Abstract
Purpose
To evaluate the improvement in subjective symptoms of conjunctivochalasis after bipolar coagulation.
Methods
Forty-three eyes of 26 patients (average age, 75.7 ± 8.4 years) were included in this study. The inferior conjunctivas were cauterized between April 2009 and June 2010. Surgery involved pinching the excess conjunctiva and performing bipolar cauterization after subconjunctival injection of a local anesthetic agent. Patients were asked to describe the postoperative foreign-body sensation and change in subjective symptoms 1 month postoperatively, with the preoperative symptom score defined as 10.
Results
Twenty-two patients (84.6%) reported symptom relief immediately after the procedure, though all patients had a mild gritty sensation for 1–2 weeks postoperatively. The mean postoperative symptom score obtained from the questionnaire was 3.27 ± 3.31, which was significantly lower than the preoperative score (P < 0.0001). No patients had experienced recurrent symptoms at the end of the follow-up period.
Conclusion
Thermal cauterization can achieve conjunctival shrinkage and adherence to the subconjunctival tissues. Operation time is only a few minutes, postoperative pain is not severe, and the procedure can be performed in an outpatient clinic, all of which represent benefits to the patients.
Introduction
Conjunctivochalasis (CCh) causes watery eyes, ocular irritation, and discomfort.Citation1 Epiphora is mainly caused by obstruction of the lacrimal pathway; however, some patients suffer from epiphora without lacrimal pathway obstruction, and CCh may contribute to this condition in these patients. A histopathologic study showed fragmentation of the subconjunctival elastic fibers in patients with CCh.Citation2 Slack conjunctival tissue can lead to epiphora through mechanical blockage of the lacrimal puncta and tear meniscus formation.Citation3–Citation5 Moreover, the mechanical friction and negative pressure exerted on the tear meniscus by CCh also cause corneal and/or conjunctival abrasion, leading to ocular irritation and discomfort. Removal of the slack conjunctiva enables the formation of a clear single tear meniscus and eliminates the blocked puncta, which leads to improved epiphora.Citation4 Although CCh is a common cause of ocular surface irritation and watery eyes, it is generally diagnosed as an unidentified complaint, and its clinical relevance is often overlooked.Citation6
Various therapeutic procedures for CCh have been reported, including resection, suture fixation, fibrin glue, and coagulation.Citation1,Citation7,Citation8 Resection is the most common treatment in Japan,Citation1 but this procedure requires conjunctival stitches, which often generate severe postoperative ocular irritation that may worsen several weeks postoperatively. However, the suturing and fibrin glue methods also have disadvantages. The long-term effects of the suture method have not been confirmed. The fibrin glue method with amniotic membrane transplantation is newer and able to omit the need for stitches, but is not widely performed because the amniotic tissue is not readily available. Haefliger et alCitation9 reported the use of a coagulation method using bipolar forceps, but all patients had residual postoperative CCh. Gumus et alCitation10 also reported CCh areas were decreased significantly after conjunctival cauterization for CCh using anterior segment optical coherence tomography.
This paper reports a new surgical method for CCh using bipolar forceps. Changes in subjective postoperative symptoms were assessed using a questionnaire.
Materials and methods
A total of 43 consecutive eyes of 26 patients (18 women, 8 men; age range, 56–87 years; mean, 75.7 ± 8.4) were examined at the Department of Ophthalmology, Gunma University School of Medicine or Saku General Hospital, from April 2009 to June 2010. The inclusion criteria were (1) the presence of excess conjunctiva emerging above the edge of the lower eyelid, and (2) subjective symptoms such as epiphora, irritation, and discomfort which were not improved by topical medication, including artificial tears, hyaluronic acid and/or nonsteroidal anti-inflammatory drugs. The subjective preoperative symptoms are shown in . Eleven patients had epiphora, 12 had ocular irritation, and three had ocular discomfort. One surgeon (KT) performed all examinations and operations. Patients with lacrimal pathway occlusion, including obstruction of the lacrimal canaliculus and nasolacrimal duct, ectropion of the lacrimal puncta, horizontal eyelid laxity, and eyelash/globe contact were excluded. All research and interviews complied with the guidelines of the Declaration of Helsinki. All patients provided informed consent. The postoperative follow-up periods ranged from 59 to 465 days (average, 220.5 ± 111.2).
Table 1 Patient symptoms
The originally developed technique of bipolar coagulation using the tuck and coagulation method to shrink excessive conjunctiva is described below ().Citation1 After application of topical anesthetics of oxybuprocaine hydrochloride, 0.2 mL of 1% lidocaine with epinephrine was injected into the space between the conjunctiva and Tenon’s capsule. Intraoperatively, the patients were instructed to look upward. The excess conjunctiva was grasped 4 mm from the limbus and coagulated, starting with low voltage (power level 0.6) bipolar cauterization (TB50, B Braun Aesculap, Japan) and gradually increasing the voltage until the conjunctiva was coagulated. Coagulation was considered to be adequate when the conjunctiva turned white. Coagulation was performed at 5–10 sites in an arc on the inferior bulbar conjunctiva (). The slack conjunctiva shrank and tightened immediately after coagulation. The procedure only took a few minutes to complete for each eye (see “CCh coagulation movie.mpg,” which demonstrates this procedure). Postoperative betamethasone phosphate ophthalmic ointment was administered to prevent acute chemosis, and levofloxacin ophthalmic solution and betamethasone phosphate ophthalmic solution were prescribed to be taken six times daily. One week postoperatively, fluorometholone four times daily was substituted for these drops. All drugs were stopped 1 week later. Patients were asked to remember the severity of the subjective symptoms preoperatively. They were then asked to rate their symptoms 1 month postoperatively on the basis of “If the greatest severity of preoperative symptoms was 10, on a scale of 1 to 10, how great are the present symptoms? (better or worse?)”, and “Was the irritation in the immediate postoperative period mild, moderate, or severe?”.
Figure 1 Schema of conjunctival coagulation. The operator instructs the patient to gaze upward and picks up the conjunctiva using hook forceps (red). The tissue was coagulated using coagulation forceps (blue) and minimal electrical power. Yellow bursts indicate coagulation.
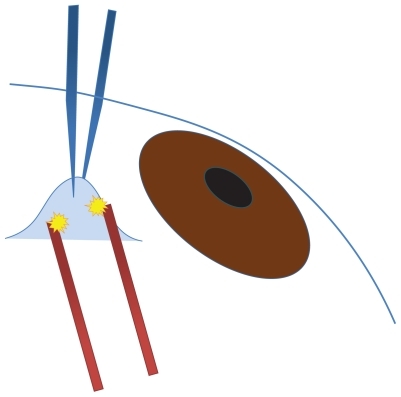
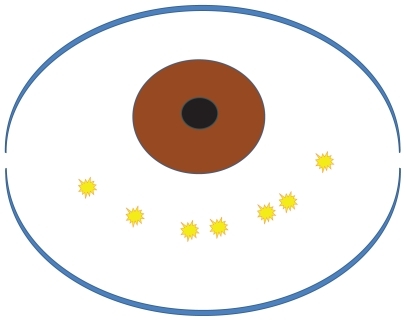
Figure 2 Schema of the coagulation area. The surgical area is in the inferior conjunctiva, 4 mm below the corneal limbus. The inferonasal and inferotemporal areas, which are hidden by the lower eyelid, should also be treated. Five to ten pulsatile coagulations are applied to the inferior conjunctiva (yellow bursts).
Statistical analyses were performed using Mann–Whitney’s U test. Values of P < 0.05 indicated statistical significance. All statistical analyses were carried out using SPSS for Windows (SPSS Japan Inc, Tokyo, Japan).
Results
All patients reported only mild postoperative irritation. A total of 24 patients had conjunctival injection that resolved within 2 weeks, though this was prolonged for 1 month in two patients with severe dry eye. The coagulated region was stained with fluorescein 1 week postoperatively in all patients. The subjective symptoms resolved along with diminution of the staining. The coagulated conjunctiva adhered to the sclera or Tenon’s capsule within 1 month (–), and the integrity of the tear meniscus was restored in all but two patients. These two patients had severe CCh with drooping lower eyelids, and residual postoperative CCh. No severe side effects such as symblepharon or restriction of ocular motility developed. The subjective symptoms clearly decreased, but a second surgery was performed to further improve the outcome in one patient. A normal tear meniscus was obtained after the second procedure. No recurrent CCh developed postoperatively in any patient during the observation period.
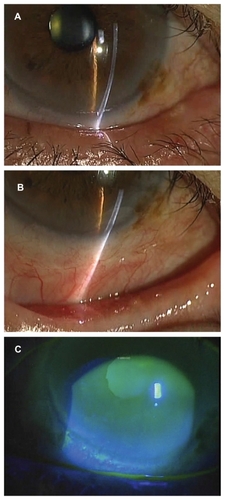
Figure 3 The patient presented with ocular irritation. (A) Preoperative photograph showing CCh on the edge of the lower eyelid. The patient also had keratoconjunctivitis sicca. (B) A preoperative photograph showing fluorescein staining. The CCh divides the tear meniscus into two layers. Punctate conjunctivitis is seen on the CCh.
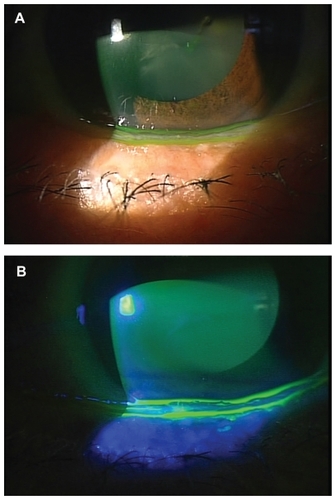
Figure 4 Photograph 1 month postoperatively. (A) The conjunctivochalasis has resolved, but slight conjunctival injection remains. (B) A white scar has formed in the coagulated region and is accompanied by mild injection. Conjunctival injection tends to be prolonged in patients with keratoconjunctivitis sicca.
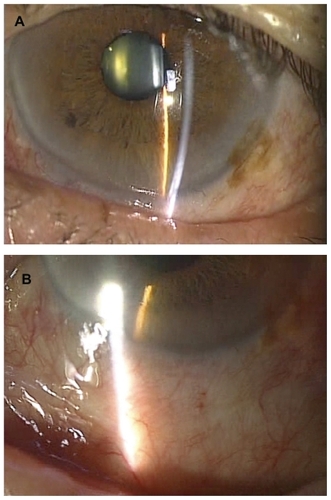
Figure 5 Photograph 3 months postoperatively. (A) The conjunctivochalasis has resolved. Ocular irritation has decreased to 10% of the preoperative level. (B) White scar tissue has formed in the area of coagulation, but is inconspicuous. (C) Photograph obtained 3 months postoperatively showing fluorescein staining. The single tear meniscus is restored and the watery eye has resolved.
The mean postoperative symptom score was 3.27 ± 3.31, which was significantly lower than the preoperative symptom score (P < 0.0001). The preoperative symptoms improved in 22 cases (84.6%), but not in the other four cases (15.4%). Two patients with no improvements in subjective symptoms had watery eyes, one patient had ocular irritation, and one patient had discomfort. There was no correlation between the type of subjective symptoms and the postoperative scores. No patient complained of worsened subjective symptoms.
Discussion
Patients with CCh were treated using the coagulation method involving bipolar coagulation. The operation was performed rapidly in a clinic setting, and no patients experienced intolerable postoperative ocular irritation. The goal of surgery to treat CCh is to remove and anchor the slack conjunctiva.Citation11 The authors of this present paper have previously performed conventional resection, but this does not eliminate severe postoperative irritation caused by the residual knots and persistent small lacerations in the sutured wound. The coagulation methodCitation9,Citation10 achieves conjunctival shortening by electrical coagulation, which also promotes fixation of the conjunctiva to the sclera or Tenon’s capsule. Although the authors of this present paper were unable to confirm tissue adhesion, no eyes showed overflow of the conjunctival tissue at the inferior edge of the eye postoperatively. Because the excess conjunctiva may be functionless, the method did not restrict ocular movement. The short surgical time was a further advantage of this method; surgery was completed in about 5 minutes per eye. The ease of performance and lack of requirement for special instruments means that this procedure represents an easily accessible treatment for both patients and medical staff at the outpatient clinic. Because no sutures are placed in the conjunctiva, most patients experienced no postoperative discomfort.
The surgical benefit of the coagulation method can be measured on the basis of the difference between preoperative and postoperative subjective symptom scores. Although the National Eye Institute Visual Function Questionnaire is the major instrument used to investigate visual function,Citation12–Citation14 it is unsuitable for evaluating the discomfort associated with CCh. In the current study, the questionnaire was adapted to measure the subjective symptoms of CCh. Because of the unknown extent of postoperative change, a nonsliding scale was used to assess the subjective symptoms.
CCh is often diagnosed as an unidentified complaint in elderly patients. Because the symptoms of CCh are not severe, its treatment should not be a burden for patients. Resection of the conjunctiva sometimes leads to postoperative foreign-body sensation and ocular pain. However, no patients reported severe postoperative irritation or pain after use of the current method.
A second operation was needed in one patient with severe CCh, but because the procedure is not painful, a second procedure is generally considered to be acceptable. Patients should be advised preoperatively of the advantages (short surgical time, mild postoperative irritation) and potential disadvantage (repetition of surgery) of this method.
Although Haefliger et alCitation10 previously reported a coagulation method for CCh using bipolar forceps, residual postoperative CCh was present in all their patients. Because the slack conjunctiva was not grasped with forceps, their method only coagulated the conjunctival surface, resulting in only slight shrinkage and fixation of the conjunctival tissue. The coagulation method used in this current study has improved on this by grasping a large amount of slack conjunctival tissue, making it possible to treat sufficient tissue and cause scar formation in the deeper subconjunctival tissue. This coagulation method appears to produce better outcomes than the method of Haefliger et al.Citation9
The coagulation method caused only mild postoperative irritation or pain, and the coagulated area did not form any tissue defects visible by biomicroscopy. The coagulated region was covered by white, slightly elevated tissue that could be stained by fluorescein, and which resolved within 1 week postoperatively. The authors speculated that this white tissue was a remnant of the necrotic tissue resulting from coagulation, and that the postoperative irritation was reduced because this tissue covered the coagulated area, in contrast with the resection method, which denudes the epithelial surface and exposes nerve endings.
There was no recurrence of CCh during the observation period, but the long-term prognosis is unknown. Conjunctival injuries need about 3 weeks to heal, and tissue remodeling takes about 2–3 months.Citation15–Citation17 The observation period in the current study was sufficiently long to predict that the long-term recurrence rate was likely to be low.
In conclusion, the coagulation method for treating CCh, involving bipolar coagulation with conjunctival pinching, had a high success rate, a short surgical time and short recovery time, and represented a minimal treatment burden for patients. Patients with CCh not associated with other complaints should thus undergo coagulation treatment prior to the consideration of other treatment methods.
Supplementary video
The video shows the procedure of the method used in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
- YokoiNInatomiTKinoshitaSSurgery of the conjunctivaDev Ophthalmol20084113815818453766
- WatanabeAYokoiNKinoshitaSHinoYTsuchihashiYClinicopathologic study of conjunctivochalasisCornea20042329429815084864
- LiuDConjunctivochalasis. A cause of tearing and its managementOphthal Plast Reconstr Surg198622528
- SerranoFMoraLMConjunctivochalasis: a surgical techniqueOphthalmic Surg1989208838842630968
- MellerDTsengSCConjunctivochalasis: literature review and possible pathophysiologySurv Ophthalmol1998432252329862310
- KheirkhahACasasVBlancoGAmniotic membrane transplantation with fibrin glue for conjunctivochalasisAm J Ophthalmol200714431131317659969
- OtakaIKyuNA new surgical technique for management of conjunctivochalasisAm J Ophthalmol200012938538710704560
- NagaiMHatouSOhnoKMochizukiHYamadaMSurgical repair of conjunctivochalasis with anchoring suturesAtarashii Ganka20082515571560
- HaefligerIOVysniauskieneIFigueiredoARPiffarettiJMSuperficial conjunctiva cauterization to reduce moderate conjunctivochalasisKlin Monatsbl Augenheilkd200722423723917458782
- GumusKCrockettCHPflugfelderSCAnterior segment optical coherence tomography: a diagnostic instrument for conjunctivochalasisAm J Ophthalmol201015079880620869039
- KheirkhahACasasVEsquenaziSNew surgical approach for superior conjunctivochalasisCornea20072668569117592317
- SuzukamoYOshikaTYuzawaMPsychometric properties of the 25-item National Eye Institute Visual Function Questionnaire (NEI VFQ-25), Japanese versionHealth Qual Life Outcomes200536516248900
- MangioneCMLeePPPittsJPsychometric properties of the National Eye Institute Visual Function Questionnaire (NEI-VFQ). NEI-VFQ Field Test InvestigatorsArch Ophthalmol1998116149615049823352
- BalcerLJBaierMLKunkleAMSelf-reported visual dysfunction in multiple sclerosis: results from the 25-Item National Eye Institute Visual Function Questionnaire (VFQ-25)Mult Scler2000638238511212133
- GeggelHSFriendJThoftRAConjunctival epithelial wound healingInvest Ophthalmol Vis Sci1984258608636735650
- ChouHShimizuTEndoYTaniTWound healingSurgery Frontier2007145661
- MatsuuraNOkitaKUmemotoMYamamotoSCellular and molecular mechanisms of wound healingSurgery Frontier200310121126
- KashimaTMiuraFAkiyamaHKishiSSimple surgery for conjunctivochalasis using shrinking effect of heat coagulation with biopolar coagulation forcepsAtarashii Ganka201027229233