Abstract
Purpose
To evaluate the effect of the shape of Bowman probes on the success of primary probing for congenital nasolacrimal duct obstruction.
Materials and methods
Records of 42 nasolacrimal duct obstructions in 37 children who underwent probing with straight Bowman probes (group A) and 128 nasolacrimal duct obstructions in 110 children who underwent probing with Bowman probes manually bent to mimic the natural curve of the bony nasolacrimal pathway (group B) were evaluated and compared. All children were under 2 years of age. The main outcome was successful probing. Successful probing was defined as a complete resolution of signs and symptoms.
Results
The mean age of the patients was 16.4 ± 4.1 months (range 8–24 months) in group A and 16.8 ± 4.2 months (range 7–24 months) in group B. No canalicular or nasolacrimal sac pathologies were diagnosed during probing. The success rate was 76.2% (32/42) in group A and 91.4% (117/128) in group B. The difference was statistically significant (P < 0.01).
Conclusion
Manually curved probes can be used efficiently during probing and increase the success rates.
Introduction
Congenital nasolacrimal duct obstruction (CNLDO) is a major problem of the nasolacrimal system in infancy and childhood.Citation1 An embryological membrane obstructs the distal end of the nasolacrimal duct (NLD) in most cases, and patients present with epiphora and discharge.Citation2 Most cases resolve spontaneously or with lacrimal massage in the first year of life.Citation3,Citation4 If the condition persists, most authors agree that NLD probing is the most effective treatment modality with high success rates in or around the first year of life.Citation5 Surgical techniques and tools chosen by different surgeons during probing may affect the results of probing and have not yet been studied. Some surgeons use straight Bowman probesCitation6 and some suggest curved Bowman probes to mimic the curve of the bony nasolacrimal pathway in children.Citation7
The aim of this study was to evaluate the effect of the shape of Bowman probes on the success rate of initial probing for CNLDO in children < 2 years of age.
Material and methods
The current study is a retrospective, interventional study. Group A comprised 42 CNLDOs in 37 children who underwent probing with straight Bowman probes (Katena Products, NJ, USA) and group B comprised 128 CNLDOs in 110 children who underwent probing with Bowman probes (size one) manually bent approximately 15 degrees to mimic the natural curve of the bony nasolacrimal pathway between January 2007 and March 2011. The diagnosis of CNLDO was based on a history of epiphora and discharge since the first months of life and delayed fluorescein disappearance time. A detailed ophthalmological examination was performed to eliminate any other ophthalmological problem which may cause epiphora such as congenital glaucoma, trichiasis, conjunctivitis, keratitis, and metabolic disorders. Patients < 2 years of age were included in the study. Patients with congenital craniofacial and lid abnormalities, punctal agenesis, a history of trauma, nasolacrimal surgery, previous probing or other nasolacrimal intervention, and postoperative follow-up <3 months were excluded from the study.
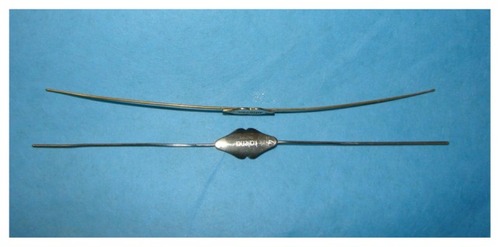
Written informed consent was obtained from the patients’ families preoperatively. The tenets of the Declaration of Helsinki were followed in the study. All patients underwent primary probing under general anesthesia. In group A, straight Bowman probes (Katena Products) were used; in group B, Bowman probes gently curved to mimic the bony nasolacrimal pathway were used (). The surgeon dilated both puncta with a fine punctal dilator (Infant lacrimal dilator, Katena Products). The probe was inserted through the upper punctum into the ampulla of the upper canaliculus and then rotated horizontally to fit in the canaliculus. Lateral traction was applied to the eyelid to prevent kink formation. After a “hard stop” was felt, the probe was slightly retracted and rotated 90 degrees. At this point, in group A, the straight Bowman probe was directly advanced toward the NLD; in group B, the curve of the probe was turned posteriorly and medially while advancing toward the NLD.Citation7 After a popping sensation was felt, passage into the nose was confirmed by metal-to-metal contact under the inferior turbinate with another probe. The same procedure was repeated from the lower punctum to exclude any lower canalicular obstruction. After the operation, all patients received a topical steroid and antibiotic treatment four times daily for 10 days and a nasal decongestant for 5 days. The patients were evaluated at 1 week, 1 month, and 3 months. A fluorescein disappearance test was repeated at 3 months. Successful probing was defined as a complete resolution of signs and symptoms at 3 months postoperatively. The chi-squared test was used for the comparison of success rates. P < 0.05 was considered statistically significant.
Figure 1 Manually bent Bowman probes to mimic the natural curve of the nasolacrimal duct in children.
Results
The mean age of the patients was 16.4 ± 4.1 months (range 8–24 months) in group A and 16.8 ± 4.2 months (range 7–24 months) in group B. Both groups were similar regarding age characteristics. No canalicular or nasolacrimal sac pathologies were diagnosed during probing. The success rate was 76.2% (32/42) in group A and 91.4% (117/128) in group B. The difference was statistically significant (P < 0.01).
Discussion
NLD probing is an effective therapeutic procedure in the management of CNLDO; however, different success rates were reported in the same age groups by different authors. Limbu et al reported a success rate of 90.2% in a group of children < 2 years of age;Citation8 however, Repka et al reported a success rate of 78% in children 6–12 months of age and 79% in children 12–24 months of age.Citation9 In children > 2 years of age, success rates of probing is much more controversial. Robb reported that the success rate of probing was 94.5% in patients aged ≥ 2 years.Citation10 In contrast, in Sturrock et al’s study the success rate was 42% in patients probed after 2 years of age and Young et al reported a cure rate of 54% in the same age group.Citation11,Citation12 The reason for the different success rates reported previously is unclear. Some authors performed simple NLD probing and some combined probing with inferior turbinate fracture.Citation11,Citation13 Nasal endoscopy was also used in some studies.Citation6,Citation14 Patient characteristics may affect the surgical results of probing.Citation15 Additionally, the anatomy of NLD, surgical techniques, and tools chosen by different surgeons during probing may affect the results of probing and have not yet been studied.
In children, the NLD slopes downwards medially and posteriorly.Citation7 Some surgeons use straight Bowman probes and some suggest gentle recontouring of the probe to suit the configuration of the bony nasolacrimal pathway in children;Citation6,Citation7 however, no comparative studies have been conducted yet. In this study, probing with manually curved Bowman probes was performed in 110 children and the results compared with those performed by the same surgeons with straight probes before October 2008.
For effective probing, an ophthalmologist must pass the probe through the bony nasolacrimal canal and perforate the embryological membrane without traumatizing other anatomical structures or creating a false passage. In the current study, a complete resolution of signs and symptoms was achieved in 76.2% of eyes with a straight Bowman probe and in 91.4% of eyes with a curved Bowman probe and the difference was statistically significant (P < 0.01). In children, the slope of the NLD may make it difficult to pass a straight Bowman probe through the NLD without trauma. Strenuous attempts to pass a straight Bowman probe through a curved NLD may cause mucosal damage, submucosal passage, and synechia formation in the duct. In group B, the Bowman probe was gently bent to mimic the curve of the bony nasolacrimal pathway, as suggested by Robb.Citation7 This may lead to an easy introduction of the probe into the duct, and advancement through the duct without rubbing and traumatizing the mucosa or the bony structures of the canal may be possible and this may be the reason of the high success rate of probing with recontoured probes.
Some authors classify CNLDO into two main groups – membranous and complex (firm) – based on the sensation while passing the Bowman probe.Citation16 If the passage of the probe produces a popping sensation with subsequent free passage, it is called a membranous obstruction and if the passage of the probe produces a bony sensation similar to passing the probe through sandpaper, it is called a complex (firm) obstruction. However, this classification is subjective and depends on the feeling during probing and different rates of obstruction types were reported in the same age groups by different authors.Citation17,Citation18 The medially and posteriorly directed NLD can make it difficult to pass a straight Bowman probe through the NLD in children. Therefore, it may be a misdirected Bowman probe that produces the bony sensation, which might result in a membranous obstruction being misdiagnosed as a firm or complex obstruction. This may be one of the reasons for the controversy that exists regarding the rates of obstruction types and the outcomes in different studies. With a curved Bowman probe, the probability of misdirection and false passage formation may be reduced and success rates of probing may be increased.
Conclusion
According to the results, using a curved Bowman probe in children with CNLDO is more effective in the management of CLNDO than a straight probe. Curved probes that mimic the slope of the NLD can be used efficiently during probing. Production and usage of tools that mimic the NLD anatomy also for silicone intubation or balloon dacryocystoplasty may be taken into consideration for possible higher success rates. Anatomical studies of the nasolacrimal system in children are required to further evaluate the effectiveness of surgical techniques and tools used for the management of CLNDO.
Disclosure
The authors report no conflicts of interest in this work.
References
- GuerryD3rdKendigELJrCongenital impotency of the nasolacrimal ductArch Ophthalmol194839193204
- KashkouliMBBeigiBParvareshMMKassaeeATabatabaeeZLate and very late initial probing for congenital nasolacrimal duct obstruction: what is the cause of failure?Br J Ophthalmol20038791151115312928286
- Pediatric Eye Disease Investigator GroupResolution of congenital nasolacrimal duct obstruction with nonsurgical managementArch Ophthalmol2012130673073422801833
- NucciPCapoferriCAlfaranoRBrancatoRConservative management of congenital nasolacrimal duct obstructionJ Pediatr Ophthalmol Strabismus198926139432915312
- KatowitzJAWelshMGTiming of initial probing and irrigation in congenital nasolacrimal duct obstructionOphthalmology19879466987053627719
- KouriASTsakanikosMLinardosENikolaidouGPsarommatisIResults of endoscopic assisted probing for congenital nasolacrimal duct obstruction in older childrenInt J Pediatr Otorhinolaryngol200872689189618440076
- RobbRMPediatric lacrimal surgeryAlbertDMOphthalmic Surgery: Principles and TechniquesHoboken, NJWiley-Blackwell199910151023
- LimbuBAkinMSaijuRAge-based comparison of successful probing in Nepalese children with nasolacrimal duct obstructionOrbit2010291162020302404
- RepkaMXChandlerDLBeckRWPrimary treatment of nasolacrimal duct obstruction with probing in children younger than 4 yearsOphthalmology2008115357758417996306
- RobbRMSuccess rate of nasolacrimal duct probing at time intervals after 1 year of ageOphthalmology19981057130713099663238
- SturrockSMMacEwanCJYoungJDLong-term results after probing for congenital nasolacrimal duct obstructionBr J Ophthalmol199478128928947819169
- YoungJDMacEwanCJOgstanSACongenital nasolacrimal duct obstruction in second year of life: a multicenter trial of managementEye (Lond)199610Pt 44854918944104
- HavinsHEWilkinsRBA useful alternative to slicone intubation in congenital nasolacrimal duct obstructionsOphthalmic Surg1983148660670
- ElmorsySShabanaYKFayekHMEndoscopic assisted probing for symptomatic congenital nasolacrimal ductablet obstruction after one year of ageRhinology201048110010321480567
- Al-FakyYHAl-SobaieNMousaAEvaluation of treatment modalities and prognostic factors in children with congenital nasolacrimal ductobstructionJ AAPOS2012161535722370666
- MaheshwariRMaheshawriSLate probing for congenital nasolacrimal duct obstructionJ Coll Physicians Surg Pak2007171414317204219
- ChenPLHsiaoCHBalloon dacryocystoplasty as the primary treatment in older children with congenital nasolacrimal duct obstructionJ AAPOS20059654654916414521
- MaheshwariRSuccess rate and cause of failure for late probing for congenital nasolacrimal duct obstructionJ Pediatr Ophthalmol Strabismus200845316817118524195