Abstract
We report a case of neovascularization secondary to Purtscher’s retinopathy that showed minimal improvement with photocoagulation treatment. A 14-year-old boy with a history of cerebellar medulloblastoma presented with blurry vision and floaters after being struck by a motor vehicle while riding his bike. At presentation, visual acuity was 20/400 in his right eye and counting fingers in his left eye. Fundus examination showed disk edema, retinal whitening, and retinal hemorrhages in both eyes. Optical coherence tomography demonstrated thinning of the temporal retina and disruption of the inner segment–outer segment junction of the photoreceptor layer in the right eye and thickening and edema of the nasal macula, as well as a central foveal hyper-reflectivity, in the left eye. At the initial visit, there was no ischemia or neovascularization (NV). One month later, the patient developed NV of the disk and ischemia in the mid-periphery of the left eye. The patient underwent treatment with pan-retinal photocoagulation. The NV regressed, but visual outcome remained poor at his 5-month follow-up visit.
Introduction
Purtscher’s retinopathy was first described in 1910 by Otmar Purtscher in five patients who suffered acute blindness after sustaining severe trauma.Citation1 The patients exhibited multiple areas of retinal whitening in the posterior pole which are now recognized as cotton wool spots. Papillitis, intraretinal hemorrhage, and preretinal hemorrhage were also seen. The severity of visual loss in Purtscher’s retinopathy is typically bilateral and variable. The onset of visual symptoms may be acute or delayed by up to 48 hours. Without treatment, vision usually recovers spontaneously within 1–3 months. The fundus examination may be characterized by mottling of the retinal pigment epithelium, temporal disk pallor, and attenuation or sheathing of the retinal vessels.Citation2 Rarely, neovascularization can occur.Citation3,Citation4
Case report
A 14-year-old boy was referred to the ophthalmology service for new blurry vision and floaters in both eyes. A few days earlier, he had suffered multiple fractures to his face and skull after being struck by a truck while riding his bike. He also had a lacerated liver and pancreas, a small pneumothorax, and a pelvic hematoma. He did not require any surgical intervention. His medical history was significant for cerebellar medulloblastoma that had been treated with surgery, radiation, and chemotherapy 6 years prior to presentation.
Visual acuity was 20/400 in the right eye and counting fingers at 5 feet in the left eye. An afferent pupillary defect was not present. Intraocular pressure was 21 mmHg in the right eye and 19 mmHg in the left eye. Slit lamp examination revealed trace cell in the anterior vitreous in the right eye. Dilated fundus examination revealed disk edema, retinal whitening, and retinal hemorrhages in both eyes (). Optical coherence tomography showed atrophy of the temporal retina and disruption of the inner segment–outer segment junction of the photoreceptor layer in the right eye () with thickening and edema of the nasal macula, and central foveal hyper-reflectivity consistent with a scar in the left eye (). One month later, the right eye was without neovascularization () and the patient was found to have neovascularization of the disk and ischemia in the mid-periphery in the left eye (). He underwent uncomplicated pan-retinal photocoagulation. At the last follow-up, 5 months after his initial presentation, visual acuity had slightly improved to 20/200 in the right eye and 20/300 in the left eye. The neovascularization had regressed (), and he was referred to low vision services.
Figure 1 (A and B) Color fundus photograph montages showing disk edema, diffuse retinal whitening, and retinal hemorrhages more prominent in the left eye compared to the right eye. (C) Optical coherence tomography showing atrophy of the temporal retina and disruption of inner segment–outer segment junction of the photoreceptor in the right eye. (D) Optical coherence tomography revealing edema of the nasal macula and central foveal hyper-reflectivity consistent with a scar in the left eye. (E) Optical coherence tomography thickness map of the right eye demonstrating temporal thinning.
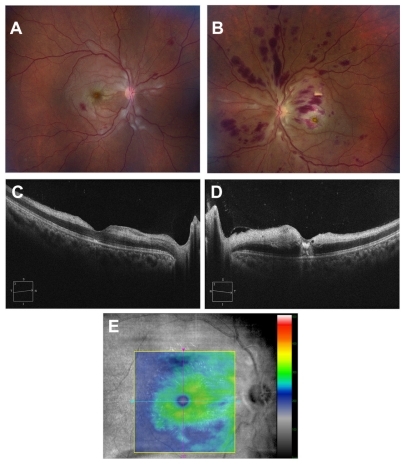
Figure 2 (A) Color photograph and (B) fluorescein angiogram of the right eye 1 month after presentation.
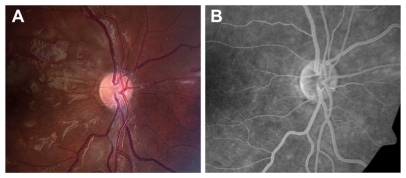
Figure 3 (A) Color photograph of the left eye 1 month after presentation revealing neovascularization of the disk. (B, C and D) Early, mid, and late fluorescein angiograms of the left eye at the same visit demonstrating leakage of the disk consistent with neovascularization. (E) Fluorescein angiogram of the mid-periphery revealing ischemia superonasal to the disk.
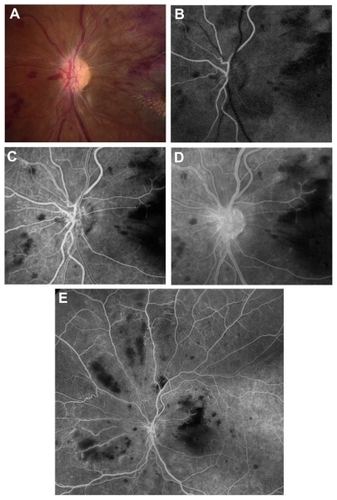
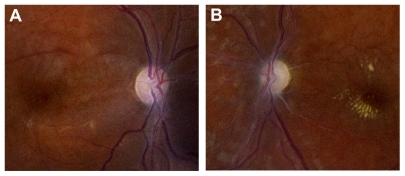
Figure 4 Color photographs of the right (A) and left (B) eyes 5 months after pan-retinal photocoagulation, demonstrating regression of neovascularization of the disk. Optic atrophy and pallor are present.
Discussion
Conditions that can have funduscopic findings similar to Purtscher’s retinopathy include: compressive chest trauma, hydrostatic pressure syndrome, post-traumatic fat embolism from long bone fractures, acute pancreatitis, lupus erythematosis, dermatomyositis, scleroderma, and amniotic fluid embolism.Citation5–Citation7
To our knowledge, this is the first reported case of neovascularization secondary to traumatic Purtscher’s retinopathy treated with panretinal photocoagulation. This case illustrates that retinal ischemia can be severe enough in Purtscher’s retinopathy for neovascularization to occur. Sturm et al described similar findings in two children with hemolytic uremic syndrome, one of whom required laser photocoagulation for bilateral rubeosis irides and neovascularization of the disk.Citation4 Vision was poor as a result of optic atrophy. It is unclear why our patient did not develop neovascularization in both eyes.
The presence of ischemia certainly contributed to poor visual outcome in the left eye of our patient. Optic disk swelling, which was present in both eyes at the time of presentation, has been suggested as a prognostic factor associated with poor outcome and may also help explain the poor visual outcome.Citation2
In conclusion, Purtscher’s retinopathy in the setting of trauma can rarely lead to neovascularization and ischemia. Even with treatment, visual prognosis can be guarded.
Disclosure
The authors report no conflicts of interest in this work.
References
- PurtscherOUnknown findings after head traumaBerl Dtsch Ophthal Ges191036294301 German
- AgrawalAMcKibbin Purtscher’s and Purtscher-like retinopathies: a reviewSurv Ophthalmol200651212913616500213
- PrammerGDisturbances of the retinal vessels as a result of Purtscher’s retinopathy (author’s transl)Klin Monbl Augenheilkd19761686840843 German994390
- SturmVMenkeMNLandauKLaubeGFNeuhausTJOcular involvement in paediatric haemolytic uraemic syndromeActa Ophthalmol201088780480719604154
- KellyJSPurtcher’s retinopathy related to chest compression by safety belts: fluorescein angiographic findingsAm J Ophthalmol19727422782835054237
- BlodiBJohnsonMWGassJDFineSLJoffeLMPurtcher’s-like retinopathy after childbirthOphthalmology19909712165416592087295
- BurtonTCUnilateral Purtcher’s retinopathyOphthalmology19808711109611057243205