Abstract
Purpose
To report the use of intracorneal ring segment (ICRS) implantation in a case of severe corneal thinning and irregularity secondary to alkali burn.
Case report
A 33-year-old man who had a history of ocular alkali burn in the right eye was admitted. His best corrected visual acuity was 0.16 with manifest refraction of +5.00 (–7.00 × 180°). Orbscan II® revealed steepening of >53 D superiorly, excessive thinning inferiorly with thinnest pachymetric reading of 269 μm. Two KeraRing® segments, 200 μm thick and 90° arced, were implanted. During intrastromal channel creation by Intralase®, the inferior half of the applanating cone was covered by a gelatinous paper to prevent the penetration of the laser beam into the anterior chamber. In the first year postoperation, best corrected visual acuity was 0.7 with manifest refraction of +1.50 (–3.50 × 35°). Visante® opticial coherence tomography displayed ICRS at a depth of <370 μm.
Conclusion
ICRS implantation with this novel approach may be an option in eyes with severe corneal irregularity and thinning.
Video abstract
Introduction
The outcome of an ocular alkali burn might range from mild epithelial injury to permanent blindness secondary to destruction of the ocular surface and damage to the intraocular structures.Citation1,Citation2 Once immediate first aid and preventive measures are performed and a quiescent ocular surface with no inflammation is achieved, visual rehabilitation becomes important. Keratoplasty techniques in excessively thinned corneas with limbal stem-cell insufficiency pose unique challenges for surgeons.
Intracorneal ring segments (ICRS) have been used with success in the treatment of primary and secondary corneal ectasia.Citation3–Citation6 However, there have been no reports on their use in eyes that have suffered chemical injury.
Here, the authors report a patient with corneal thinning and irregularity secondary to alkali burn who underwent ICRS implantation using femtosecond laser keratome, with a novel approach to prevent the penetration of laser shoots through the excessively thinned cornea.
Case report
A 33-year-old man was admitted to Turkiye Hospital in April 2008 complaining of decreased vision in his right eye. In September 2002 he had sustained alkaline chemical injury from caustic soda (sodium hydroxide) in this eye. He had suffered from nonprogressive loss of vision since then. At time of admission, his uncorrected visual acuity (UCVA) enabled him to count fingers held up at a distance of 2 m away. His best corrected visual acuity (BCVA) was 0.16 in Snellen lines, with a manifest refraction of +5.00 (–7.00 × 180°). The patient was emmetropic in the left eye, with a UCVA of 1.0. He mentioned that vision in his right eye had been the same as in his left eye before the injury. His medical records from the center where he had received immediate first aid eye care for the management of alkali burn showed that his UCVA and BCVA had remained stable since the injury. The potential visual acuity, assessed by placing a rigid contact lens over his eye, revealed a BCVA of 0.3.
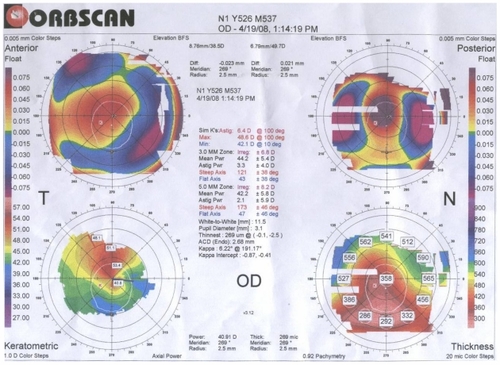
Orbscan® II (Bausch & Lomb, Rochester, NY) topography revealed that severe corneal thinning was present inferiorly with excessive steepening in the superior quadrants. The minimum and maximum simulated K readings were 42.1 D and 48.6 D, respectively; however, steepening in the superior quadrants reached >53 D. The central and thinnest pachymetric readings were 358 μm and 269 μm, respectively, with a reverse keratectasia pattern (). The corneal transparency was not affected centrally, but, as a consequence of localized limbal stem cell deficiency, perilimbal opacification and corneal neovascularization were noted inferiorly. The intraocular pressure was 16 mmHg and fundus examination was unremarkable.
Figure 1 Patient’s preoperative Orbscan II® corneal topography imaging information.
In an attempt to improve the vision, ICRS (KeraRing®, Mediphacos Ltda, Belo Horizonte, Brazil) implantation was planned for the correction of the corneal steepening and irregularity. Two segments with 200 μm thickness and 90° arcs were to be placed temporally and nasally, where corneal thicknesses were greater than 400 μm. The patient was given detailed information about the planned surgery; its possible risks and complications, particularly those that were relevant to his unique corneal characteristics; and possible modifications of the surgical technique. Written informed consent was obtained from the patient before any procedures were performed.
Surgical technique
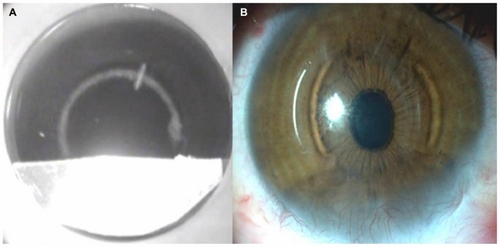
The pachymetric readings were confirmed by ultrasonic pachymetry prior to the surgery. The femtosecond laser keratome (Intralase®, Advanced Medical Optics, Inc, Abbott Park, IL) was used to create intrastromal channels for ICRS at a depth of 370 μm, with inner and outer diameters of 5.0 and 5.6 mm, respectively. A disposable suction ring and an applanation cone were used to stabilize and flatten the cornea to maintain a precise distance from the laser head to the focal point. The pulse duration was 600 fs. The femtosecond laser settings were as follows: entry cut thickness, 1 μm; ring energy, 1.50–2.50 μJ; and entry cut energy 1.50 μJ. Since the inferior cornea was thinner than the depth of the planned intrastromal channels, a novel technique had to be developed to prevent the penetration of the femtosecond laser beam into the anterior chamber. Thus, a piece of gelatinous paper was placed into the applanation cone of the femtosecond laser, at the area corresponding to the extremely thin inferior segment, which prevented the femtosecond laser beam from passing through. In this way, a C-shaped intrastromal channel with an inferior opening was created instead of a full circle (). This allowed the implantation of the ICRS as in routine procedures with no additional technical difficulties, while protecting the anterior segment structures inferiorly (see Supplementary video, available here).
Figure 2 (A) Intraoperative image of intrastromal channel creation with femtosecond laser; inferior half of the cone was covered by a gelatinous paper. (B) Postoperative first-month slit-lamp image of the cornea showing the inferiorly thin and vascularized cornea and temporal and nasal placement of the intracorneal ring segments.
Postoperatively, topical ofloxacin 0.3% (Exocin®; Allergan, Mougins, France) four times daily and prednisolone acetate 1% eye drops (PredForte®; Allergan, Mougins, France) four times daily were used for 1 week. The steroid eye drop was tapered over 3 weeks. Preservative-free artificial tear (Refresh plus®; Allergan, Irvine, CA, USA) eye drops were used as needed.
Postoperative course
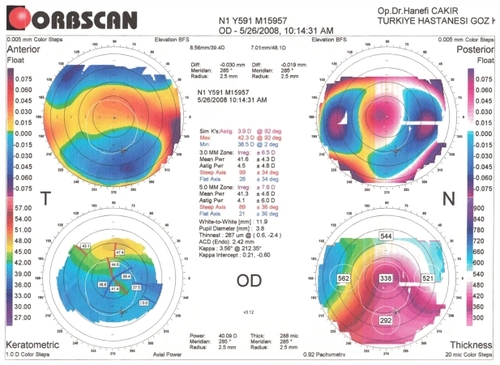
In his examination 1 month postoperation, the patient’s UCVA was 0.05 and his BCVA had improved to 0.6 with a manifest refraction of +3.00 (–4.50 × 45°). Slit-lamp examination revealed well-centered intracorneal rings with no migration or inflammatory reaction (). In Orbscan II® topography, minimum and maximum simulated K readings were 42.3 D and 38.5 D, respectively (). Visante® (Carl Zeiss Meditec Inc, Dublin, CA) anterior segment optical coherence tomography displayed that the intrastromal channels were created at a depth of <370 μm. No signs of damage to the anterior segment structures were noted.
Figure 3 Patient’s postoperative Orbscan II® corneal topography imaging information.
In his examination at 1 year postoperation, his UCVA was 0.1 and BCVA was 0.7, with a manifest refraction of +1.50 (–3.50 × 35°) in the operated eye.
Discussion
Eyes affected by alkali burn are often complicated by limbal stem-cell insufficiency and dry eye, persistent epithelial defects, stromalysis, and even perforation.Citation7–Citation9 Penetrating keratoplasty (PK) poses technical difficulties in these eyes due to irregularly thinned corneas and high risk for graft rejection due to stem-cell insufficiency, corneal neovascularization, and dry eye. Corneal grafting should be deferred until a healthy ocular surface with no inflammation is achieved. ICRS implantations have been successfully implemented for the rehabilitation of primary corneal ectasias such as keratoconus and pellucid corneal marginal degenerationsCitation3,Citation4,Citation6 and iatrogenic postrefractive surgery corneal ectasias.Citation5,Citation6 However, there have been no reports on their use in alkali burn corneas.
The patient discussed here had been scheduled for PK in another clinic when he was first seen by the authors for a second opinion. Having high-risk characteristics for corneal graft rejection, the authors recommended a trial for intracorneal ring surgery, which would not rule out future PK in the case of an unsuccessful outcome. To achieve the maximum improvement in astigmatism in the central optic zone of the cornea, ICRS with smaller inner diameter were selected for implantation (ie, KeraRing®, Mediphacos). The thickness of the rings and depth of intracorneal channels were selected using the nomogram provided by the manufacturer. Given the high amount of astigmatism, implantation of two rings along the horizontal axis was planned. The second-line strategy would be placing one ring superiorly; however, the amount of cylinder that is expected to be corrected with that technique is low.
The femtosecond laser was used to create the intracorneal channels in this case, since it was of paramount importance that they be created at uniform intracorneal depth. During manual intracorneal channel formation in such an injured cornea, epithelial disturbance and associated stromal edema can be inevitable and posterior corneal perforation the worst complication.Citation6 In this case, it was aimed to arrest the laser shoots in the thinnest areas of the cornea, where the anterior chamber structures could have been affected. For this purpose, the region of the cone that corresponded to the inferior thinned segment of the cornea was covered by gelatinous paper. The gelatinous paper is covered with aluminium foil, which is used in the industry due to its resistance and protection performance for femtosecond laser illumination,Citation10 the beam of which can travel in the transparent media and cause destruction to the tissue at a focused plane of predetermined distance, unlike the 196 nm excimer laser beam, which ablates the tissue it faces within a range of distances.
A C-shaped intracorneal channel, rather than a full circle, allowed the implantation of the intracorneal rings. Creating individual channels separately would have been harder to accomplish due to the technical difficulties in placing them at a regular distance from each other around the pupil, at different applications of the femtosecond laser cone. Therefore, it was aimed to create a C-shaped channel in a single attempt for full-circular intrastromal channel.
Postoperatively, increased regularity of the central optic zone of the cornea with reduced irregular astigmatism led to subsequent improvement in the BCVA, to the level that might never be achieved after PK on such an irregular ocular surface. This relatively noninvasive method of optical correction also avoided the healing problems of graft failure/ rejection and frequent follow-up visits.
In cases with irregular corneal surface due to chemical injury, it is important to perform manual ultrasonic pachymetry prior to surgery to confirm Orbscan readings, which can be inaccurate when corneal opacities are present. Additionally, these cases should be carefully followed up, as corneal neovascularization and stromal inflammation or melting can be stimulated by ICRS implantation even in normal eyes, and might be more likely in an eye with lasting damage from a chemical burn, even when the segments are placed away from the area of most severely injured cornea.
In conclusion, ICRS implantation might be an option for the management of corneal irregularities secondary to ocular surface problems, if special consideration is given and required preventive measures are taken according to the thickness of the cornea in the region of the femtosecond laser beam.
Disclosure
The study was presented at the 42nd National Meeting of Turkish Ophthalmology Society in Antalya, Turkey, in November 2008.
The authors do not have any financial or proprietary interests in any of the devices mentioned in this manuscript. There has been no public or private support in the conduct of this study.
References
- BrodovskySCMcCartyCASnibsonGManagement of alkali burns: an 11-year retrospective reviewOphthalmology2000107101829183511013181
- BagleyDMCastertonPLDresslerWEProposed new classification scheme for chemical injury to the human eyeRegul Toxicol Pharmacol200645220621316764976
- ZareMAHashemiHSalariMRIntracorneal ring segment implantation for the management of keratoconus: safety and efficacyJ Cataract Refract Surg200733111886189117964393
- AkaishiLTzelikisPFRaberIMFerrara intracorneal ring implantation and cataract surgery for the correction of pellucid marginal corneal degenerationJ Cataract Refract Surg200430112427243015519101
- WoodwardMARandlemanJBRussellBLynnMJWardMAStultingRDVisual rehabilitation and outcomes for ectasia after corneal refractive surgeryJ Cataract Refract Surg200834338338818299061
- CarrasquilloKGRandJTalamoJHIntacs for keratoconus and post-LASIK ectasia: mechanical versus femtosecond laser-assisted channel creationCornea200726895696217721296
- HughesWFJrAlkali burns of the eye; review of the literature and summary of present knowledgeArch Ophthalmol194635423426
- HughesWFJrAlkali burns of the eye; clinical and pathologic courseArch Ophthalmol194636189214
- Roper-HallMJThermal and chemical burnsTrans Ophthalmol Soc U K1965856316535227208
- MartinSKrügerJHertwigAFiedlerAKautekWFemtosecond laser interaction with protection materialsAppl Surf Sci2003208–209333339