Abstract
Central retinal vein occlusion (CRVO) is frequent in patients with systemic lupus erythematosus (SLE), but the treatment of the macular edema with this disease is extremely difficult. We report a case of cystoid macular edema (CME) secondary to unilateral CRVO in a patient with SLE that responded to intravitreous injection of an anti-vascular endothelial growth factor (VEGF) agent. A 33-year-old Japanese woman was referred to our department with unilateral impairment of vision. Microperimetry (MP-1) showed a cessation of foveal sensitivity. Fluorescein angiography showed CME without ischaemia of the macular region or peripheral retina (nonischemic CRVO). A diagnosis of CME and unilateral nonischemic CRVO combined with SLE was made and intravitreous anti-VEGF therapy was given. A sample of aqueous humor was harvested at the start of intravitreous injection after obtaining informed consent. Then the levels of VEGF and monocyte chemotactic protein (MCP)-1 were measured in the aqueous humor by enzyme-linked immunosorbent assay, revealing that VEGF was 234 pg/mL and MCP-1 was 501 pg/mL. Two weeks later, left eye vision improved to 20/20. Optical coherence tomography (OCT) showed considerable amelioration of retinal swelling and CME. MP-1 showed a marked increase of foveal sensitivity. However, she had recurrence of edema 3 months later. After harvesting aqueous humor again, intravitreous injection of an anti-VEGF agent was repeated for CME. The aqueous VEGF and MCP-1 levels were 156 pg/mL and 360 pg/mL, respectively. These findings suggest that inflammation was improved by intravitreous injection of bevacizumab. Intravitreous injection of anti-VEGF agents may be effective for CME due to nonischemic CRVO in SLE patients if their inflammatory factor levels are low.
Introduction
Systemic lupus erythematosus (SLE) is a chronic autoimmune disorder that affects multiple organs, including the eye.Citation1 Ocular symptoms are usually due to retinal vascular manifestations of this disease, such as central retinal vein occlusion (CRVO), which is frequent in patients with SLE.Citation2 We report an SLE patient with macular edema and unilateral CRVO who responded to intravitreous injection of an anti-vascular endothelial growth factor (VEGF) agent.
Materials and methods
Laboratory test results confirmed the diagnosis of SLE, and revealed leukopenia together with elevation of antinuclear antibody (ANA) and anti-double-stranded DNA antibody (anti-dsDNA). Antiphospholipid antibodies (both anticardiolipin and lupus anticoagulant) were negative. Serology for syphilis, human immunodeficiency virus 1 and 2, and hepatitis B and C was negative. Blood cultures showed no growth. Urinalysis was within normal limits. Magnetic resonance imaging of the central nervous system (CNS) revealed findings compatible with the diagnosis of CNS vasculitis.
Treatment of cystoid macular edema (CME) was started with intravitreous injection of an anti-VEGF agent (bevacizumab, 1.25 mg/0.05 mL). A sample of undiluted aqueous humor was harvested at the start of intravitreous anti-VEGF therapy after informed consent was obtained following an explanation of the purpose and potential adverse effects of the procedure. This study was performed in accordance with the Helsinki Declaration of 2008 (sixth revision), and our institutional review board of Tokyo Women’s Medical University also approved the protocol for collection of aqueous humor. The levels of VEGF and monocyte chemotactic protein-1 (MCP-1) were measured in the aqueous humor sample by using enzyme-linked immunosorbent assay kits for human VEGF and MCP-1 (R&D Systems, Minneapolis, MN, USA).Citation3 As a result, the VEGF level was 234 pg/mL and the MCP-1 level was 501 pg/mL.
Case report
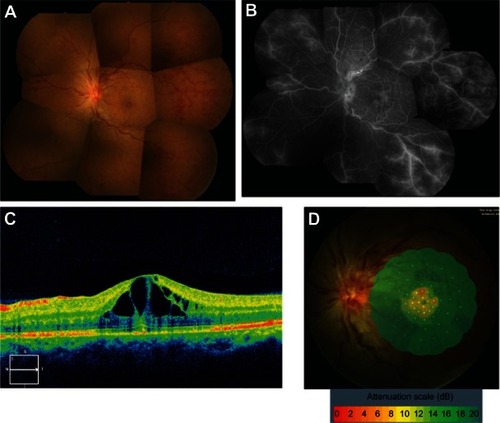
A 33-year-old Japanese woman was referred to our department with unilateral impairment of vision. Six months earlier, SLE was diagnosed on the basis of a malar rash, polyarthritis, leukopenia, and elevation of ANA and anti-dsDNA antibody.Citation1 At the initial examination, visual acuity (VA) was 20/100 in the left eye. Superficial and deep intraretinal hemorrhages were scattered throughout the retina, suggesting that the patient had CRVO (). Fluorescein angiography showed CME without ischemia of the macular region or peripheral retina (). Optical coherence tomography (OCT) identified retinal swelling and CME (). Fundus-monitored microperimetry with the MP-1 system (Nidek, Gamagori, Japan) revealed a cessation of foveal sensitivity ().
Figure 1 Fundus color photograph (A) of our patient with systemic lupus erythematosus, showing unilateral central retinal vein occlusion. Superficial and deep intraretinal hemorrhages are scattered throughout the retina. Fluorescein angiogram (B) shows a pattern resembling cystoid macular edema (CME) without ischemia of the macula or the peripheral retina. Optical coherence tomography (C) reveals retinal swelling and CME. Fundus-monitored microperimetry with the MP-1 system (D) indicates a cessation of foveal sensitivity.
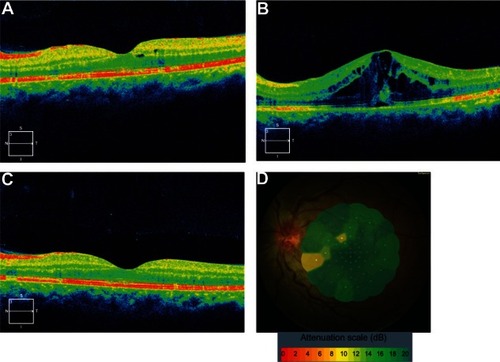
Two weeks later, VA of the left eye had improved to 20/20. OCT showed marked alleviation of retinal swelling and CME (). However, recurrence of edema was noted after 3 months () and VA of the left eye decreased to 20/50. After harvesting aqueous humor, intravitreous injection of bevacizumab (1.25 mg/0.05 mL) was performed again for CME. Levels of VEGF and MCP-1 were 156 pg/mL and 360 pg/mL, respectively. The VA of the left eye improved to 20/20 again, while OCT showed marked alleviation of retinal swelling and CME at one week after the second intravitreous injection (). In addition, there was improvement of foveal sensitivity (). During the subsequent 6 months, there was no recurrence of CME.
Figure 2 Optical coherence tomography (OCT) (A) shows marked improvement of retinal swelling and cystoid macular edema (CME) at 2 weeks after the first intravitreous injection of bevacizumab. OCT (B) reveals the recurrence of macular edema at 3 months after intravitreous anti-vascular endothelial growth factor (VEGF) therapy. OCT (C) displays marked improvement of retinal swelling and CME at 1 week after the second intravitreous injection of bevacizumab. Fundus-monitored microperimetry with the MP-1 system (D) demonstrates improvement of foveal sensitivity.
Discussion
Retinal vascular changes are frequent in patients with SLE.Citation2 The classic retinal findings are hemorrhages and cotton wool spots and VA is generally unaffected. If macular edema occurs, however, it leads to visual impairment. In the present patient, visual acuity, retinal sensitivity, and macular edema were all improved by two intravitreous injections of an anti-VEGF agent (bevacizumab). VEGF decreased from 234 to 156 pg/mL after the first injection and MCP-1 also decreased from 501 to 360 pg/mL. This finding is supported by the report that changes of VEGF after intravitreous anti-VEGF therapy significantly associated with changes of MCP-1,Citation4 and it suggests that inflammation was improved by intravitreous injection of bevacizumab. It has been reported that anti-VEGF treatment is more effective for nonischemic CRVO than ischemic CRVO,Citation5 and we previously reported that aqueous VEGF levels are significantly higher in patients with ischemia than in those without ischemia.Citation6 The present patient had nonischemic CRVO with relatively low levels of VEGF (234 pg/mL and 156 pg/mL), which means that she was more likely to respond to intravitreous anti-VEGF therapy.
Conclusion
These findings suggest that inflammation was improved by intravitreous injection of bevacizumab. Intravitreous anti-VEGF therapy may be effective for CME due to nonischemic CRVO in SLE patients with low levels of inflammatory factors.
Disclosure
Authors report no conflicts of interest in this work.
References
- TanEMCohenASFriesJFThe 1982 revised criteria for the classification of systemic lupus erythematosusArthritis Rheum19822511127112777138600
- ArevaloJFLowderCYMuci-MendozaROcular manifestations of systemic lupus erythematosusCurr Opin Ophthalmol200213640441012441845
- NomaHMimuraTEguchiSAssociation of inflammatory factors with macular edema in branch retinal vein occlusionJAMA Ophthalmol2013131216016523411880
- FunkMKriechbaumKPragerFIntraocular concentrations of growth factors and cytokines in retinal vein occlusion and the effect of therapy with bevacizumabInvest Ophthalmol Vis Sci20095031025103219060280
- KriechbaumKMichelsSPragerFIntravitreal Avastin for macular oedema secondary to retinal vein occlusion: a prospective studyBr J Ophthalmol200892451852218211942
- NomaHFunatsuHMimuraTHarinoSSoneTHoriSIncrease of vascular endothelial growth factor and interleukin-6 in the aqueous humour of patients with macular oedema and central retinal vein occlusionActa Ophthalmol201088664665119563372