Abstract
The original technique of staining the anterior capsule of the lens with Trypan blue involves the injection of an air bubble in the anterior chamber. A drawback of this technique is the possible instability of the anterior chamber caused by the sudden exit of air when the dye is injected with the cannula through the side-port incision. Other staining techniques that use viscoelastic substances to increase the stability of the anterior chamber and to dose the injected dye have been described. The authors present an under-air staining technique of the anterior capsule using one drop of Trypan blue injected with a 30 G needle through the peripheral cornea. This procedure prevents the air bubble from escaping the anterior chamber and allows fast and selective staining of the capsule.
Introduction
The original technique of staining the anterior capsule with Trypan blue (TB) in eyes with no red reflex involves the injection of the dye with a cannula after filling the anterior chamber with an air bubble.Citation1 The stability of the anterior chamber can be compromised by air escaping when the cannula is introduced and the dye is injected. Moreover, the superficial tension of air bubble and capillary action between TB and the metal cannula can force the dye to build up within the aqueous meniscus surrounding the air bubble, making selective staining of the capsule difficult. Several techniques using viscoelastic substances as an alternative to air have been presented to increase the stability of the anterior chamber.Citation2–Citation5 However, staining under viscoelastic material can be time-consuming and expensive, as it requires the mechanical spreading of TB onto the anterior capsule and the replacement of the viscous solution when an excessive diffusion of dye affects its transparency.
We present an under-air staining technique of the anterior capsule using one drop of TB injected with a 30 G needle through the peripheral cornea. Our procedure prevents the exit of air during the injection of the dye, resulting in increased stability of the anterior chamber. Moreover, it allows selective staining of the capsule using the needle and avoids an excessive buildup of TB in the anterior chamber.
Technique
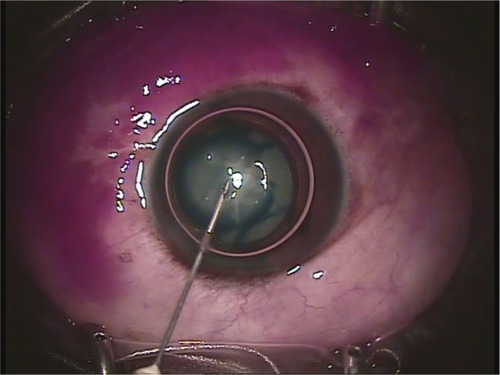
Connect a 30 G needle to a 2.25 mL Luer Lock syringe containing Trypan blue 0.06% (VisionBlue; Dutch Ophthalmic Research Center International, Zuidland, Netherlands). Make a standard side-port incision with a 15° blade. Use a 25 G cannula connected to a 5 mL syringe to inject a big air bubble in the anterior chamber. Introduce the 30 G needle bevel-up in the anterior chamber through the peripheral cornea between the side-port incision and the site chosen for the corneal tunnel. Push the needle forward in the air bubble right between the anterior capsule and posterior corneal surface until the tip reaches the center of the pupil. Unlike what occurs using a cannula, the air cannot escape from the anterior chamber. Inject gently, allowing the TB volume to grow within the needle bevel (). Rotate the syringe 90°, letting the drop fall on the anterior capsule (). The needle tip allows precise control on the injected dye, similarly to a dropper. If the staining is not sufficient, it is possible to inject one more drop of TB on the unstained area. Once the needle is removed, the perforation will close spontaneously in a few seconds, and if necessary an absorbent stick can be used to stop tiny leakages of air and/ or dye. Inject viscoelastic substance in the anterior chamber through the side-port incision, allowing the air and the leftover dye to exit the eye. Perform a standard capsulorhexis.
Figure 1 Air-filled anterior chamber with a Trypan blue drop held in the bevel of the needle.
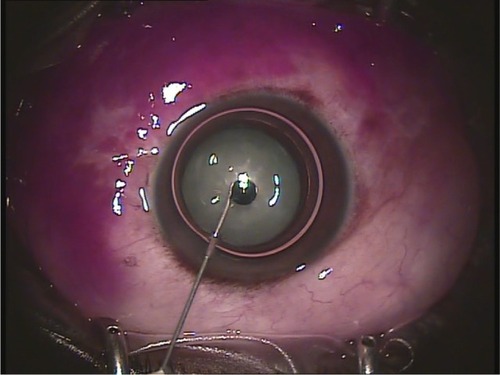
Figure 2 The tension surface of the air bubble spreads the dye on the anterior capsule.
Discussion
TB is the most used dye to perform capsulorhexis in eyes with no red reflex.Citation6 The main staining techniques involve TB injection under air,Citation1 under viscoelastic material,Citation2–Citation5 or directly under aqueous humor.
An air bubble within the anterior chamber reduces the contact between the dye and the corneal endothelium and allows the delivery of undiluted TB onto the anterior capsule. However, the air bubble makes the anterior chamber unstable and prone to collapse when the cannula is introduced to inject the dye. In such an event, the anterior chamber has to be reinflated, thus increasing the duration of surgery. Moreover, sudden reductions in volume of the anterior chamber can cause narrowing of the pupil and damage to the corneal endothelium. To prevent the air bubble from escaping the anterior chamber, it has been proposed that a small amount of high-density viscoelastic material be placed near the side-port incision.Citation7
In our technique, we inject the dye in the anterior chamber, introducing a 30 G needle through the peripheral cornea. In this way, the air cannot escape from the side-port incision, as often occurs when a cannula is used. Once the needle is pulled out, the corneal perforation spontaneously closes in a few seconds.
When the dye is injected with a blunt cannula through the side-port incision, the superficial tension of the air bubble spreads the dye into the thin liquid layer between the air and the anterior capsule.Citation8 In this phase, a meniscus of TB forms between the metal cannula and the anterior capsule due to the capillary action and adhesive forces. To obtain the right staining, the anterior capsule must be swept thoroughly with the cannula, allowing the meniscus of TB to contact the largest possible area. If too much dye is injected, it can migrate back between the cannula and the capsule, escaping from the paracentesis, or it could build up in the aqueous meniscus surrounding the air bubble. To avoid this, Toprak et alCitation8 modified a cannula by bending it to increase the surface contact between the dye and the capsule. In our procedure, we use a very sharp-tipped needle, which reduces the adhesive forces with TB and allows the drop of dye to fall easily over the anterior capsule.
Many authors have described alternative staining techniques based on viscoelastic substances instead of air.Citation2–Citation5 These techniques have the advantage of making the anterior chamber more stable and of better dosing the amount of injected dye. However, when the anterior chamber is filled with viscoelastic substance, it is difficult to deliver the dye onto the capsule. The surgeon has to mechanically spread the dye on the largest possible surface of the capsule, and at times the dyed viscoelastic material or pockets of dye can affect the visibility of the capsule beneath. To avoid these problems, special cannulae have been proposed.Citation2,Citation4 Rarely, an exchange of the viscoelastic material is needed to restore the transparency before the capsulorhexis.
We injected TB with a 30 G needle in seven consecutive patients with white cataract and normal anterior chamber depth. In this small group of patients, we have not observed intra- or postoperative complications. After surgery, all patients showed marked improvement in their visual acuity. In six patients, we performed a regular capsulorhexis after injecting only one drop of dye. In a single patient, one more drop of TB had to be injected to build up the staining of the capsule.
An additional corneal access and a sharp needle in the anterior chamber are the major disadvantages of our technique. In eyes with shallow anterior chamber or with excessive posterior pressure, the use of the 30 G needle technique could be dangerous and should be avoided.
In conclusion, in a small series of seven patients, the staining of the anterior capsule using TB under air with a 30 G needle allowed for enhanced stability of the anterior chamber and the use of the smallest quantity of dye. Our technique has been shown to be safe and successful. Further studies are needed to fully investigate its advantages over the standard procedure.
Disclosure
The authors report no conflicts of interest in this work.
References
- MellesGRJde WaardPWTPameyerJHBeekhuisWHTrypan blue capsule staining to visualize the capsulorhexis in cataract surgeryJ Cataract Refract Surg199925799888070
- KhokharSPangteyMSPandaASelthiHSPainting technique for staining the anterior lens capsuleJ Cataract Refract Surg20032943543612663002
- YetikHDevranogluKOzkanSDetermining the lowest trypan blue concentration that satisfactorily stains the anterior capsuleJ Cataract Refract Surg20022898899112036641
- MarquesDMVMarquesFFMOsherRHThree-step technique for staining the anterior lens capsule with indocyanine green or trypan blueJ Cataract Refract Surg200430131614967263
- CaporossiABalestrazziAAlegenteMCaspriniFCaporossiTTrypan Blue staining of the anterior capsule: the one-drop techniqueOphthalmic Surg Lasers Imaging20053643243416238046
- JacobsDSCoxTAWagonerMDAriyasuRGKarpCLCapsule staining as an adjunct to cataract surgery: a report from the American Academy of OphthalmologyOphthalmology200611370771316581432
- PandeySKWernerLEscobar-GomezMRoig-MeloEAAppleDJDye-enhanced cataract surgery. Part 1: Anterior capsule staining for capsulorhexis in advanced/white cataractJ Cataract Refract Surg2000261052105910946199
- ToprakABErkinEFGulerCTrypan blue staining of the anterior capsule under an air bubble with a modified cannulaOphthalmic Surg Lasers Imaging20033423623812757103