popular among cataract and refractive surgeons. Recent trifocal diffractive lenses, designed to provide patients with good intermediate vision without negatively impacting distance or near visual acuity,Citation2 have been launched in the market, and there is increasing number of implants and designs available. Our group has evaluated different models, with various designs and additions in cataract and refractive lens exchange surgeries,Citation3–Citation20 with excellent outcomes.
However, up to now, few studies have focused on considering specifically the ametropia of the eye in multifocal IOL designs. In fact, only two studies report detailed outcomes of multifocal IOLs in hyperopic eyes,Citation10,Citation11 being short-eyes a very important group of patients who may benefit of multifocal IOLs. These two studies, published previously by our group, showed the visual and refractive outcomes in 170 and 172 hyperopic pseudophakic eyes implanted with the Acri.LISA 366DCitation10 (Carl Zeiss Meditec AG, Germany) and the AcrySof ReSTORCitation11 (Alcon, Fort Worth, TX) bifocal IOLs, respectively. Good visual and refractive outcomes, for low and high hyperopic eyes, were shown at 6 months postsurgery.
To date, no studies have published specific and detailed outcomes for hyperopic eyes using trifocal IOLs. Then, the purpose of the present research was to assess the correction of presbyopia in hyperopia with the implant of the AcrySof IQ PanOptix trifocal IOL (Alcon) in a large sample of patients that underwent cataract surgery.
Methods
This was a retrospective study of 214 eyes of 107 patients who underwent bilateral implantation of the PanOptix trifocal IOL at the Fernández-Vega Ophthalmological Institute (Oviedo, Spain). All patients aimed to correct both refractive error and presbyopia. Informed consent was obtained from all patients after the natural and possible consequences of the study were explained. This was a retrospective study and a standard clinical surgery was performed in our center. Patients signed a specific consent form that covers their privacy and the data can be used for research clinical purposes following the Declaration of Helsinki, and which meets the requirements of our institutional review board. Eyes were divided into 2 groups as a function of the IOL power implanted. The first group, named low-moderate, included eyes with low-moderate hyperopia with IOL power ranging from 22 to 26 D, and the second group, named high, included eyes with high hyperopia, with IOL power ranging from 25 to 34 D.
Inclusion criteria were: maximum axial length of 22.50 mm and refraction ≥+0.50 D, age between 45 and 80 years, bilateral implantation and patient interest to no longer wear any form of spectacle or contact lens correction. Exclusion criteria included >1.25D of corneal astigmatism, history of glaucoma, retina or corneal disease, previous corneal or intraocular surgery, abnormal iris, pupil deformation, neuroophthalmic diseases, and history of prior ocular inflammation.
The AcrySof IQ PanOptix trifocal IOL shows a central nonapodized diffractive zone of 4.5 mm with 15 diffractive rings creating 3 foci: distance, +2.17D and +3.25D and a peripheral refractive zone from 4.5 to 6 mm for distance. The light is split into two, with one half allocated to the distance focus (50%) and the other half split between the near (25%) and intermediate (25%) focus.Citation21 It uses zeroth, second, and third nonsequential diffraction orders for distance, intermediate, and near foci, respectively, and the energy at the first diffractive order is redistributed to optimize the performance at three other focal points.Citation21 The IOL has been designed with a negative asphericity of −0.10 μm. The overall diameter of the lens is 13.0 mm and the optical diameter is 6.0 mm. Lens power varied from +13.0 D to +34.0 D.
All surgeries in this study were operated by phacoemulsification with the Centurion Vision System (Alcon) using topical anesthesia and a clear corneal incision of 2.2 mm on the steep axis by an experienced surgeon using the Callisto system (Carl Zeiss Meditec AG). All eyes were submitted to femtosecond laser-assisted lens surgery using the LenSx platform (Alcon) to perform the anterior capsulotomy and fragment of the nucleus, and a capsular tension ring (CTR) was implanted. The CTR was implanted in order to improve the stability of the capsular bag, to improve the centration of the IOL and to facilitate a possible future exchange of the IOL. The Barrett Universal II formula was used for IOL power calculation.Citation22 The targeted refraction was emmetropia.
Patients were scheduled for clinical evaluation 1 day, 1 week, and 1, 3, and 6 months after surgery. A standard ophthalmologic examination, including manifest refraction, slit-lamp biomicroscopy, Goldmann applanation tonometry, and binocular indirect ophthalmoscopy, were performed at all visits. Snellen decimal monocular uncorrected distance visual acuity (UDVA) and best-corrected distance visual acuity (CDVA) were measured at 100% contrast under photopic conditions (85 cd/m2). All examinations were performed 6 months after IOL implantation. Data analysis was performed using Excel (version 2016, Microsoft Corporation, Redmond, WA, USA).
Results
One hundred and nine eyes were included in the low-moderate hyperopia eye group and 105 eyes in the high hyperopia eye group. Demographic characteristics of the two patient populations are shown in . There were no complications in any of the cases. The age of the patients ranged from 45 to 78 years and the IOL power ranged from 22 to 34D. Detailed values (mean and ranges) for both groups are also shown in .
Table 1 Demographic Characteristics Of Participants Shown As Means, Standard Deviations (SD) And Ranges
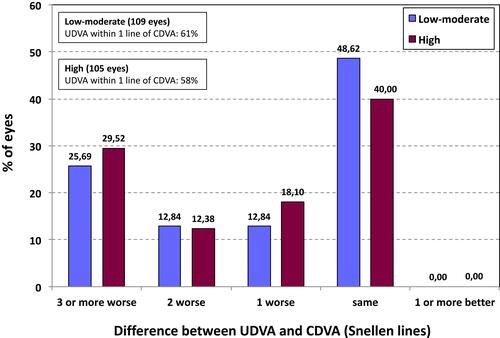
On average, the results that we have obtained at 6 months of follow-up reveal for the low-moderate hyperopia group a monocular distance Snellen decimal UDVA and CDVA of 0.82±0.21 and 0.97±0.05, respectively. For the high hyperopia group, these values were 0.78±0.19 and 0.94±0.09, respectively. shows the cumulative monocular UDVA and CDVA outcomes for both groups. The low-moderate hyperopia group showed a 75.23% of eyes with 20/20 of CDVA and 100% of eyes with 20/25 of CDVA, and the high hyperopia group showed percentages of 60.95 and 94.29 for these values of visual acuity, respectively (being 100% for 20/32). Percentages for UDVA were lower in both groups. Specifically, shows the difference between UDVA and CDVA. The percentage of eyes with UDVA within 1 line of CDVA was similar for the low-moderate and the high hyperopia groups, 61% and 58%, respectively.
Figure 1 Cumulative proportion of eyes having a given uncorrected distance visual acuity (UDVA) and best-corrected distance visual acuity (CDVA) values for low-moderate and high groups, at 6 months postoperatively.
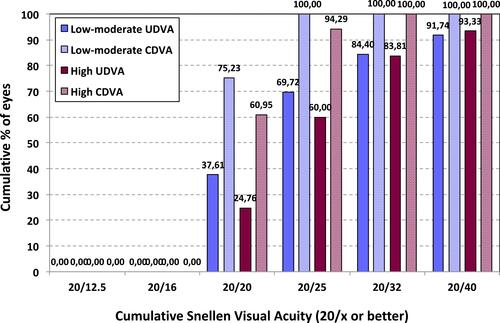
Figure 2 Difference between uncorrected distance visual acuity (UDVA) and best-corrected distance visual acuity (CDVA) values for low-moderate and high groups, at 6 months postoperatively.
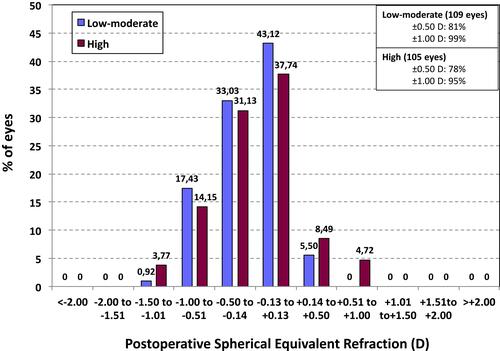
shows the postoperative spherical equivalent found in both groups. The highest percentage for both low-moderate and high hyperopia groups was in the range from −0.13 to +0.13D, with values of 43.12% (47 eyes) and 37.74% (40 eyes), respectively. In the case of low-moderate group, 81% of eyes (n=88) were within ±0.50D and 99% (n=108) within ±1.00D. These values were slightly reduced to 78% (n=82) and 95% (n=100), respectively, for the high hyperopic eyes. Postoperative SE was more distributed around myopic values, but no values larger than −1.50D were found for either group. The mean postoperative spherical equivalent was −0.25±0.36D (ranging from 0.50 to −1.50D) and −0.24±0.42D (ranging from 0.75 to −1.50D) for low-moderate and high hyperopia groups, respectively.
Figure 3 Postoperative spherical equivalent refraction (D) for low-moderate and high groups, at 6 months postoperatively.
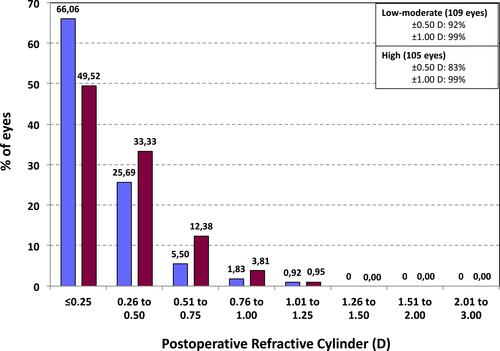
As shown in , the postoperative refractive cylinder was similar between both groups: 92% (n=100) and 99% (n=108) of low-moderate hyperopic eyes were within ±0.50D and ±1.00D, respectively. Similar to what previously happened with the spherical equivalent, values were slightly reduced to 83% (n=87) and 99% (n=104), respectively, for the high hyperopic eyes. 91.7% (n=100) and 82.8% (n=87) of eyes showed a postoperative refractive cylinder ≤0.50D.
Figure 4 Postoperative refractive cylinder (D) for low-moderate and high groups, at 6 months postoperatively.
Mean IOP values changed from 13.65±2.46 mmHg (ranging from 10 to 20 mmHg) before the surgery to 12.33±2.08 mmHg (ranging from 6 to 17 mmHg) after the surgery for the low-moderate hyperopic group. In relation to the high hyperopic group, values were 13.62±2.09 mmHg (ranging from 10 to 19 mmHg) before and 12.18±1.93 mmHg (ranging from 8 to 15 mmHg) after the surgery.
Discussion
One of the most important aspects of the presbyopia correction surgery is the accuracy of the postoperative spherical equivalent. Specifically, the use of different IOL calculation formulas has been discussed. In a recent study published by Melles et al,Citation22 it has been reported that 9.5% of eyes from a sample of 18,501 eyes undergoing cataract surgery showed a short axial length (<22.5 mm). This percentage of eyes is important to be specifically considered for IOL power calculation. In fact, Hoffer and SaviniCitation23 indicated that the main problem with short eyes is due to the higher optical power of the IOL that gives more weight to any possible error in the predicted IOL position. But other factors, such as the power of the cornea, the anterior chamber depth, and the crystalline lens rise, may also play a role.
The analysis of 282,811 cataract extractions reported to the European Registry of Quality Outcomes for cataract and refractive surgery recommends an absolute biometry prediction error of 0.45D or less and that, at least, 90% of cases should fall within an absolute error or ±1.00D.Citation24 We have used the Barrett Universal II formula for IOL power calculation, and our outcomes were good and in agreement with this registry (note that the postoperative spherical equivalent was about a quarter of diopter in both groups). In 2016, Kane et alCitation25 published a series of 156 short eyes (≤22 mm) showing comparable results between this formula with others (Haigis, Hoffer Q, Holladay 1 and 2, SRK/T and T2). They indicated that the difference between formulas was not statistically significant, making it impossible to make any inferences about IOL power formula accuracy for eyes with short axial length based on this study. In another comparative study in 86 short eyes (≤22 mm), Gökce et alCitation26 concluded that there were no statistically significant differences in the median absolute error between the Barret Universal II, Haigis, Hill-RBF, Hoffer Q, Holladay 1, Holladay 2, and Olsen. Shrivastava et alCitation27 concluded that the Barrett Universal II, Haigis, Hoffer Q, Holladay 2, RBF method, and SRK/T formulas were equally accurate in predicting the IOL power in 50 eyes shorter than 22.0 mm. Melles et alCitation22 recently reported that the Barret formula had the lowest mean absolute prediction error for short eyes (n=1270).
Considering our postoperative refraction (spherical equivalent of −0.25±0.36D and −0.24±0.42D, for low-moderate and high hyperopia groups, respectively) it seems that the Barrett Universal II formula may be considered for this trifocal IOL power calculation. Note that 99% and 95% of eyes were within ±1.00D for low-moderate and high hyperopia groups, respectively. In relation to visual acuity, our results show good outcomes for both groups of eyes. CDVA was 0.97 and 0.94 (Snellen decimal) for low-moderate and high hyperopic groups, respectively. The low-moderate hyperopia group showed 100% of eyes with 20/25 of CDVA, and the high hyperopia group showed 94.29%.
Unfortunately, there are no published studies with trifocal IOLs in short eyes in order to be compared with the present research. However, as we have indicated in the introduction section, there are two previous studies with bifocal IOLs in hyperopic eyes. These studies deserve to be analyzed. Fernández-Vega assessed the Acri.LISA 366D bifocal IOL in 170 eyesCitation10 at 6 months postsurgery. They analyzed the performance of this IOL in two groups of eyes: low-moderate hyperopia (IOL power ranging from 21 to 24.5D, with a mean axial length of 22.75 mm and a mean IOL power of 22.77D, n=100) and high hyperopia (IOL power ranging from 25 to 36D, with a mean axial length of 21.19 mm and a mean IOL power of 29.11D, n=70). In this study, good monocular DCVA in both groups was shown: 0.03 and 0.05 logMAR units (about 0.9 decimal) in the low-moderate and high groups, respectively. The mean of postoperative spherical equivalent using the Holladay II formula was near emmetropia (−0.06±0.38D and 0.07±0.36D, for low-moderate and high hyperopia groups, respectively). The percentage of eyes within 0.5D in spherical equivalent was 88% in the low-moderate group and 84.29% in the high hyperopia group, with 100% being within 1D for both groups. The authors concluded that bilateral implantation of this IOL in high hyperopic eyes provided a satisfactory full range of vision comparable with that obtained in eyes with low-moderate hyperopia. These values were also comparable with previous studies of this IOL in other types of eyes.Citation7,Citation12,Citation16–Citation18
Alfonso et alCitation11 in another study evaluated the bifocal AcrySof ReSTOR IOL in 172 eyes. They also analyzed the performance of this IOL in two groups of eyes: low hyperopia (IOL power from 21 to 25D, with a mean IOL power of 23.22D, n=86) and high hyperopia (IOL power from 25.5 to 30D, with a mean IOL power of 27.62D, n=86). The mean value of DCVA was 0.01 and 0.04 logMAR for the low and high hyperopic groups, respectively (about 0.9 Snellen decimal). The percentage of eyes achieving DCVA of 20/25 or better was 90.7% in the high hyperopic group and 96.5% in the low hyperopic group. Postoperative spherical equivalent, using the Holladay II, for the 2 groups was good, showing a mean value lower than a quarter diopter (−0.20±0.56D and −0.08±0.38D for high and low hyperopia, respectively). Similar outcomes were found for medium and long eyes using this IOL model.Citation4,Citation5,Citation8,Citation13,Citation14,Citation16,Citation17
Both studies showed similar outcomes using two different models of bifocal IOLs. The accuracy of the postoperative spherical equivalent was similar using the Holladay II formula.
In conclusion, bilateral implantation of the AcrySof IQ PanOptix IOL in hyperopic eyes provided satisfactory vision and good accuracy in the postoperative refractive error. Similar outcomes were found between low-moderate and high hyperopic eyes. Future studies should include evaluation of the quality of vision at different distances, under different lighting conditions, patient satisfaction questionnaire, and a comparison with other types of trifocal IOLs.
Acknowledgments
This study was presented at the 37th congress of the ESCRS in Paris (France), on 14–19 September 2019.
Disclosure
Professor Robert Montés-Micó report grants from Staar Surgical, contracting from Alcon, and grants from Essilor outside the submitted work. The authors report no other conflicts of interest in this work.
References
- Khandelwal SS, Jun JJ, Mak S, Booth MS, Shekelle PG. Effectiveness of multifocal and monofocal intraocular lenses for cataract surgery and lens replacement: a systematic review and meta-analysis. Graefes Arch Clin Exp Ophthalmol. 2019;257:863–875. doi:10.1007/s00417-018-04218-6
- Shen Z, Lin Y, Zhu Y, Liu X, Yan J, Yao K. Clinical comparison of patient outcomes following implantation of trifocal or bifocal intraocular lenses: a systematic review and meta-analysis. Sci Rep. 2017;7:45337. doi:10.1038/srep45337
- Alfonso JF, Fernández-Vega L, Señaris A, Montés-Micó R. Quality of vision with the Acri. Twin asymmetric diffractive bifocal intraocular lens system. J Cataract Refract Surg. 2007;33:197–202. doi:10.1016/j.jcrs.2006.09.033
- Fernández-Vega L, Alfonso JF, Rodríguez PP, Montés-Micó R. Clear lens extraction with multifocal apodized diffractive intraocular lens implantation. Ophthalmology. 2007;114:1491–1498. doi:10.1016/j.ophtha.2006.10.058
- Alfonso JF, Fernández-Vega L, Baamonde MB, Montés-Micó R. Prospective visual evaluation of apodized diffractive intraocular lenses. J Cataract Refract Surg. 2007;33:1235–1243. doi:10.1016/j.jcrs.2007.03.034
- Fernández-Vega L, Alfonso JF, Baamonde MB, Montés-Micó R. Symmetric bilateral implantation of a distance-dominant diffractive bifocal intraocular lens. J Cataract Refract Surg. 2007;33:1913–1917. doi:10.1016/j.jcrs.2007.06.044
- Alfonso JF, Fernández-Vega L, Señaris A, Montés-Micó R. Prospective study of the Acri.LISA bifocal intraocular lens. J Cataract Refract Surg. 2007;33:1930–1935. doi:10.1016/j.jcrs.2007.06.067
- Alfonso JF, Puchades C, Fernández-Vega L, Montés-Micó R, Valcárcel B, Ferrer-Blasco T. Visual acuity comparison of 2 models of bifocal aspheric intraocular lenses. J Cataract Refract Surg. 2009;35:672–676. doi:10.1016/j.jcrs.2008.11.061
- Alfonso JF, Fernández-Vega L, Amhaz H, Montés-Micó R, Valcárcel B, Ferrer-Blasco T. Visual function after implantation of an aspheric bifocal intraocular lens. J Cataract Refract Surg. 2009;35:885–892. doi:10.1016/j.jcrs.2009.01.014
- Fernández-Vega L, Alfonso JF, Baamonde B, Madrid-Costa D, Montés-Micó R, Lozano J. Visual and refractive outcomes in hyperopic pseudophakic patients implanted with the Acri.LISA 366D multifocal intraocular lens. Am J Ophthalmol. 2009;148:214–220.e1. doi:10.1016/j.ajo.2009.02.036
- Alfonso JF, Fernández-Vega L, Ortí S, Ferrer-Blasco T, Montés-Micó R. Refractive and visual results after implantation of the AcrySof ReSTOR IOL in high and low hyperopic eyes. Eur J Ophthalmol. 2009;19:748–753. doi:10.1177/112067210901900511
- Fernandez-Vega L, Madrid-Costa D, Alfonso JF, Poo-Lopez A, Montes-Micò R. Bilateral implantation of the Acri.LISA bifocal intraocular lens in myopic eyes. Eur J Ophthalmol. 2010;20:83–89. doi:10.1177/112067211002000111
- Alfonso JF, Fernández-Vega L, Ortí S, Ferrer-Blasco T, Montés-Micò R. Differences in visual performance of AcrySof ReSTOR IOL in high and low myopic eyes. Eur J Ophthalmol. 2010;20:333–339. doi:10.1177/112067211002000212
- Alfonso JF, Fernández-Vega L, Valcárcel B, Ferrer-Blasco T, Montés-Micó R. Outcomes and patient satisfaction after presbyopic bilateral lens exchange with the ResTOR IOL in emmetropic patients. J Refract Surg. 2010;26:927–933. doi:10.3928/1081597X-20100114-01
- Alfonso JF, Fernández-Vega L, Ortí S, Montés-Micó R. Refractive lens exchange with distance-dominant diffractive bifocal intraocular lens implantation. Graefes Arch Clin Exp Ophthalmol. 2010;248:1507–1514. doi:10.1007/s00417-010-1345-6
- Alfonso JF, Fernández-Vega L, Puchades C, Montés-Micó R. Intermediate visual function with different multifocal intraocular lens models. J Cataract Refract Surg. 2010;36:733–739. doi:10.1016/j.jcrs.2009.11.018
- Alfonso JF, Puchades C, Fernández-Vega L, Merayo C, Montés-Micó R. Contrast sensitivity comparison between AcrySof ReSTOR and Acri.LISA aspheric intraocular lenses. J Refract Surg. 2010;26:471–477. doi:10.3928/1081597X-20090728-04
- Alfonso JF, Fernández-Vega L, Baamonde B, Ortí S, Montés-Micó R. Refractive lens exchange with Acri.LISA bifocal intraocular lens implantation. Eur J Ophthalmol. 2011;21:125–131. doi:10.5301/EJO.2010.2991
- Alfonso JF, Fernández-Vega L, Blázquez JI, Montés-Micó R. Visual function comparison of 2 aspheric multifocal intraocular lenses. J Cataract Refract Surg. 2012;38:242–248. doi:10.1016/j.jcrs.2011.08.034
- Alfonso JF, Fernández-Vega Cueto L, Belda-Salmerón L, Montés-Micó R, Fernández-Vega L. Visual function after implantation of a diffractive aspheric trifocal intraocular lens. Eur J Ophthalmol. 2016;26:405–411. doi:10.5301/ejo.5000741
- Lee S, Choi M, Xu Z, Zhao Z, Alexander E, Liu Y. Optical bench performance of a novel trifocal intraocular lens compared with a multifocal intraocular lens. Clin Ophthalmol. 2016;10:1031–1038. doi:10.2147/OPTH
- Melles RB, Holladay JT, Chang WJ. Accuracy of intraocular lens calculation formulas. Ophthalmology. 2018;125:169–178. doi:10.1016/j.ophtha.2017.08.027
- Hoffer KJ, Savini G. IOL Power calculation in short and long eyes. Asia Pac J Ophthalmol (Phila). 2017;6:330–331. doi:10.22608/APO.2017338
- Lundström M, Dickman M, Henry Y, et al. Risk factors for refractive error after cataract surgery: analysis of 282 811 cataract extractions reported to the European Registry of Quality Outcomes for cataract and refractive surgery. J Cataract Refract Surg. 2018;44:447–452. doi:10.1016/j.jcrs.2018.01.031
- Kane JX, Van Herdeen A, Atik A, et al. Intraocular lens power formula accuracy: comparison of 7 formulas. J Cataract Refract Surg. 2016;42:1490‒1500. doi:10.1016/j.jcrs.2016.07.021
- Gökce SE, Zeiter JH, Weikert MP, Koch DD, Hill W, Wang L. Intraocular lens power calculations in short eyes using 7 formulas. J Cataract Refract Surg. 2017;43:892–897. doi:10.1016/j.jcrs.2017.07.004
- Shrivastava AK, Behera P, Kumar B, Nanda S. Precision of intraocular lens power prediction in eyes shorter than 22 mm: an analysis of 6 formulas. J Cataract Refract Surg. 2018;44:1317–1320. doi:10.1016/j.jcrs.2018.07.023