Abstract
Background
The evaluation of intravitreal bevacizumab treatment for delayed radiation maculopathy and papillopathy after irradiation for maxillary sinus cancer.
Case report
A patient with radiation maculopathy and papillopathy was treated with intravitreal bevacizumab (1.25 mg). Main outcome measures included fundus photography, angiography, and optical coherence tomography (OCT). Two weeks after intravitreal bevacizumab, visual acuity improved from 0.4 to 1.2. Fundus examination revealed decreased disc swelling, peripapillary hemorrhage, and macular edema. OCT demonstrated complete resolution of serous retinal detachment. At the 12-month follow-up, there was no exudation recurrence. No ocular or systemic side effects were observed.
Conclusion
Intravitreal bevacizumab can be used to treat radiation maculopathy and papillopathy. Antivascular endothelial growth factor therapy may decrease tissue injury associated with radiation vasculopathy.
Introduction
Radiation maculopathy and papillopathy are complications after radiotherapy for intracranial, skull base, and paranasal sinus tumors. Macular edema and serous retinal detachment associated with radiation maculopathy may lead to severe visual loss. Although the natural history of radiation papillopathy may be more favorable than previously assumed,Citation1 any cases associated with underlying vascular disorders are more likely to be aggressiveCitation2 and there is still no evidence-based treatment for radiation papillopathy. More recently, there have been isolated reports of intravitreal bevacizumab (Avastin®; Genentech Inc, San Francisco, CA) for radiation optic neuropathy or maculopathy secondary to plaque radiotherapy.Citation3–Citation5 Here, a case of delayed radiation maculopathy and papillopathy secondary to irradiation for maxillary sinus cancer that was successfully treated with intravitreal bevacizumab is reported.
Case report
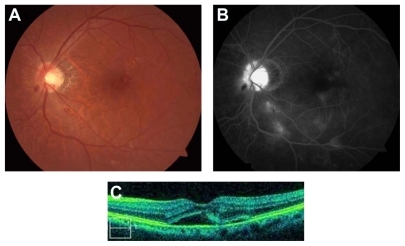
A 73-year-old male presented with acute decrease in vision in the left eye 6 years after irradiation therapy for maxillary sinus cancer. The patient had a history of irradiation with a dose of 50–55 Gy in 1.8–1.9 Gy fractions to the cancer without invasion into eye and orbit. Treatment was performed with an anterior and lateral pair of 45° wedged beams. The patient had no diabetes mellitus or vascular disease. On presentation, his best-corrected visual acuity was 1.2 OD and 0.4 OS. Ophthalmoscopy was normal in the right eye but showed optic disc swelling with peripapillary hemorrhage, retinal exudates, and intraretinal microangiopathy in the left eye (). The corresponding fluorescein angiogram (FA) revealed optic disc and macular edema, capillary nonperfusion, microaneurysms, and vascular leakage (). Optic coherence tomography (OCT) demonstrated serous retinal detachment (SRD) ().
Figure 1 (A) Before bevacizumab treatment, the color fundus photograph shows optic disc swelling, peripapillary hemorrhage, retinal exudates and microangiopathy. (B) Fluorescein angiography demonstrates optic disc and macular edema, capillary nonperfusion, and microaneurysms. (C) Optical coherence tomography (OCT) reveals serous retinal detachment.
The patient was suspected to have radiation maculopathy and papillopathy in the left eye. Intravitreal bevacizumab (1.25 mg in 0.05 mL) was provided to reduce vascular hyperpermeability and intraretinal neovascularization. Two weeks after the administration, visual acuity improved to 20/20 with resolution of SRD. Two months after administration, a color photograph showed decreased optic disc swelling, hemorrhage, and exudates (). OCT demonstrated complete regression of SRD (). The corresponding FA revealed markedly reduced macular edema, decreased intraretinal microangiopathy, and vascular leakage (). These findings were maintained over 12 months and at the last follow-up ().
Figure 2 (A) Two months after treatment with intravitreal bevacizumab, the color fundus photograph shows a decrease of optic disc swelling, peripapillary hemorrhage, retinal exudates and microangiopathy. (B) Fluorescein angiography demonstrates improvement of optic disc and macular edema, and microaneurysms. (C) Optical coherence tomography (OCT) reveals complete resolution of serous retinal detachment.
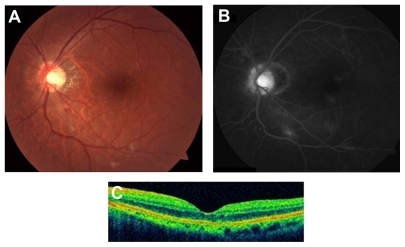
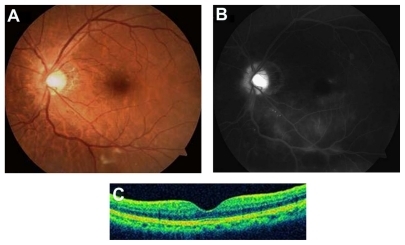
Figure 3 (A) Twelve months after treatment, the color fundus photograph shows a well-defined optic disc margin with resolution of peripapillary hemorrhage. (B) Fluorescein angiography demonstrates persistent decreased microangiopathy and vascular leakage. (C) Optical coherence tomography (OCT) reveals sustained resolution of serous retinal detachment.
Discussion
Radiation-induced retinopathy, maculopathy, and papillopathy are serious complications of head and neck radiotherapy. Takeda et al have suggested that radiation dose and area irradiated are the most important factors in the development of radiation retinopathy.Citation6 The results in that study showed that 8/14 (57%) eyes that received 50 Gy or more, over 60% or more of the area of the retina, developed severe retinal complications. Citation6 Parsons et al also indicated that, in the dose range 45–50 Gy, 8/15 (53%) eyes studied developed retinopathy and there was an increased risk of injury among patients who received fractional doses of over 1.9 Gy.Citation7 Kim et al reported that 63/93 (67.7%) patients who received 70 cobalt Gy equivalents (CGEs) developed papillopathy a median of 1.5 years after irradiation.Citation1 Demizu et al found that the maximum dose to the optic nerve (>110 GyE3) was significant for the occurrence of radiation-induced optic neuropathy.Citation8 Taking this into consideration, in this case with a dose of 50–55 Gy in 1.8–1.9 Gy fractions over 50% of the area of the retina, radiation damage to the macula and optic nerve might be mild and the clinical findings might support that view.
Intravitreal bevacizumab has been used in the treatment of age-related macular degeneration,Citation9 retinal vein occlusion,Citation10 and diabetic retinopathyCitation11 as it inhibits the formation of abnormal blood vessels and reduces vascular hyperpermeability from vascular cell damage. Hopewell has noted that radiation injury in the central nervous system is a consequence of vascular rather than neural cell damage.Citation12 Radiation papillopathy and maculopathy represent disc swelling, peripapillary hemorrhage, hard exudates, intraretinal edema, subretinal fluid, and capillary nonperfusion by a radiation- damaged microvasculature. Thus, intravitreal bevacizumab may be a reasonable choice for radiation papillopathy and maculopathy, although the severe forms may need more aggressive therapy.
Rapid and sustained resolution of radiation maculopathy and papillopathy by intravitreal bevacizumab may be a consequence of prompt reduction of vascular hyperpermeability and prolonged suppression of retinal neovascularization. A recent study has shown that intravitreous ranibizumab (Lucentis®; Genentech, San Francisco, CA) can be used for radiation maculopathy.Citation13 Because ranibizumab is in the form of smaller molecules with rapid wash-out, the drug may need repeated monthly injections and consequently increase the opportunity for adverse events such as endophthalmitis and retinal detachment. In addition, the costs of ranibizumab are much higher than bevacizumab. Therefore, the longer acting and less expensive bevacizumab therapy may be best for the treatment of radiation vasculopathy, although risk–benefit comparisons are still needed.
Disclosure
The authors report no conflicts of interest in this work.
References
- KimIKLaneAMEganKMMunzenriderJGragoudasESNatural history of radiation papillopathy after proton beam irradiation of parapapillary melanomaOphthalmology201011781617162220363507
- GragoudasESLiWLaneAMMunzenriderJEganKMRisk factors for radiation maculopathy and papillopathy after intraocular irradiationOphthalmology199910681571157710442906
- FingerPTAnti-VEGF bevacizumab (Avastin®) for radiation optic neuropathyAm J Ophthalmol2007143233533817258524
- FingerPTChinKAnti-vascular endothelial growth factor bevacizumab (Avastin) for radiation retinopathyArch Ophthalmol2007125675175617562985
- GuptaAMueckeJSTreatment of radiation maculopathy with intravitreal injection of bevacizumab (Avastin)Retina200828796496818698298
- TakedaAShigematsuNSuzukiSLate retinal complications of radiation therapy for nasal and paranasal malignancies: relationship between irradiated-dose area and severityInt J Radiat Oncol Biol Phys199944359960510348290
- ParsonsJTBovaFJFitzgeraldCRMendenhallWMMillionRRRadiation retinopathy after external-beam irradiation: Analysis of time-dose factorsInt J Radiat Oncol Biol Phys19943047657737960977
- DemizuYMurakamiMMiyawakiDAnalysis of vision loss caused by radiation-induced optic neuropathy after particle therapy for head-and-neck and skull-base tumors adjacent to optic nervesInt J Radiat Oncol Biol Phys20097551487149219345516
- AveryRLPieramiciDJRabenaMDCastellarinAANasirMAGiustMJIntravitreal bevacizumab (Avastin) for neovascular age-related macular degenerationOphthalmology2006113336337216458968
- IturraldeDSpaideRFMeyerleCBIntravitreal bevacizumab (Avastin) treatment of macular edema in central retinal vein occlusion: a short-term studyRetina200626327928416508427
- HaritoglouCKookDNeubauerAIntravitreal bevacizumab (Avastin) therapy for persistent diffuse diabetic macular edemaRetina2006269999100517151486
- HopewellJWRadiation injury to the central nervous systemMed Pediatr Oncol1998Suppl 1199659940
- FingerPTChinKJIntravitreous ranibizumab (Lucentis) for radiation maculopathyArch Ophthalmol2010128224925220142553